Page 1 of 15
EN1.1 | Anatomy and Physiology of Ear, Nose, Throat, Head and Neck — SDL Guide
Learning Objectives
- Describe the anatomy of the external, middle, and inner ear, and explain the physiology of hearing and balance
- Describe the anatomy of the nasal cavity, paranasal sinuses, and the physiology of olfaction and nasal functions
- Describe the anatomy of the pharynx, tonsils, and larynx, and explain the physiology of voice, speech, and swallowing
- Describe the surgical anatomy of the head and neck including deep fascial spaces, salivary glands, cervical lymph node levels, and the thyroid gland
- Correlate anatomical knowledge with common clinical presentations in ENT
INSTRUCTIONS
The ear, nose, throat, head, and neck form a functionally and anatomically interconnected region. Mastering this anatomy is not an academic exercise — it is the foundation for every clinical decision in ENT, from understanding why a patient with tonsillitis develops earache to recognising why thyroid surgery can cause hoarseness. This module builds a systematic map of ENT anatomy and physiology that you will use throughout your clinical ENT rotation and beyond.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Chs 1–4 (Ear anatomy/physiology), Chs 17–18 (Nose/sinuses anatomy), Chs 26–28 (Throat/larynx anatomy) (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat: Diseases, 4th ed., Section I (Anatomy and Physiology) (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 1 Chs 1–6 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 12-year-old girl is brought by her mother with a 3-day history of sore throat, fever, and now — surprisingly — pain in her right ear. She has no ear discharge. On examination, both tonsils are enlarged and covered with pus. The right tympanic membrane appears mildly injected. Her mother is confused: 'Doctor, we came for the throat, why is the ear hurting?' How do you explain the referred earache? And what anatomical connections must you understand to answer that question?
WHY THIS MATTERS
ENT is a specialty that punishes anatomical ignorance more than most. The ear, nose, throat, and neck share a dense web of vascular supply, lymphatic drainage, neural interconnections, and fascial pathways — meaning that disease in one region routinely presents with symptoms in another. A dental abscess can cause earache; a nasopharyngeal tumour can obstruct the Eustachian tube and produce a middle ear effusion; a thyroid goitre can compress the recurrent laryngeal nerve and produce hoarseness. As a final-year MBBS student and future doctor, your ability to take a coherent ENT history, perform a focused ENT examination, and understand the anatomical basis of the diseases you will manage depends entirely on the foundational anatomical map you build now. The NMC EN1.1 competency is designated at the KH (Knowledge and How) level — you must not only know this anatomy but be able to explain how it underlies clinical findings and guides examination. This module is the map. Every subsequent ENT module is the journey.
RECALL
Before we map the ENT region, recall from your Year-1 anatomy (AN) and physiology (PY) what you already know. You have studied the cranial nerves — recall that CN VIII (the vestibulocochlear nerve) carries both cochlear (hearing) and vestibular (balance) fibres from the inner ear, and that CN VII (the facial nerve) travels through the temporal bone in intimate proximity to the middle ear and mastoid — making it vulnerable in ear surgery and chronic ear disease. Recall that CN IX (glossopharyngeal nerve) carries sensation from the posterior third of the tongue and the oropharynx, and that CN X (vagus nerve) gives branches to the larynx and pharynx — including the recurrent laryngeal nerves. From physiology, recall that sound is a longitudinal wave of pressure — the ear's job is to convert this mechanical pressure into electrical nerve impulses, a process requiring three mechanical stages (outer, middle, inner ear). Recall mucociliary clearance from respiratory physiology — the nose relies on the same mechanism to keep the airway clean. These Year-1 foundations will recur throughout this module.
Why ENT Anatomy Matters at the Bedside
The head and neck is arguably the most anatomically dense region of the human body — a space of roughly 15 × 15 × 15 cm housing structures responsible for hearing, balance, smell, taste, speech, swallowing, breathing, and multiple critical neurovascular pathways. What makes ENT anatomy clinically distinctive is the degree of structural interdependence: the nasopharynx communicates with the middle ear via the Eustachian tube; the paranasal sinuses drain into the nasal cavity; the pharynx serves simultaneously as an airway and a food passage; the larynx guards the trachea from aspiration during every swallow. Understanding these connections transforms a list of anatomical facts into a clinical reasoning framework.
Consider the scenario of referred otalgia — earache without primary ear disease — which affects up to 50% of patients presenting with earache. The ear receives sensory supply from five cranial nerves: CN V3 (auriculotemporal nerve, from the mandibular division of the trigeminal), CN VII (sensory fibres from the posterior EAC and concha), CN IX (Jacobson's nerve, from the middle ear mucosa), CN X (Arnold's nerve, from the EAC and auricle), and C2/C3 (greater auricular nerve). Any pathology in the distribution of these nerves — dental caries, tonsillitis, pharyngeal carcinoma, oesophageal disease, thyroid disease — can produce referred pain in the ear. In our opening case, tonsillitis produces otalgia via CN IX fibres that also carry sensation from the tonsil and Jacobson's nerve in the middle ear.
This clinical example illustrates the core principle of ENT anatomy: the region is best understood as a series of functional compartments with shared neural, vascular, and lymphatic pathways, rather than as a collection of isolated organs. Every heading in this module maps one compartment — but throughout, look for the connections that link them.
Anatomy of the Ear: External, Middle, and Inner
The ear is conventionally divided into three anatomically and functionally distinct compartments: the external ear, the middle ear, and the inner ear. Understanding each compartment precisely is the foundation for interpreting otoscopic findings, understanding hearing loss types, and grasping the surgical anatomy of ear disease.
External Ear
The pinna (auricle) is a cartilaginous framework covered by skin, shaped to collect and funnel sound. Its landmarks — helix, antihelix, tragus, antitragus, lobule — are clinically important for describing the site of lesions. The external auditory canal (EAC) is approximately 2.5 cm long in adults, with an outer cartilaginous third and an inner bony two-thirds. The junction of these two portions creates a narrow isthmus. The outer EAC is lined by skin bearing hair follicles, sebaceous glands, and ceruminous glands (modified apocrine glands producing earwax). The inner bony EAC has thin, tightly adherent skin without subcutaneous tissue, which is why furuncles here are extraordinarily painful. The EAC is angled — the canal runs anteroinferiorly in adults (hence the adult ear requires upward and backward traction to straighten it for otoscopy; in infants, the canal is more horizontal, requiring downward traction).
Tympanic Membrane (TM)
The tympanic membrane separates the EAC from the middle ear. It is pearl-grey, semi-transparent, oval, and sits obliquely (tilted at approximately 55° to the floor of the EAC). Otoscopic landmarks (essential for examination): the handle (manubrium) of the malleus runs downward and slightly anteriorly as a white streak; the lateral process of the malleus is the bright knob at the upper end of the handle; the umbo is the most depressed point at the lower tip of the handle; the cone of light (light reflex) radiates anteroinferiorly from the umbo. The TM has two regions: the pars tensa (the main drum, with three layers: outer epithelial, middle fibrous, inner mucosal) and the pars flaccida (Shrapnell's membrane — in the upper portion between the anterior and posterior malleal folds; lacks the middle fibrous layer; clinically important as the site of primary acquired cholesteatoma formation). Safe myringotomy is performed in the anteroinferior quadrant of the pars tensa (to avoid the ossicles posterosuperiorly and the jugular bulb inferiorly).
Middle Ear (Tympanic Cavity)
The middle ear is an air-filled space within the temporal bone containing the three ossicles — malleus, incus, and stapes — which transmit sound vibrations from the TM to the inner ear. The ossicular chain amplifies sound pressure: the stapes footplate at the oval window is approximately 17× smaller than the TM, so pressure is amplified approximately 17-fold (additional 1.3× from the ossicular lever arm = approximately 22× total, or ~27 dB). The tensor tympani (CN V3) muscle attaches to the malleus and stiffens the chain in response to loud sounds. The stapedius (CN VII, the smallest muscle in the body) attaches to the stapes and also stiffens the chain — stapedius reflex testing is used clinically to localise CN VII lesions. The Eustachian tube connects the middle ear to the nasopharynx (approximately 35 mm long in adults; shorter and more horizontal in children — explaining their greater susceptibility to otitis media). Its primary function is to equalise pressure between the middle ear and the atmosphere; it opens during swallowing and yawning. The mastoid antrum communicates with the middle ear posterosuperiorly through the aditus; the mastoid air cells extend from the antrum.
Critical surgical anatomy: the facial nerve (CN VII) runs through the middle ear in its tympanic segment — superior to the oval window — before turning downward in the mastoid segment. This proximity makes CN VII vulnerable in mastoid surgery and in cholesteatoma eroding the bone.
Inner Ear (Labyrinth)
The inner ear occupies the petrous temporal bone. It consists of a bony labyrinth (hard bone enclosing a perilymph-filled space) with a membranous labyrinth (floating inside, filled with endolymph) contained within it. The bony labyrinth has three parts:
1. Cochlea (hearing): a 2.75-turn spiral around the bony modiolus. Contains three fluid compartments: scala vestibuli (perilymph, connected to oval window), scala tympani (perilymph, connected to round window), and scala media/cochlear duct (endolymph). The organ of Corti sits on the basilar membrane within the scala media — it contains inner and outer hair cells (hair cells are the auditory sensory receptor cells, detecting basilar membrane vibration and converting it to electrical signals via mechanotransduction channels).
2. Vestibule (static balance): contains the saccule (detects linear acceleration and gravity, via the macular otolith membrane) and the utricle (also detects linear acceleration, particularly horizontal).
3. Semicircular canals (dynamic balance): three canals (anterior, posterior, lateral/horizontal) oriented approximately at right angles to each other; each has an expanded ampulla at one end containing the crista ampullaris (hair cells embedded in a gelatinous cupula). Movement of endolymph deflects the cupula and stimulates hair cells — detecting angular acceleration in the plane of that canal.
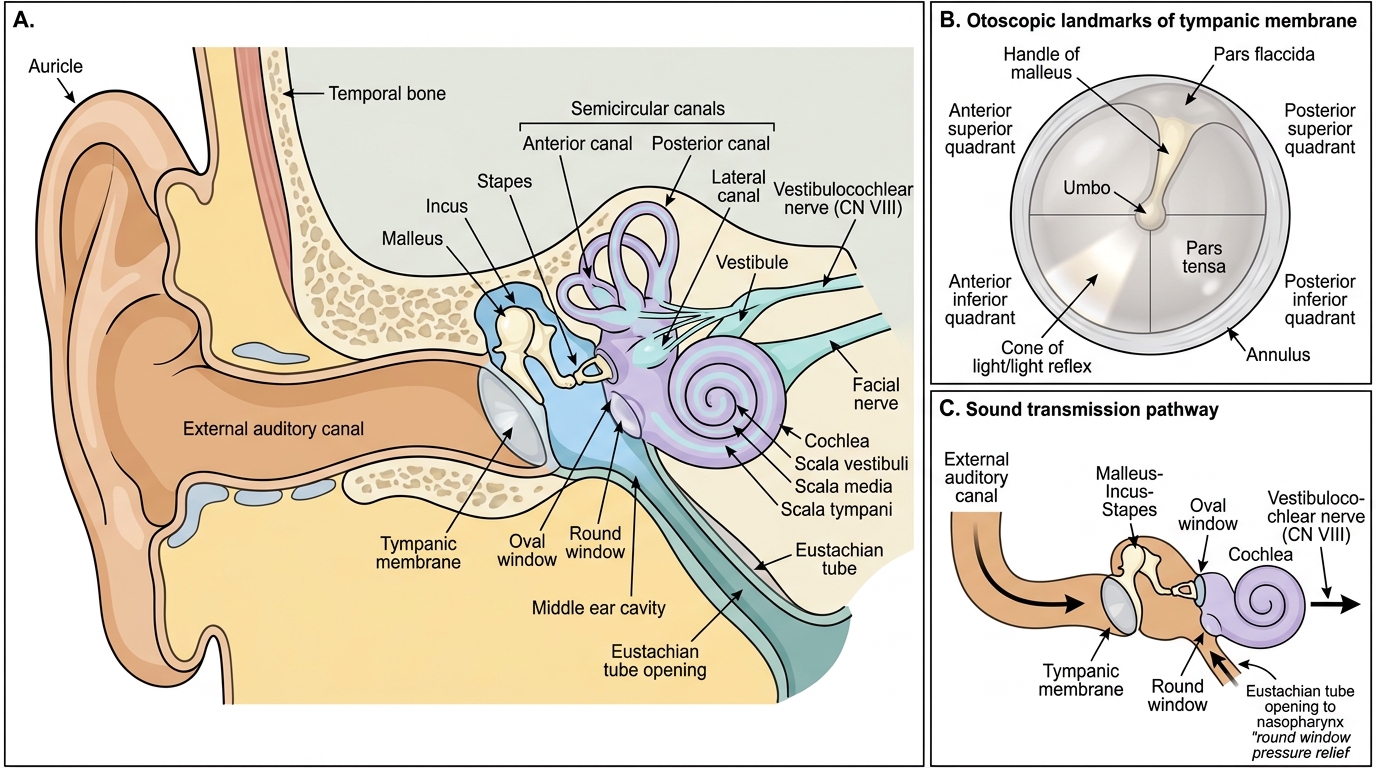
Ear Anatomy and Otoscopic Landmarks
Physiology of Hearing and Balance
Hearing and balance physiology bridge the anatomical structures just described to the clinical phenomena of hearing loss and vestibular disorders. Understanding the transduction pathway at each stage allows you to localise the site of pathology from clinical and audiological findings.
Sound Transduction — The Hearing Pathway
Sound waves entering the EAC cause the tympanic membrane to vibrate. These vibrations are transmitted mechanically through the ossicular chain — malleus → incus → stapes — to the oval window. The ossicular chain performs two critical functions: (1) impedance matching — converting low-impedance air-borne sound waves to high-impedance fluid waves in the inner ear perilymph (without this, approximately 99.9% of sound energy would be reflected at an air-fluid interface; the ossicles preserve approximately 97% of the energy); (2) amplification — the area ratio of TM to oval window (~17:1) plus the lever action of the ossicular chain (~1.3:1) provides approximately 27 dB of pressure gain.
At the oval window, stapes footplate movement sets up a travelling pressure wave in the perilymph of the scala vestibuli. This pressure wave travels up the cochlear spiral, displaces the basilar membrane at a frequency-specific point (tonotopy: high frequencies at the base of the cochlea, low frequencies at the apex), and creates a shearing motion on the hair cells of the organ of Corti. The stereocilia of hair cells are deflected, opening mechanosensitive ion channels (predominantly K+ channels), depolarising the hair cell, and triggering neurotransmitter (glutamate) release onto the afferent fibres of CN VIII (cochlear division). The signal travels to the cochlear nuclei, superior olivary complex, inferior colliculus, medial geniculate body of the thalamus, and finally to the primary auditory cortex (Heschl's gyrus) in the superior temporal lobe.
Two pathways of sound transmission exist clinically: (1) Air conduction (AC): the normal pathway just described (outer ear → TM → ossicles → oval window → cochlea). (2) Bone conduction (BC): sound vibrates the skull directly, bypassing the outer and middle ear, and stimulating the cochlea through the petrous bone. This distinction underlies the interpretation of tuning-fork tests and audiometry in hearing loss.
Vestibular Physiology — Balance
The vestibular system detects head movement and position to maintain balance and stabilise gaze. It works through two receptor types:
1. Semicircular canals (angular acceleration): The three canals detect rotation in the three planes of space. When the head rotates, inertia causes the endolymph to lag behind relative to the moving ampulla — the cupula is deflected, stimulating or inhibiting hair cells in the crista ampullaris. The lateral canal pair works together: rotation toward one side excites that side's lateral canal (cupula deflected toward utricle = utriculopetal = excitatory) and simultaneously inhibits the opposite side — this push-pull arrangement provides precise directional sensitivity.
2. Utricle and saccule (linear acceleration and gravity): The macular hair cells are embedded in an otolith membrane weighted by calcium carbonate crystals (otoliths/otoconia). Linear acceleration or tilting displaces the otoconia, shearing the hair cells. The utricle primarily detects horizontal linear acceleration; the saccule detects vertical (gravitational).
Vestibular signals travel via the vestibular division of CN VIII to the vestibular nuclei (pons/medulla), then to the cerebellum, spinal cord (vestibulospinal tracts for postural correction), and via the medial longitudinal fasciculus (MLF) to the cranial nerve nuclei controlling extraocular muscles — producing the vestibulo-ocular reflex (VOR), which keeps the gaze stable when the head moves.
SELF-CHECK
A 55-year-old man presents with gradual progressive hearing loss bilaterally. Pure-tone audiometry shows reduced air conduction thresholds in the high-frequency range with bone conduction thresholds equally reduced. Which part of the auditory pathway is most likely impaired?
A. Tympanic membrane and ossicular chain (middle ear)
B. Hair cells of the organ of Corti in the basal turn of the cochlea
C. Eustachian tube
D. Auditory cortex (Heschl's gyrus)
Reveal Answer
Answer: B. Hair cells of the organ of Corti in the basal turn of the cochlea
When both air conduction AND bone conduction thresholds are reduced equally (no air-bone gap), the problem lies in the cochlea or beyond (sensorineural hearing loss, SNHL). The basal turn of the cochlea encodes high frequencies — age-related degeneration (presbyacusis) characteristically affects high-frequency hair cells first. A middle ear problem (TM, ossicles, Eustachian tube) would reduce air conduction more than bone conduction, creating an air-bone gap (conductive hearing loss). Cortical lesions are rare causes of hearing loss and would typically present with other neurological features.