Page 16 of 23
EN4.15 | Eustachian Tube Disorders — SDL Guide
Learning Objectives
- Describe the anatomy of the Eustachian tube including its two portions, the opening mechanism, and the differences between the adult and child tube
- Distinguish obstructive Eustachian tube dysfunction from patulous (abnormally patent) Eustachian tube dysfunction based on history, examination, and investigations
- Describe the clinical features, investigations, and management of obstructive ET dysfunction and patulous ET
- Explain the relationship between ET dysfunction and the spectrum of otitis media (ASOM, OME, and CSOM)
INSTRUCTIONS
The Eustachian tube is the hidden mechanism underlying almost all forms of otitis media. Whether the pathology is ASOM (acute ET obstruction during an URTI), OME (chronic ET dysfunction causing persistent effusion), or CSOM (ET dysfunction preventing TM healing), the common thread is a failure of the ET's three essential functions: ventilation, drainage, and protection. Understanding ET anatomy and dysfunction is therefore not just a topic in its own right — it is the explanatory framework for the entire otitis media module cluster. This module also covers the less common but clinically distinctive patulous (abnormally open) ET, which presents with the characteristic symptom of autophony.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 4 (Anatomy of ET and ET Disorders) (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 7 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old IT professional comes to your clinic with a strange, distressing symptom: when she speaks, her own voice sounds as if it is echoing loudly inside her head. She finds it particularly troubling when she is speaking on the telephone. The symptom appeared 3 months ago after she lost 8 kg on a strict diet. It is worst in the morning and relieves slightly when she lies down with her head below the level of her body. Her tympanic membranes look normal on otoscopy and tympanometry is Type A bilaterally. What structure is malfunctioning, and in which direction — and why did weight loss trigger this?
WHY THIS MATTERS
The Eustachian tube is the least-examined but most clinically consequential structure in ENT — it underpins the pathophysiology of ASOM, OME, and CSOM, which together represent the most common ENT diagnoses seen in clinical practice. Every episode of middle ear infection begins with ET dysfunction: the tube fails to open during swallowing, negative middle ear pressure develops, and bacteria are aspirated from the nasopharynx into the sterile middle ear. Every child with recurrent OME requiring grommets has impaired ET function. Every patient with CSOM whose TM perforation fails to heal despite a dry ear has persistently dysfunctional ET that prevents natural membrane repair. Beyond these common obstructive disorders, the patulous (abnormally open) ET presents a distinct and fascinating clinical entity: rather than failing to open, the ET stays permanently open, creating the distressing symptom of autophony — the patient hears their own voice resonating through the open tube directly into the middle ear. Competency EN4.15 requires you to describe ET anatomy, discuss clinical features, choose investigations, and describe management of ET disorders — placing this module at the intersection of anatomy, physiology, and clinical practice across the entire otitis media spectrum.
RECALL
Recall the anatomy of the nasopharynx from your Year-1 studies. The nasopharynx is the space behind the nasal choanae and above the soft palate. The ET orifice (Eustachian cushion) opens on the lateral wall of the nasopharynx, at the level of the inferior turbinate's posterior end. Immediately posterior and superior to the ET orifice is the fossa of Rosenmüller (pharyngeal recess) — the commonest site of nasopharyngeal carcinoma. The adenoid (pharyngeal tonsil) sits in the roof and posterior wall of the nasopharynx, in direct anatomical proximity to the ET orifice — explaining why adenoid hypertrophy causes ET dysfunction. Recall also the ET's position as the only communication between the nasopharynx and the sterile middle ear — when this communication becomes uncontrolled (as in ET dysfunction), it becomes the route of infection; when it is severed or permanently blocked, the middle ear becomes a sealed hypoxic space that develops effusion.
Clinical Presentation of Eustachian Tube Disorders
Eustachian tube disorders present along a spectrum defined by the direction of dysfunction: at one pole is the obstructive ET that fails to open, causing negative middle ear pressure and its consequences; at the other pole is the patulous ET that fails to close, staying permanently open and transmitting respiratory and vocal sound directly to the middle ear. These two poles have opposite mechanisms and opposite clinical presentations, and the clinician who conflates them will mismanage both. The history is the key to distinguishing them: obstructive ET dysfunction produces a sensation of ear fullness, hearing loss, and repeated episodes of middle ear fluid — symptoms that are typically worse during and after URTIs and better between infections; patulous ET produces the distinctive symptom of autophony (the patient hears their own voice or their own breathing resonating loudly inside the affected ear), which is characteristically relieved by lying down with the head in a dependent position (because the venous engorgement of the dependent head closes the cartilaginous tube wall and reduces the abnormal patency). Understanding the direction of dysfunction — obstructive vs patent — is the first and most important clinical step.
History in obstructive ET dysfunction:
- Ear fullness or 'blocked ear' sensation (intermittent, often with URTIs or altitude change)
- Mild to moderate hearing loss (conductive, fluctuating)
- History of ASOM, OME, or recurrent middle ear infections (these are consequences of obstructive ET dysfunction)
- Popping or clicking in the ear during swallowing (may indicate intermittent ET opening)
- Age: children predominantly; also adults with adenoid hypertrophy, chronic rhinitis, allergy, or nasopharyngeal pathology
History in patulous ET:
- Autophony: Hearing own voice resonating loudly or echoing inside the head — the single most characteristic symptom
- Synchronous sounds: Hearing own breathing (blowing, rushing sound) synchronous with respiratory cycle
- Positional relief: Symptoms improve when lying down or bending head forward (dependent position → venous engorgement → closure of the soft cartilaginous tube wall)
- Precipitating factors: Significant weight loss (fatty tissue around the ET cartilage is lost → tube becomes permanently open), pregnancy, use of oral contraceptives, neuromuscular disorders (reduced tensor veli palatini tone)
- Symptoms worsen with exercise, anxiety, dehydration (all reduce peritubular tissue bulk)
Anatomy and Physiology of the Eustachian Tube
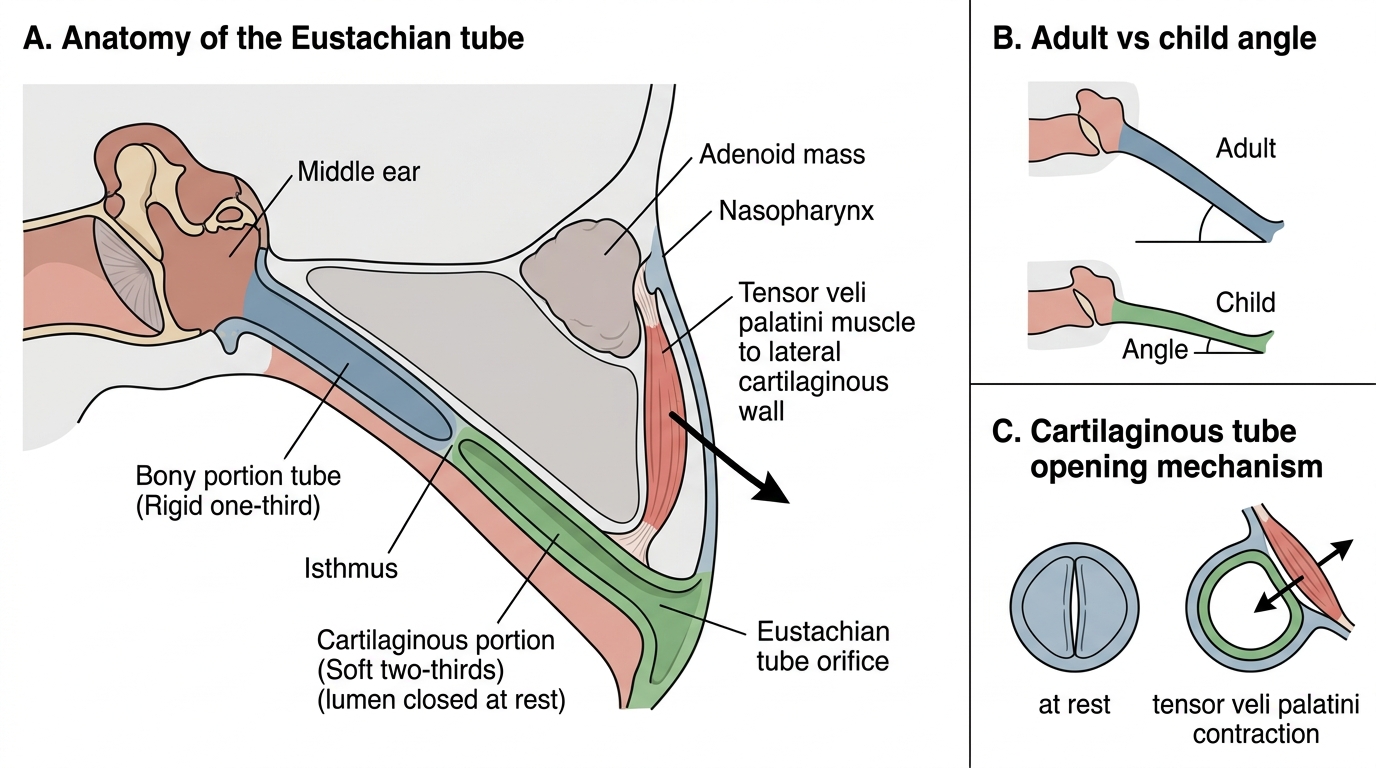
The Eustachian tube is a fibrocartilaginous channel approximately 35–37 mm long in adults, connecting the anterolateral wall of the nasopharynx to the anterior wall of the middle ear (the tympanic orifice). It has two structurally and functionally distinct portions that explain both its normal physiology and its failure modes in different disease states.
The bony (osseous) portion comprises the medial one-third (approximately 12 mm) of the ET. It runs within the temporal bone between the carotid canal and the tegmen, has rigid bony walls, and is always patent. It connects to the middle ear at its medial end.
The cartilaginous (fibrocartilaginous) portion comprises the lateral two-thirds (approximately 24 mm) and is formed by a hooked J-shaped cartilage whose medial limb forms the roof and part of the medial wall of the tube, with the lateral wall being a passive fibrous membrane. This portion has a slit-like lumen that is CLOSED AT REST — unlike the bony portion, the cartilaginous ET is normally collapsed shut by its own elastic cartilage and by the pharyngeal mucosal pressure. It opens only actively.
The isthmus — the junction of the bony and cartilaginous portions — is the narrowest point of the ET and is a site of particular significance: it is where mucosal oedema most readily produces complete obstruction.
Opening mechanism: The ET opens by contraction of the tensor veli palatini muscle (innervated by the mandibular nerve, CN V3). The tensor veli palatini attaches to the lateral fibrous wall of the cartilaginous ET; when it contracts during swallowing, yawning, or sneezing, it pulls the lateral wall away from the medial cartilage, opening the lumen. This is why swallowing equalises ear pressure during altitude changes. A secondary opener is the levator veli palatini (CN X, via pharyngeal plexus), which provides a minor contribution. In cleft palate, the abnormal insertion of the tensor veli palatini into the cleft margins rather than the soft palate means the muscle cannot exert its normal traction on the ET — ET opening is impaired, causing lifelong ET dysfunction.
The three functions of the ET:
1. Ventilation: Maintains equal air pressure on both sides of the TM by periodically opening to equilibrate middle ear pressure with atmospheric pressure. Without this, middle ear gas is absorbed by the mucosal capillaries, creating negative pressure, TM retraction, and eventual effusion.
2. Drainage: The mucociliary epithelium of the ET clears middle ear secretions toward the nasopharynx, preventing accumulation.
3. Protection: The normally closed tube prevents nasopharyngeal bacteria, secretions, and sound pressure from reaching the sterile middle ear.
Child vs adult ET: In children under 7 years, the ET is shorter (17–18 mm), more horizontal, and the cartilage is floppier. These characteristics: (a) reduce the gravitational barrier to ascending bacterial entry, (b) allow easier reflux of nasopharyngeal contents during bottle feeding in the supine position, and (c) impair the efficiency of mucociliary drainage — collectively explaining why ASOM and OME are overwhelmingly childhood diseases.
Anatomy and Pediatric Differences of the Eustachian Tube
SELF-CHECK
A 3-year-old child is prone to recurrent ASOM while his older adult brother is not. The single most important anatomical difference in their Eustachian tubes that explains this disparity is:
A. The child's ET is longer and more vertical — harder for bacteria to ascend
B. The child's ET is shorter, more horizontal, and floppier — easier for nasopharyngeal bacteria to ascend and reflux occurs more readily
C. The child's ET cartilage is harder and more rigid — less effective at opening with swallowing
D. The child's tensor veli palatini is stronger — it opens the ET more forcefully, introducing more bacteria
Reveal Answer
Answer: B. The child's ET is shorter, more horizontal, and floppier — easier for nasopharyngeal bacteria to ascend and reflux occurs more readily
In children under 7 years, the Eustachian tube is shorter (17–18 mm vs 35–37 mm in adults), more horizontal (less steep downward angle), and its cartilage is floppier. These three features together reduce the anatomical barrier to bacterial ascent from the nasopharynx, allow easier reflux of nasopharyngeal fluid (especially during bottle feeding in the supine position), and impair mucociliary drainage efficiency. This explains why ASOM and OME are primarily childhood diseases — as the tube lengthens and becomes more vertical with age, protection improves and ASOM incidence falls.
Examination and Investigations for ET Disorders
The examination strategy in ET disorders is guided by the clinical hypothesis established from the history: if obstructive ET dysfunction is suspected, the examination looks for evidence of negative middle ear pressure and its consequences (retracted TM, middle ear effusion); if patulous ET is suspected, the examination looks for respiratory synchronous TM movement. Both hypotheses can be confirmed or refuted by combining otoscopy with tympanometry — the combination is more sensitive than either alone. The nasopharynx must also be examined, because the most clinically consequential cause of ET obstruction in adults is a nasopharyngeal mass, and missing this examination is a patient safety error equivalent to the failure to perform nasendoscopy in adult unilateral OME. An efficient, accurate ET assessment also includes specific attention to the nasopharynx, because the fossa of Rosenmüller — the pharyngeal recess immediately posterior to the ET orifice — is the commonest site for nasopharyngeal carcinoma, and failure to examine it in an adult with unilateral ET dysfunction is a patient safety error of the first order.
Otoscopic findings:
- Obstructive ET dysfunction: TM is retracted (handle of malleus more horizontal and prominent; cone of light displaced); pars flaccida may be more noticeably retracted; in chronic cases, an amber or grey TM indicates OME; perforation, if present from old ASOM, fails to heal
- Patulous ET: The TM moves visibly with respiration — rises during expiration and falls during inspiration (respiratory synchronous TM movement). This can be confirmed by asking the patient to breathe in and out through one nostril while the other is occluded and observing the TM under the otoscope. This is the most specific clinical sign of patulous ET.
Tympanometry:
- Type C tympanogram: Peak compliance is present but shifted to negative pressure (below -100 daPa) — indicates negative middle ear pressure from ET dysfunction without frank effusion; a precursor state
- Type B tympanogram: Flat curve — indicates established middle ear effusion from prolonged obstructive ET dysfunction
- Type A with respiratory variation: In patulous ET, the Type A (normal) compliance curve may show subtle oscillations synchronous with respiration — this finding, combined with the history, supports the patulous ET diagnosis
Nasoendoscopy (flexible):
- Assessment of the adenoid size and proximity to the ET orifice (Eustachian cushion) — mandatory in children with recurrent OME to determine whether adenoidectomy is indicated
- Mandatory in adult ET dysfunction to visualise the fossa of Rosenmüller and exclude nasopharyngeal carcinoma (NPC) — the most important differential in adult ET obstruction
Valsalva test and Toynbee test:
- Valsalva: The patient holds their nose and blows — positive Valsalva (ear pressure equalises, or in a perforated TM, air bubbles through the perforation) = ET is patent
- Toynbee: The patient swallows with nose held — assesses ET closure (normally the ET closes after the opening Valsalva; Toynbee monitors this)
- These simple bedside tests assess ET patency and can be performed in any clinic
Additional investigations:
- CT temporal bone and nasopharynx: assesses adenoid size, ET course, and excludes nasopharyngeal masses
- PTA: conductive hearing loss with obstructive ET dysfunction; normal audiogram with patulous ET (hearing loss is not a feature of patulous ET — the problem is hypersensitivity to internal sounds, not reduced external hearing)