Page 10 of 23
EN4.{7,11} | Squamosal CSOM with Mastoidectomy — SDL Guide
Learning Objectives
- Identify the clinical features that distinguish squamosal (unsafe) CSOM from mucosal (safe) CSOM, with emphasis on the attic/marginal perforation and the presence of cholesteatoma
- Describe the pathogenesis, types, and mechanism of bone destruction in cholesteatoma
- Describe the otoscopic, audiological, and imaging findings characteristic of squamosal CSOM
- Describe the indications for and operative steps involved in the main types of mastoidectomy (cortical, modified radical, radical, combined approach)
INSTRUCTIONS
Squamosal (atticoantral) CSOM is the 'unsafe' variant of chronic middle ear disease — unsafe because it is associated with cholesteatoma, a destructive cyst of keratinising squamous epithelium that erodes bone and can produce life-threatening intracranial complications. Unlike the safe mucosal type, squamosal CSOM requires surgery regardless of symptom severity — the decision is not whether to operate but when and what operation to perform. Understanding cholesteatoma and mastoidectomy is among the most important competencies in clinical ENT, because missing an attic perforation or failing to refer for mastoidectomy can allow cholesteatoma to silently erode the ossicles, facial nerve, or skull base over months to years.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th edition, Ch 7 (CSOM — Squamosal Type and Mastoidectomy) (textbook)
- Hazarika P — Textbook of ENT and Head and Neck Surgery, 3rd edition, Ch 10-11 (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th edition, Vol 2 (Otology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man comes to your ENT OPD with a 2-week history of increasing right-sided headache, right ear discharge (scanty but markedly foul-smelling), and, since yesterday, mild weakness of the right side of his face. On otoscopy you see a crust in the right attic. When you gently remove the crust with a crocodile forceps, you expose a small attic perforation in the pars flaccida with a pearly-white mass visible behind it. His right lower face droops slightly when he smiles. What is the diagnosis, why is this an emergency, and what is the single most important immediate step in management?
WHY THIS MATTERS
Squamosal CSOM — also called atticoantral CSOM or the 'unsafe' type — accounts for approximately 20% of all CSOM cases but is responsible for the vast majority of life-threatening CSOM complications. The reason for this disproportionate danger is cholesteatoma: a cyst of desquamating keratinising squamous epithelium in the middle ear that expands relentlessly, secreting collagenases that erode through bone at whatever structure the cyst reaches — ossicles (causing hearing loss), tegmen tympani (causing meningitis), semicircular canals (causing labyrinthitis and vertigo), the facial nerve canal (causing facial palsy), or the sigmoid sinus (causing thrombosis). The danger of squamosal CSOM is therefore not its presenting severity — the initial otoscopic finding can appear deceptively minor — but its progressive potential if untreated. A small attic crust hiding a cholesteatoma sac is more dangerous than a large foul-smelling central perforation. For you as a clinician, the key competency is to systematically examine the pars flaccida in every CSOM ear, recognise the otoscopic signs of cholesteatoma, and refer for mastoidectomy without delay. Competencies EN4.7 and EN4.11 require you to take a history, describe clinical features, choose investigations, describe management, and describe the steps of mastoidectomy.
RECALL
Recall the anatomy of the tympanic membrane and the ear from your earlier modules. The pars flaccida (Shrapnell's membrane) is the small, slack superior portion of the TM, lacking the fibrous middle layer of the pars tensa and therefore more susceptible to retraction under negative pressure. The attic (epitympanum) is the space above the level of the TM, housing the malleus head and the body and short process of the incus — collectively called the ossicular block. The lateral wall of the attic is formed by the scutum (the sharp bony spur of the lateral wall of the epitympanum visible on X-ray and CT); erosion of the scutum by cholesteatoma is a classic imaging finding. Prussak's space is the small recess medial to the pars flaccida and lateral to the malleus neck — the commonest site for the first cholesteatoma pocket to form. Recall from your mucosal CSOM module that the central perforation in the pars tensa is the safe type, while any attic or marginal perforation should be treated as unsafe until proven otherwise.
Clinical Presentation of Squamosal (Unsafe) CSOM
The clinical presentation of squamosal CSOM is characterised by a combination of features that — taken together — should always raise the suspicion of cholesteatoma. The first and most diagnostically useful feature is the nature of the ear discharge: unlike the profuse mucoid discharge of safe CSOM, squamosal CSOM produces scanty but markedly foul-smelling discharge. The foul odour arises from the anaerobic bacterial degradation of the keratin debris within the cholesteatoma sac — it is qualitatively different from the mild offensive smell that can occasionally accompany infected mucosal CSOM. A single whiff of the distinctively fetid smell from a small attic perforation should immediately trigger the suspicion of cholesteatoma. The second feature is hearing loss, which is typically greater than expected for the degree of visible disease, because cholesteatoma often erodes the ossicular chain (especially the long process of the incus — the most vulnerable ossicle due to its poor blood supply). The third critically important feature is the absence of severe spontaneous pain in uncomplicated cholesteatoma — the disease is insidiously painless, which is paradoxically what makes it dangerous, because patients tolerate it for years. When otalgia, headache, or neurological symptoms appear, they indicate that a complication is developing, and the onset of these symptoms in a patient with known or suspected cholesteatoma is a clinical emergency requiring urgent imaging and hospital admission.
Key history questions:
- Discharge: onset, duration, character — specifically ask about the ODOUR (foul = suspect cholesteatoma)
- Hearing loss: duration, progressive or stable; tinnitus
- Pain: absence in uncomplicated disease; new or worsening otalgia or headache = complication alert
- Vertigo: true rotational vertigo suggests labyrinthine fistula (cholesteatoma eroding the semicircular canal)
- Facial weakness: ipsilateral lower motor neuron pattern = facial nerve erosion by cholesteatoma (surgical emergency)
- Neurological symptoms (headache, neck stiffness, confusion, diplopia): suggest intracranial complication
- Duration of ear disease: childhood ASOM history; prior ear surgery (residual or recurrent cholesteatoma)
Red flags — any of these = urgent referral and imaging:
- Otalgia or headache in a patient with previously painless CSOM
- Vertigo or imbalance (labyrinthine fistula)
- Facial nerve palsy ipsilateral to the diseased ear
- Swinging fever or systemic toxicity (intracranial suppuration)
- Post-auricular swelling with downward/outward displacement of pinna (Bezold's abscess or subperiosteal mastoid abscess)
Anatomy, Pathophysiology, and Types of Cholesteatoma
Cholesteatoma is a cyst lined by keratinising stratified squamous epithelium situated within the middle ear cleft or mastoid. The crucial word is 'keratinising' — normal external auditory canal skin is keratinising, and normal middle ear mucosa is not. When squamous epithelium gains access to the middle ear (through a perforation, a retraction pocket, or congenitally), it continues to desquamate dead keratin layers inward, expanding the cyst as the keratin accumulates. The cyst wall matrix and the surrounding inflammatory reaction produce prostaglandins, interleukins, and collagenases (especially MMP-2 and MMP-9) that directly dissolve the collagen matrix of bone — this enzyme-mediated osteolysis is what makes cholesteatoma destructive. The ossicular chain, the tegmen tympani, the semicircular canal walls, the facial nerve bony canal, and the sigmoid sinus plate are all vulnerable to this progressive erosion. The rate of expansion is variable but relentless in the absence of surgery.
Classification of cholesteatoma:
1. Congenital cholesteatoma:
Arises from embryological rests of squamous epithelium trapped behind an intact tympanic membrane during foetal development. Classic presentation: a pearly white mass visible behind an intact, normal-appearing TM, usually in the anterosuperior or posterosuperior quadrant in a child with no prior ear disease, no perforation, and no history of otitis media. The lack of any TM abnormality is the key distinguishing feature.
2. Acquired primary cholesteatoma:
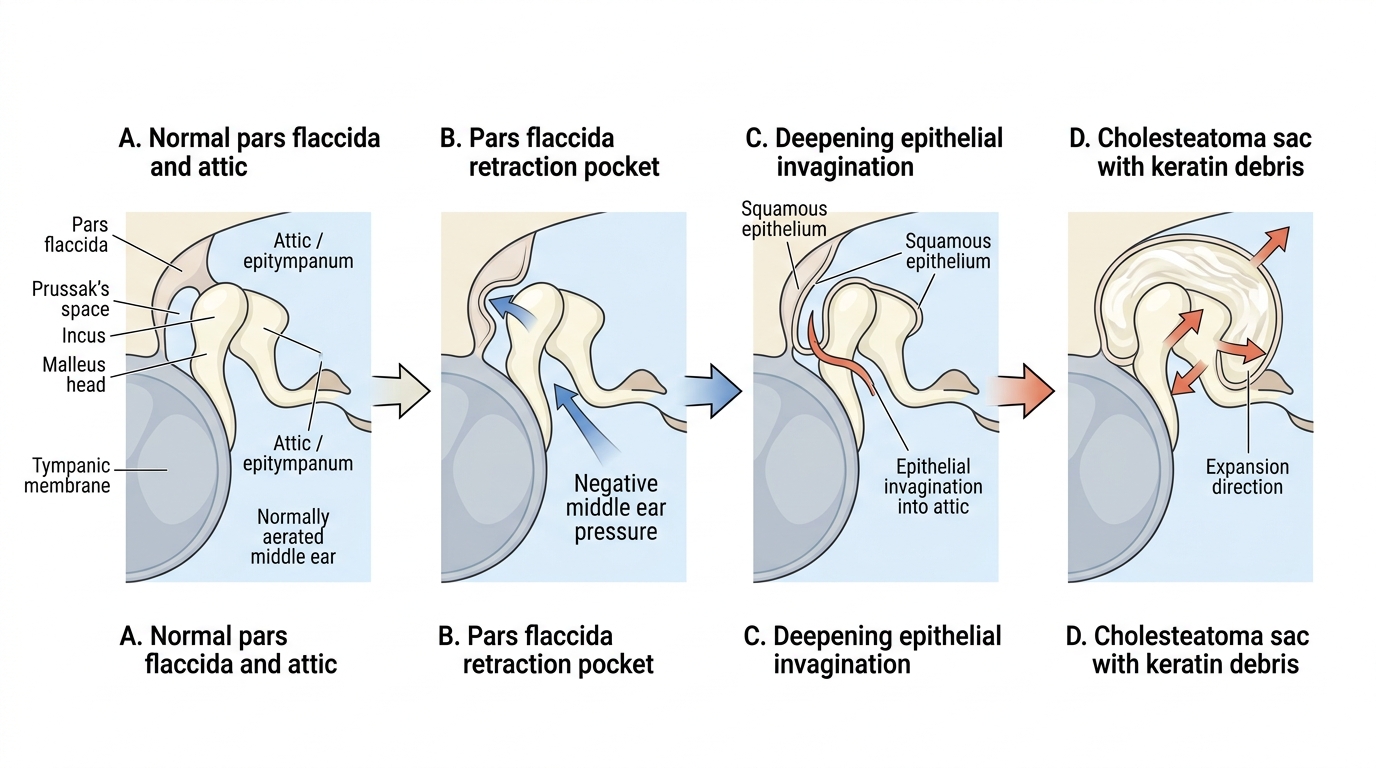
Arises without a TM perforation — the pars flaccida invaginates inward under sustained negative middle ear pressure (from ET dysfunction), forming a retraction pocket in Prussak's space (the space lateral to the malleus neck and medial to the pars flaccida). As the retraction pocket deepens, it cannot self-clean (unlike normal external canal skin), keratin accumulates, and the pocket gradually expands medially into the attic, wrapping around the ossicular chain. This is the pathogenesis by the invagination theory — the most widely accepted model.
3. Acquired secondary cholesteatoma:
Arises from a marginal TM perforation — squamous epithelium from the external auditory canal migrates medially through the marginal perforation into the middle ear, where it continues to keratinise and form a cholesteatoma sac. This is the most common type (~70% of all acquired cholesteatomas).
Pathogenesis of Acquired Primary Cholesteatoma
SELF-CHECK
A 10-year-old child is found to have a pearly white mass behind an intact tympanic membrane in the anterosuperior quadrant on a routine examination. There is no history of ear infections, no TM perforation, and no discharge. This presentation is most consistent with:
A. Acquired secondary cholesteatoma from a healed marginal perforation
B. Congenital cholesteatoma arising from an embryological squamous cell rest behind an intact TM
C. Acquired primary cholesteatoma from a pars flaccida retraction pocket
D. Glomus tympanicum tumour presenting as a middle ear mass
Reveal Answer
Answer: B. Congenital cholesteatoma arising from an embryological squamous cell rest behind an intact TM
Congenital cholesteatoma presents as a pearly white mass behind an INTACT TM with NO prior ear disease, NO perforation, and typically in children. This is the classic description. Acquired secondary cholesteatoma requires a marginal perforation for squamous epithelium to enter. Acquired primary cholesteatoma arises from a pars flaccida retraction — the TM would show attic changes, not an intact appearance in the anterosuperior quadrant. Glomus tympanicum would appear red or pulsatile, not white.
Examination and Investigations
The examination of a patient with suspected squamosal CSOM must be meticulous and systematic — a small attic crust hiding a cholesteatoma can easily be missed on a cursory examination. Every patient with CSOM must have the pars flaccida examined separately and specifically under good lighting, preferably with a microscope or operating otoscope. The clinical history has already established the suspicion: foul-smelling discharge, disproportionate hearing loss, or red-flag symptoms. The examination confirms or excludes the cholesteatoma and assesses the extent of disease. In addition to the ear examination, the neurological assessment must be completed — facial nerve function (House-Brackmann grading), nystagmus (lateral canal fistula sign), meningism (neck stiffness), and papilloedema should all be documented because their presence immediately elevates the management urgency to emergency.
Otoscopic findings in squamosal CSOM:
- Attic crust or debris: A crust, flaky material, or pus-like debris in the attic region (above the short process of the malleus) is a classical early finding; must be gently removed to visualise what lies beneath
- Attic perforation (pars flaccida perforation): A defect in the pars flaccida, usually in the posterosuperior quadrant of the attic; may be small and easily missed
- Pearly white mass: Cholesteatoma sac visible through the attic perforation as white/grey pearlescent material — pathognomonic
- Granulation tissue: Red friable granulation tissue in the attic indicates active infection around the cholesteatoma; may bleed on touch
- Marginal perforation: A posterior or posterosuperior TM perforation reaching the annulus, with squamous debris in the middle ear
- Facial nerve testing: Mandatory — assess voluntary eye closure, forehead wrinkling, and corner-of-mouth movement (House-Brackmann scale)
- Fistula test (Hennebert's sign): Apply gentle pneumatic pressure to the EAC via a pneumatic speculum; observe the eyes for nystagmus. A positive fistula test (nystagmus induced by pressure) suggests a labyrinthine fistula — cholesteatoma has eroded the lateral semicircular canal bone
Investigations:
- HRCT temporal bone (mandatory): Non-negotiable in all confirmed or suspected cholesteatoma. CT identifies: scutum erosion (classic early sign), ossicular erosion (long process of incus most often), tegmen dehiscence, semicircular canal erosion, facial canal dehiscence, sigmoid sinus involvement, soft-tissue mass in mastoid. CT defines the extent of surgery needed.
- Pure-tone audiometry (PTA): Shows conductive or mixed hearing loss. The presence of sensorineural component (raised bone conduction threshold) suggests labyrinthine damage — either from direct erosion or from toxic labyrinthitis.
- MRI (when complications suspected): For soft-tissue detail, intracranial extension, or to distinguish cholesteatoma from granulation tissue when CT is equivocal
- Culture and sensitivity: Of middle ear discharge