Page 17 of 23
EN4.15 | Eustachian Tube Disorders — SDL Guide (Part 2)
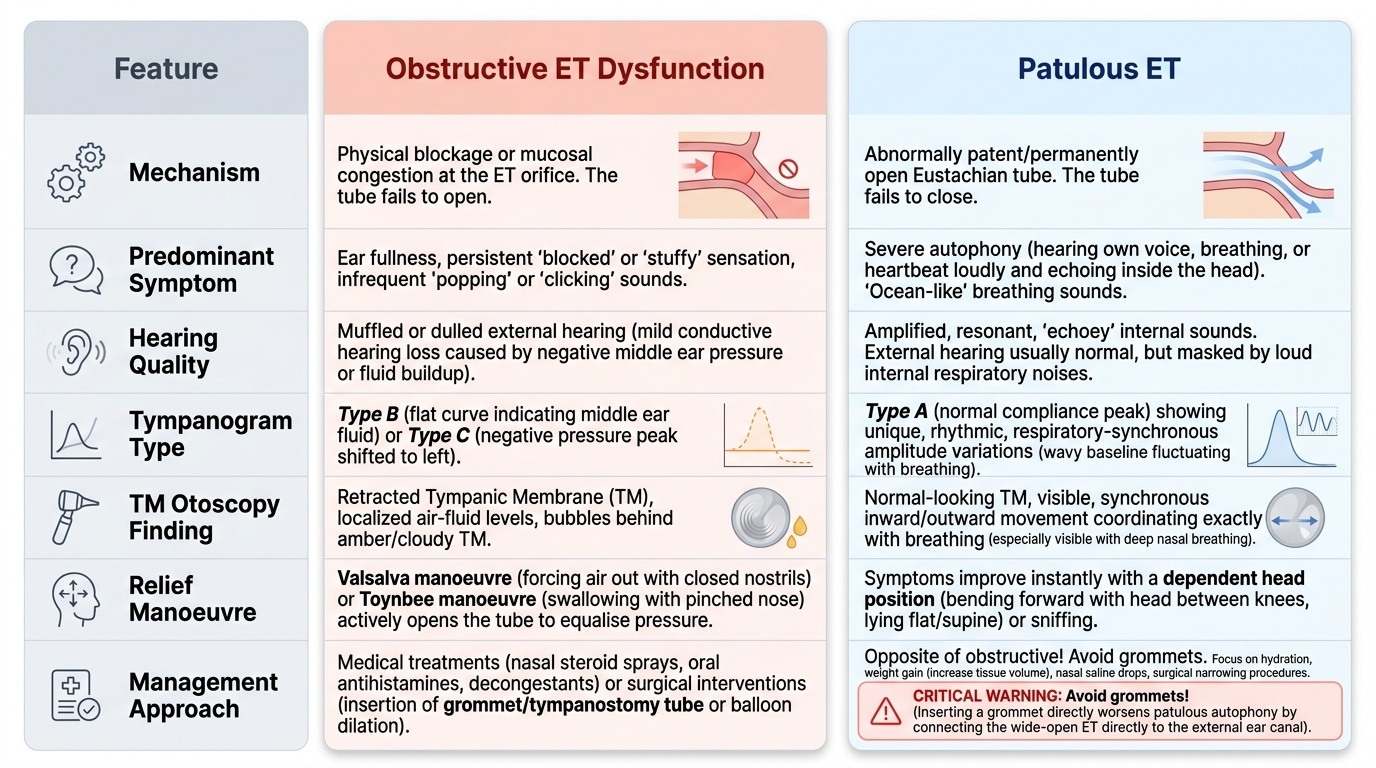
Diagnosis: Obstructive vs Patulous ET Dysfunction
The diagnosis of ET dysfunction requires integrating the history (direction of symptoms — blocked vs hyper-resonant), the otoscopic finding (retracted or fluid-containing TM vs normal TM with respiratory movement), and the tympanometric finding (Type B or C vs Type A with respiratory variation) into a coherent clinical picture. The obstructive vs patulous distinction is not merely semantic — it determines the entire management approach, which is directly opposed between the two types. Treating a patulous ET with a grommet (the standard intervention for obstructive ET dysfunction) worsens symptoms by directly connecting the open ET to the EAC, amplifying the autophony and respiratory sounds — a classic iatrogenic error made when the two types are confused.
Provided image
The clinical diagnostic framework for ET function assessment includes four validated bedside tests:
- Valsalva manoeuvre: Patient pinches the nose shut and blows gently — if the ET opens, pressure is equalised (patient notices ear popping) or in a perforated TM, air can be seen bubbling. Positive = ET is patent. Negative = ET obstruction.
- Toynbee manoeuvre: Patient swallows with the nose pinched — tests ET opening with swallowing. Used alongside Valsalva.
- Politzer bag insufflation: Air is blown into the nasopharynx via a Politzer bag while the patient says 'K-K-K' (to close the nasopharynx) — if ET opens, the patient notices equalisation; the examiner can see TM movement via otoscope.
- Sonotubometry: A sound delivered to the nostril and detected in the ear canal — specialised investigation not available in routine practice.
Key differential diagnosis for obstructive ET dysfunction:
- Adenoid hypertrophy (children: most common; adults: rare but possible)
- Allergic rhinitis (mucosal oedema at ET orifice)
- Chronic rhinosinusitis (mucosal oedema)
- Nasopharyngeal carcinoma (adult, unilateral: MUST BE EXCLUDED BY NASOENDOSCOPY)
- Cleft palate (structural tensor veli palatini dysfunction)
- Irradiation to the head and neck (radiation-induced ET mucosal fibrosis)
Patulous ET — diagnosis:
The single most diagnostic symptom is autophony improving with dependent head position. The otoscopic finding of respiratory synchronous TM movement is pathognomonic when seen. Tympanometry Type A with respiratory amplitude variation supports the diagnosis. Patulous ET is rare and often under-recognised — many patients are misdiagnosed with anxiety or somatoform disorder before the ear is carefully examined during the reporting of autophony.
SELF-CHECK
A 28-year-old woman describes hearing her own voice loudly inside her left ear when she speaks. The symptom is better when she lies down with her left side up. Otoscopy shows a normal-appearing left TM. Tympanometry is Type A bilaterally. On having her breathe in and out through one nostril, the TM appears to move in synchrony with respiration. The diagnosis is:
A. Otitis media with effusion — tympanogram should be repeated in 4 weeks
B. Patulous Eustachian tube — ET fails to close, transmitting respiratory and vocal sounds directly to the middle ear
C. Obstructive ET dysfunction with early negative pressure — Type C tympanogram expected on repeat
D. Acoustic neuroma — autophony is a classic early presenting symptom
Reveal Answer
Answer: B. Patulous Eustachian tube — ET fails to close, transmitting respiratory and vocal sounds directly to the middle ear
The combination of autophony (hearing own voice loudly), respiratory synchronous TM movement on otoscopy, and symptom relief in the dependent head-down position is diagnostic of patulous Eustachian tube — the ET remains permanently open rather than being obstructed. The normal Type A tympanogram is consistent (patulous ET does not cause effusion or negative pressure). OME would have a Type B tympanogram and no autophony. Obstructive ET dysfunction causes ear fullness and negative pressure symptoms, not autophony with positional relief. Acoustic neuroma causes SNHL and tinnitus (not autophony with a normal audiogram).
Management of Eustachian Tube Disorders
Management of ET disorders differs fundamentally between the obstructive and patulous types, reflecting their opposite pathophysiology. In obstructive ET dysfunction the aim is to facilitate ET opening and reduce mucosal oedema; in patulous ET the aim is to restore closure of the permanently open tube. The two management strategies are not interchangeable — and as stated earlier, applying obstructive ET dysfunction treatment (specifically, a grommet) to a patulous ET will worsen autophony by creating a direct acoustic conduit between the open tube and the external environment. Accurate pre-operative diagnosis is therefore the highest-priority step before any surgical intervention.
Management of obstructive ET dysfunction: This principle is the single most important operational rule in the management of ET disorders: establish the diagnosis first, then select the intervention matched to the direction of dysfunction.
Conservative (first-line):
- Autoinflation (Otovent device): The patient blows up a nasal balloon with one nostril (closing the other), raising nasopharyngeal pressure to force open the ET. Non-invasive; modest evidence of benefit in cooperative children ≥4 years; often used as a self-management tool between appointments.
- Intranasal corticosteroids: Fluticasone or mometasone nasal spray to reduce mucosal oedema at the ET orifice — evidence for benefit in ET dysfunction associated with allergic rhinitis or chronic rhinosinusitis. Minimal systemic absorption.
- Decongestants (nasal sprays or oral): Oxymetazoline or xylometazoline nasal drops provide short-term mucosal decongestion; limit use to <7 days to avoid rebound rhinitis medicamentosa
- Allergy management: Allergen avoidance, antihistamines, and immunotherapy for allergic rhinitis-driven ET dysfunction
- Nasal saline irrigation: Reduces chronic mucosal congestion; safe for long-term use
Surgical:
- Myringotomy + grommet insertion: Bypasses the dysfunctional ET by creating an artificial ventilation route through the TM; standard surgical treatment for OME secondary to chronic obstructive ET dysfunction (covered in OME module)
- Adenoidectomy: Removes the adenoid mass obstructing the ET orifice and reduces the bacterial/biofilm reservoir; indicated in children ≥4 years with recurrent OME or recurrent ASOM with documented adenoid hypertrophy
- Eustachian tube balloon dilation (ETBD): A newer minimally invasive procedure in which a balloon catheter is passed through the nasal passage into the cartilaginous portion of the ET under endoscopic guidance and inflated for 2 minutes to dilate the ET lumen; emerging evidence supports benefit in adult chronic obstructive ET dysfunction unresponsive to conservative management; currently available in specialist ENT centres
Management of patulous ET:
- Conservative (first-line): Isotonic saline nasal drops instilled into the nostril while the head is tilted to increase mucosal engorgement and temporarily narrow the ET lumen; increased fluid and nutritional intake to restore peritubular fat (most important when weight loss is the precipitant); stopping oral contraceptives if implicated (oestrogen-related patulous ET)
- Topical ear drops: Salicylate ear drops or potassium iodide solutions to irritate the mucosa and promote closure
- Surgical (reserved for severe cases): Injection of Teflon or other bulking agents around the ET cartilage to mechanically narrow the lumen; rarely, myringotomy (a small deliberate opening in the TM) paradoxically reduces autophony in some cases by breaking the acoustic amplification of the patulous ET — this is the exception where a grommet or TM opening is used for patulous rather than obstructive ET (reserved for refractory cases after specialist assessment)
CLINICAL PEARL
The single most clinically important rule in ET disorders is: never insert a grommet to treat autophony in suspected patulous ET. The grommet amplifies the open-tube problem by creating an additional direct acoustic conduit through the TM to the external ear canal, making the autophony dramatically worse. Always confirm the diagnosis — specifically, look for the respiratory synchronous TM movement on otoscopy — before any surgery. A second pearl: in adult patients with new unilateral ET dysfunction (especially unilateral OME), the first investigation is flexible nasendoscopy to exclude a nasopharyngeal mass at the Eustachian tube orifice. Nasopharyngeal carcinoma is too common in the Asian population to be overlooked.
Self-Assessment: Eustachian Tube Disorders
Before testing yourself with the final questions, consolidate the anatomical framework and the clinical diagnostic dichotomy that underpins this module. The Eustachian tube is a 35–37 mm fibrocartilaginous channel in adults with a bony medial third (always patent) and a cartilaginous lateral two-thirds (normally closed at rest, opened by tensor veli palatini contraction during swallowing). Its three functions are ventilation, drainage, and protection of the middle ear. In children, the tube is shorter, more horizontal, and floppier — predisposing to ASOM and OME. The two principal ET disorders are: (1) obstructive ET dysfunction — the tube fails to open, causing negative middle ear pressure, retraction, and effusion (ASOM/OME/CSOM); and (2) patulous ET — the tube fails to close, causing autophony, synchronous breathing sounds, and relief in the dependent head-down position. These two diagnoses have opposite mechanisms and opposite management strategies. Obstructive ET dysfunction is managed with autoinflation, intranasal corticosteroids, adenoidectomy, grommets, or ET balloon dilation. Patulous ET is managed with saline drops, nutritional restoration (if weight loss is the cause), and specialist interventions in refractory cases. Inserting a grommet for patulous ET worsens symptoms — it must not be done.
Key consolidation facts:
- ET length: adult 35–37 mm; child 17–18 mm
- ET portions: bony (medial, always open), cartilaginous (lateral, normally closed)
- ET opening muscle: tensor veli palatini (CN V3)
- Narrowest point: isthmus (bony-cartilaginous junction)
- Three ET functions: ventilation, drainage, protection
- Patulous ET symptoms: autophony, synchronous breathing sounds, relief lying down
- Patulous ET precipitants: weight loss, pregnancy, OCP use, neuromuscular disorders
- Type B tympanogram = obstructive (effusion); Type C = negative pressure; Type A with respiratory variation = patulous ET
- Never give a grommet for patulous ET
SELF-CHECK
A 45-year-old man presents with longstanding right ear fullness and mild hearing loss. Flexible nasoendoscopy reveals a smooth submucosal mass posterior to the right ET orifice in the fossa of Rosenmüller. The most appropriate next step is:
A. Prescribe intranasal corticosteroids and review in 6 weeks
B. Perform ET balloon dilation (ETBD) to treat the obstructive ET dysfunction
C. Biopsy the nasopharyngeal mass under general anaesthesia to exclude nasopharyngeal carcinoma
D. Insert a right grommet to bypass the ET obstruction while awaiting further workup
Reveal Answer
Answer: C. Biopsy the nasopharyngeal mass under general anaesthesia to exclude nasopharyngeal carcinoma
A smooth submucosal mass in the fossa of Rosenmüller (the pharyngeal recess posterior to the ET orifice) in a middle-aged man with unilateral ET dysfunction is nasopharyngeal carcinoma until proven otherwise. NPC frequently presents as a submucosal mass in the fossa of Rosenmüller causing unilateral ET obstruction. The mandatory next step is biopsy under GA to obtain histological diagnosis. Intranasal corticosteroids and grommet insertion address symptoms without diagnosing or treating the underlying malignancy. ET balloon dilation is irrelevant when there is a structural mass causing obstruction. Early biopsy allows staging and treatment of a surgically resectable NPC.