Page 11 of 23
EN4.{7,11} | Squamosal CSOM with Mastoidectomy — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of squamosal CSOM with cholesteatoma is primarily clinical: the combination of an attic perforation (or marginal perforation) with pearly white debris or granulation tissue, a foul-smelling discharge, and the HRCT temporal bone showing scutum erosion and soft tissue density in the epitympanum is virtually diagnostic. The key diagnostic act, as emphasised throughout this module, is the systematic examination of the pars flaccida in every CSOM case — without this step, the diagnosis will be missed. The diagnosis has two inseparable consequences: HRCT must be performed to stage the disease, and mastoidectomy must be planned. There is no conservative management pathway for confirmed cholesteatoma (unlike the dry-ear phase in mucosal CSOM) — the only question is the timing of surgery and the surgical approach.
Differential diagnosis of an attic or middle ear mass:
1. Mucosal (safe) CSOM: The most important differential. Distinguishing features of safe type: central pars tensa perforation, NO whitish debris, intact pars flaccida, no foul odour. Never call a pars flaccida perforation 'safe.'
2. Tympanosclerosis: White chalky calcification on the TM surface or in the middle ear — can appear white like cholesteatoma. Key distinction: tympanosclerosis is flat, chalky, and non-expanding; TM is intact; no foul discharge; no bone erosion on CT. It is a result of healed inflammation, not active disease.
3. Congenital cholesteatoma: White mass behind an INTACT TM in a child with no prior ear disease. No perforation. Managed by surgery but presents differently from acquired types.
4. Glomus tympanicum (paraganglioma): Vascular middle ear tumour appearing as a RED pulsatile mass behind the TM ('rising sun' sign on otoscopy). Pulsatile tinnitus is characteristic. CT shows an enhancing mass at the cochlear promontory. Distinguished from cholesteatoma by colour, pulsatility, and imaging characteristics.
5. Aberrant internal carotid artery: A vascular anomaly presenting as a pulsatile retrotympanic mass, potentially misidentified as a middle ear tumour or cholesteatoma. CT angiography differentiates.
The HRCT in squamosal CSOM — key findings to report:
- Scutum erosion (the lateral epitympanic spur): a classic early finding
- Soft tissue density in Prussak's space or attic
- Ossicular erosion (long process of incus most commonly)
- Extension into the mastoid antrum or mastoid air cells
- Tegmen tympani dehiscence (risk of CNS complication)
- Semicircular canal erosion (risk of fistula)
- Facial canal dehiscence
- Sigmoid sinus plate erosion
SELF-CHECK
HRCT temporal bone in a patient with suspected right squamosal CSOM shows erosion of the right scutum, soft tissue density filling the right attic, and erosion of the long process of the right incus. What is the surgical implication of these findings?
A. Conservative management with topical ciprofloxacin for 6 weeks is appropriate; surgery is not yet indicated
B. Myringoplasty (tympanoplasty Type I) is the appropriate first intervention to close the perforation
C. Mastoidectomy is indicated to remove the cholesteatoma and address the ossicular erosion; the eroded incus will require ossicular reconstruction
D. Watchful waiting for 3 months with repeat CT is the standard approach
Reveal Answer
Answer: C. Mastoidectomy is indicated to remove the cholesteatoma and address the ossicular erosion; the eroded incus will require ossicular reconstruction
CT findings of scutum erosion, attic soft-tissue mass (cholesteatoma), and incus long-process erosion confirm squamosal CSOM with established bone destruction. Mastoidectomy is mandatory — there is no non-surgical option for cholesteatoma. The scutum erosion and attic disease define the extent of mastoid/attic surgery required; the incus erosion means that ossicular reconstruction (TORP or PORP) will be needed as part of the procedure or at a second-look operation. Tympanoplasty Type I (myringoplasty) is for safe mucosal CSOM with intact ossicles — irrelevant here. Watchful waiting allows the cholesteatoma to expand further.
Management: Surgery — Types of Mastoidectomy
Management of squamosal CSOM is surgical. Unlike mucosal CSOM where a dry ear phase precedes an elective tympanoplasty, the presence of cholesteatoma is itself an absolute indication for surgery. The urgency depends on the presence or absence of complications: uncomplicated squamosal CSOM can be managed as an urgent elective procedure within weeks; cholesteatoma with complications (facial palsy, labyrinthine fistula, intracranial spread) is a surgical emergency requiring immediate hospital admission and operative intervention. The goals of mastoidectomy in cholesteatoma are: (1) complete eradication of all cholesteatoma matrix and debris; (2) creation of a safe ear (one that does not risk life-threatening complications) even at the cost of hearing; (3) hearing rehabilitation as a secondary goal once the primary goal of safety is achieved. The principle 'safety before hearing' is the guiding philosophy of cholesteatoma surgery — it distinguishes it from the tympanoplasty for safe CSOM where hearing restoration is the primary operative aim.
Provided image
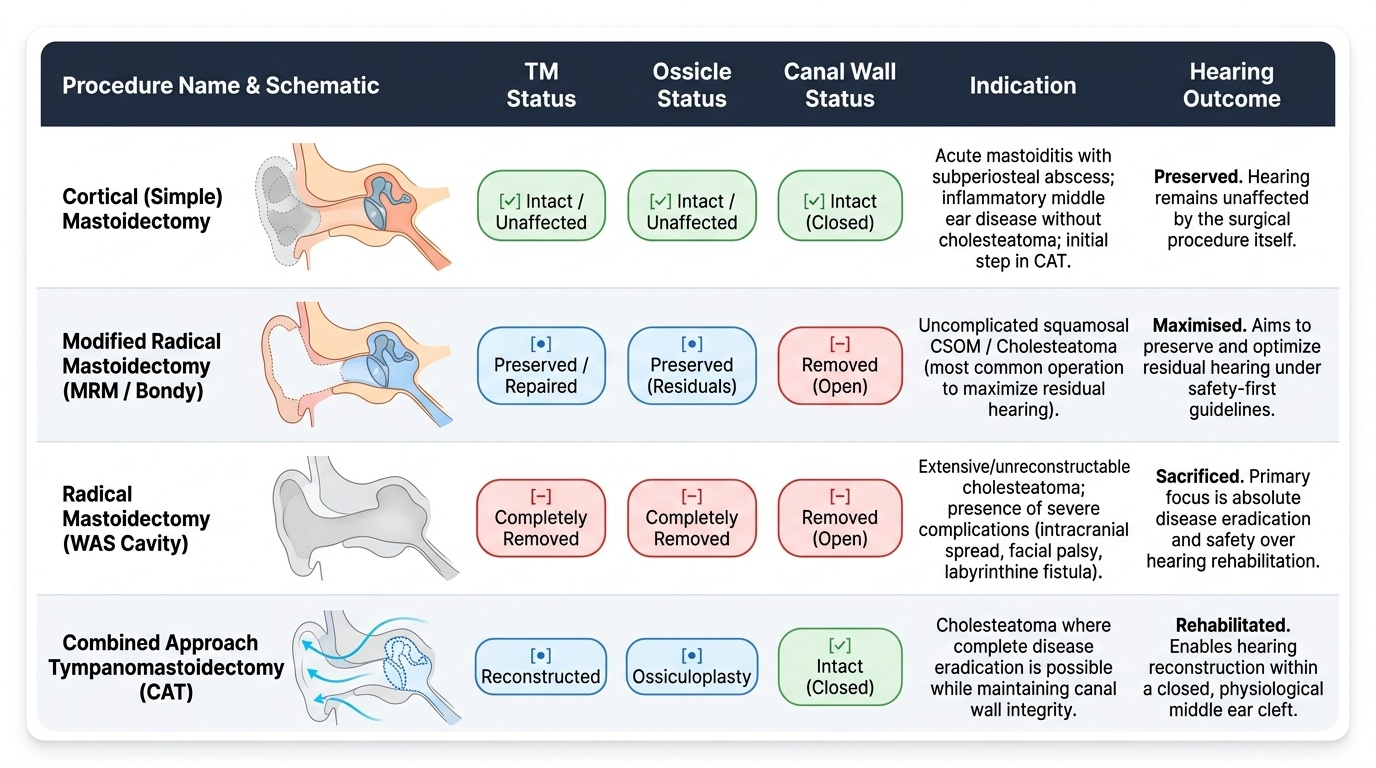
Types of mastoidectomy — classification and indications:
1. Cortical (simple) mastoidectomy:
Opens the mastoid cortex and exenterates all mastoid air cells, exposing the mastoid antrum, without modifying the posterior canal wall or middle ear. The canal wall is kept intact. Indications: acute mastoiditis with subperiosteal abscess (drainage); as the initial step in combined approach tympanomastoidectomy; inflammatory disease without cholesteatoma.
2. Modified Radical Mastoidectomy (MRM / Bondy operation):
The most common operation for cholesteatoma. The posterior external auditory canal wall is taken down to create an open mastoid cavity that communicates with the EAC — this is the mastoid cavity (radical cavity). However, the middle ear and any remaining ossicles/TM are preserved as far as possible. Disease is removed from the mastoid, attic, and middle ear while residual hearing is maximised. The posterior canal wall removal is what distinguishes MRM from cortical mastoidectomy. The resulting open cavity requires lifelong outpatient review (cleaning and cavity care) and strict water precautions.
3. Radical mastoidectomy (Radical or WAS cavity — Wullstein classification):
Complete removal of the posterior canal wall, ALL of the tympanic membrane, and ALL ossicles. Creates a single large open cavity (EAC + middle ear + mastoid). Hearing is severely impaired. Indications: advanced cholesteatoma involving the entire middle ear and ossicular chain, recurrent or residual cholesteatoma where no ossicular reconstruction is possible, or when the middle ear environment is hostile to reconstruction. Rarely performed as primary procedure today — MRM has largely replaced it.
4. Combined Approach Tympanomastoidectomy (CAT / Intact Canal Wall):
Removes the mastoid disease via a post-aural approach but preserves the posterior canal wall. This is a two-stage operation: Stage 1 removes cholesteatoma; Stage 2 at 9–12 months confirms no residual cholesteatoma (second-look) and reconstructs the ossicular chain. Advantage: preserves better acoustic anatomy for hearing reconstruction. Disadvantage: higher residual/recurrent cholesteatoma rates because the canal wall prevents complete visualisation; requires second surgery.
Ossicular reconstruction after mastoidectomy:
When the ossicular chain is eroded by cholesteatoma, hearing can be partially rehabilitated using prostheses:
- PORP (Partial Ossicular Replacement Prosthesis): Used when the stapes superstructure is intact — connects the TM/graft to the stapes head
- TORP (Total Ossicular Replacement Prosthesis): Used when only the stapes footplate remains — connects the TM/graft directly to the footplate
Post-operative care after MRM:
- Cavity dressing changes; cavity granulations managed with silver nitrate or steroid drops
- Strict water precautions (no swimming, ear plugs during bathing) — lifelong
- Regular outpatient cavity reviews (typically every 6–12 months) for cleaning and surveillance for recurrence
- Hearing aid may be needed if ossicular reconstruction fails or was not possible
- Second-look at 9–12 months in CAT cases
CLINICAL PEARL
The most important clinical rule in squamosal CSOM is: cholesteatoma is never safely managed conservatively. Once the diagnosis is confirmed by otoscopy (attic perforation with pearly debris) and HRCT (scutum erosion, attic soft tissue mass), mastoidectomy is the treatment — the only decision remaining is timing and approach. A second critical rule: every facial nerve palsy in a patient with known CSOM is a surgical emergency. Cholesteatoma erosion of the facial nerve canal is the cause until proven otherwise. Do not attribute a new ipsilateral facial palsy in a CSOM patient to Bell's palsy without imaging the temporal bone.
Self-Assessment: Squamosal CSOM and Mastoidectomy
At this stage of the module, consolidate the most clinically critical framework before attempting the self-check questions. Squamosal CSOM is the unsafe type: it is distinguished from mucosal CSOM by an attic or marginal perforation (not central), the presence of cholesteatoma (not mere mucosal inflammation), and a foul-smelling scanty discharge (not profuse mucoid discharge). The three types of cholesteatoma are congenital (intact TM, no prior disease), acquired primary (pars flaccida retraction pocket / invagination, no perforation), and acquired secondary (marginal perforation with epithelial ingrowth — most common). Cholesteatoma destroys bone by enzyme-mediated osteolysis, affecting the ossicles, tegmen, semicircular canals, facial nerve canal, and sigmoid sinus. The definitive investigation is HRCT temporal bone showing scutum erosion and attic soft-tissue density. Surgery is always required: the commonest procedure is modified radical mastoidectomy (MRM/Bondy), which takes down the posterior canal wall to create an open mastoid cavity. Radical mastoidectomy removes all TM and ossicles; combined approach tympanomastoidectomy preserves the canal wall but requires two stages. Ossicular reconstruction with PORP or TORP is performed when residual ossicular anatomy permits hearing rehabilitation.
Key consolidation facts:
- Unsafe type = squamosal = atticoantral = cholesteatoma = attic or marginal perforation
- Three types: congenital (intact TM), acquired primary (pars flaccida retraction — Prussak's space), acquired secondary (marginal perforation — most common)
- Bone destruction by collagenases (MMP-2, MMP-9) from cyst matrix and inflammatory reaction
- Classic CT finding: scutum erosion
- Most common ossicle eroded: long process of incus
- Most common mastoidectomy for cholesteatoma: MRM (Bondy)
- Facial palsy in CSOM = surgical emergency
- Second-look at 9-12 months in CAT (combined approach)
SELF-CHECK
A 40-year-old patient undergoes modified radical mastoidectomy (MRM) for squamosal CSOM. At 3 months post-operatively, they return with recurrent foul-smelling discharge from the cavity and a visible white mass re-forming at the attic. The most likely explanation and appropriate management is:
A. Normal post-operative granulation tissue — reassure and apply silver nitrate
B. Residual or recurrent cholesteatoma in the mastoid cavity — second-look operation with removal of residual disease
C. Post-operative chronic infection from Pseudomonas aeruginosa — treat with prolonged topical ciprofloxacin
D. Tympanosclerosis developing in the cavity — no intervention required
Reveal Answer
Answer: B. Residual or recurrent cholesteatoma in the mastoid cavity — second-look operation with removal of residual disease
Recurrent foul-smelling discharge with a visible white mass in the attic cavity at 3 months post-mastoidectomy is highly suspicious of residual or recurrent cholesteatoma — the most feared complication of cholesteatoma surgery. Cholesteatoma recurrence is common (10–30%) and occurs because microscopic squamous epithelium remnants were left behind at the first operation. Management is a second-look operation for careful removal of all residual disease. Reassurance with silver nitrate is appropriate for granulation tissue (which is red and friable), not for a white mass. While infection can occur in a mastoid cavity, the white mass and foul odour point to cholesteatoma, not simple infection.