Page 2 of 15
EN1.1 | Anatomy and Physiology of Ear, Nose, Throat, Head and Neck — SDL Guide (Part 2)
Anatomy of the Nose and Paranasal Sinuses
The nose is the gateway to the respiratory tract, simultaneously performing the functions of air conditioning (heating, humidifying, filtering), olfaction, and resonance for speech. Its anatomy is complex and clinically significant — nasal obstruction, epistaxis, sinusitis, and anosmia all map precisely to identifiable anatomical structures.
The Nasal Cavity
The nasal cavity extends from the nostrils (nares) anteriorly to the posterior choanae (opening into the nasopharynx) posteriorly. It is divided by the nasal septum into right and left halves. The septum has three components: anteriorly, the quadrilateral (septal) cartilage; posterosuperiorly, the perpendicular plate of the ethmoid bone; and posteroinferiorly, the vomer. Deviation of the quadrilateral cartilage is the commonest anatomical abnormality causing nasal obstruction.
The lateral wall of each nasal cavity is the most anatomically complex surface. It bears three bony projections — the nasal turbinates (conchae): inferior turbinate (largest, most clinically relevant — mucosal engorgement here causes the most obstruction), middle turbinate, and superior turbinate. Below and lateral to each turbinate is its corresponding meatus:
- Inferior meatus: receives the nasolacrimal duct (epiphora — overflow of tears — results when this duct is blocked).
- Middle meatus: the most surgically important — contains the ostiomeatal complex (OMC), the common drainage pathway for the maxillary, anterior ethmoid, and frontal sinuses; chronic sinusitis nearly always involves OMC blockage.
- Superior meatus: drains posterior ethmoid air cells and the sphenoid sinus.
Blood Supply and Epistaxis
The nasal septum's anterior surface at the vestibule is the meeting point of five arteries forming Kiesselbach's plexus (Little's area): (1) anterior ethmoidal artery (from ophthalmic, CN V1 territory), (2) posterior ethmoidal artery, (3) sphenopalatine artery (from the maxillary artery, the main arterial supply to the posterior nose — the dominant vessel in posterior epistaxis in elderly hypertensives), (4) greater palatine artery, and (5) superior labial artery (from the facial artery). Little's area on the anterior nasal septum is the commonest site of epistaxis, particularly in children and young adults, because the mucosa here is thin and easily traumatised. Posterior epistaxis from the sphenopalatine territory occurs in elderly patients and is more serious — less visible, harder to control.
Olfactory Area
The olfactory mucosa occupies a small area at the roof of the nasal cavity: the cribriform plate of the ethmoid, the superior septum, and the upper part of the superior turbinate. Olfactory receptor neurons are bipolar neurons embedded in this specialised neuroepithelium. Their unmyelinated axons (olfactory fila) pass through approximately 20 foramina in the cribriform plate to synapse in the olfactory bulb on the floor of the anterior cranial fossa. Second-order neurons travel in the olfactory tract to the piriform (primary olfactory) cortex and the amygdala. The olfactory system is unique in reaching the cortex WITHOUT relaying in the thalamus.
Paranasal Sinuses
Four paired sinuses surround the nasal cavity and drain into it. Clinically they are remembered by the mnemonic MEFS (Maxillary, Ethmoid, Frontal, Sphenoid):
- Maxillary sinus: the largest sinus, pyramidal in shape, below the orbit. Its floor is below the nasal cavity floor — explaining why drainage is poor (the natural ostium is at the upper medial wall, above the sinus floor, making gravity drainage impossible). Floor of the maxillary sinus is in close relation to the upper molar/premolar roots — dental infections can cause maxillary sinusitis, and Caldwell-Luc surgical approach enters through the canine fossa.
- Ethmoid sinuses: a honeycomb of 8–15 air cells between the nasal cavity and the orbit, divided into anterior (drain into middle meatus) and posterior (drain into superior meatus) groups. The lamina papyracea separates the lateral ethmoid wall from the orbital fat — an important surgical landmark and route of orbital complication in ethmoiditis.
- Frontal sinus: absent at birth, develops from the anterior ethmoid cells and becomes visible on X-ray at age 5–6 years. Drains via the nasofrontal duct into the middle meatus/frontal recess. Absent in 4% of adults.
- Sphenoid sinus: occupies the body of the sphenoid bone, posterior to the nasal cavity. Its posterior wall is related to the internal carotid artery and the optic nerve — making posterior ethmoid/sphenoid surgery the most hazardous region of functional endoscopic sinus surgery (FESS).
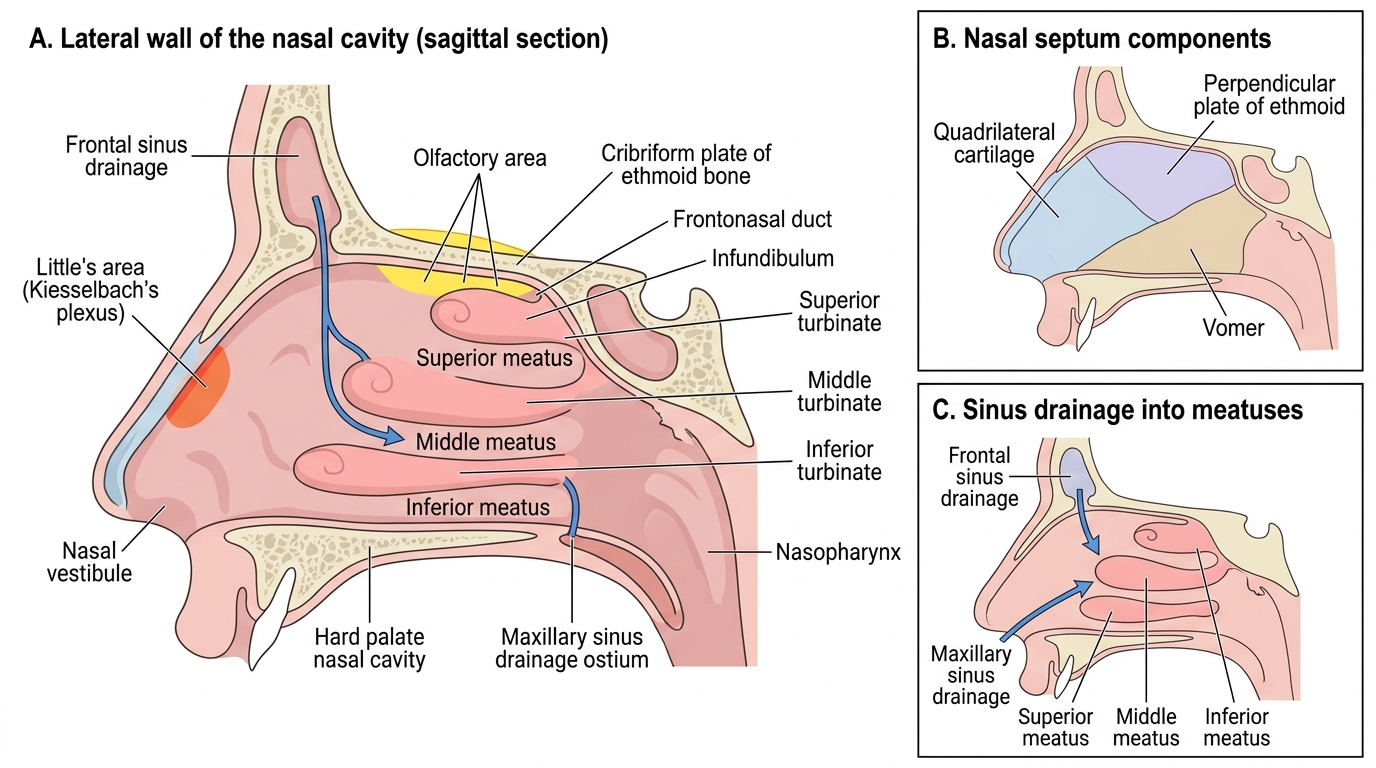
Sagittal Anatomy of the Nasal Cavity and Sinus Drainage
Physiology of Smell and Nasal Functions
The nose performs four major physiological functions beyond simply conducting air: air conditioning, olfaction, mucociliary clearance, and contributing to speech resonance. These functions depend on the precise anatomy just described, and their failure produces symptoms that ENT clinicians encounter daily. A student who understands nasal physiology is not merely memorising facts — they are building the explanatory framework for why nasal obstruction causes snoring and sleep apnoea, why chronic sinusitis leads to recurring mucopurulent rhinorrhoea, why anosmia follows head trauma involving the cribriform plate, and why the hypernasal voice of a cleft-palate patient differs from the hyponasal voice of a child with adenoid hypertrophy. Each of the four physiological functions maps to a specific anatomical substrate, and each can be assessed clinically, providing the critical link between structure and bedside observation.
Air Conditioning — Humidification, Warming, and Filtration
Inspired air is rapidly transformed as it passes through the nasal cavity. The inferior and middle turbinates are densely vascularised with a venous sinusoidal plexus — a capacitance system that can rapidly engorge or decongest, altering nasal airway resistance. This allows:
- Warming: inspired air is raised to approximately 32–34°C (near body temperature) by the time it reaches the nasopharynx.
- Humidification: the mucous membrane surface evaporates up to 1 litre of water daily into inspired air, raising humidity to approximately 90% relative humidity by the nasopharynx.
- Particle filtration: nasal hairs (vibrissae) in the vestibule filter particles >10 μm; the mucus blanket traps smaller particles (1–10 μm) which are then cleared by mucociliary transport.
Mucociliary Clearance
The entire nasal and paranasal sinus mucosa is lined by pseudostratified ciliated columnar epithelium with goblet cells, producing a two-layer mucus blanket: a periciliary sol layer (watery; the cilia beat within this layer) and an overlying gel layer (viscous; traps particles). Cilia beat at 1,000 beats per minute in a coordinated direction — posteriorly and medially toward the nasopharynx, where the mucus is swallowed or expectorated. Mucociliary transit time is approximately 20–30 minutes. Impaired mucociliary clearance (in primary ciliary dyskinesia/Kartagener syndrome, cystic fibrosis, or dry air) leads to mucus stasis, recurrent sinusitis, and respiratory infections.
Olfaction
Odorant molecules dissolve in the mucus layer overlying the olfactory epithelium and bind to specific olfactory receptor proteins on the cilia of olfactory receptor neurons. These are G-protein coupled receptors — ligand binding activates adenylyl cyclase, raises cAMP, opens cyclic nucleotide-gated ion channels, and depolarises the receptor neuron. Humans have approximately 350 functional olfactory receptor genes (the largest family of G-protein coupled receptor genes). Anosmia (loss of smell) after head trauma is classically due to shearing of olfactory fila as they pass through the cribriform plate.
Nasal Contribution to Speech
The nasal cavity and paranasal sinuses act as resonators modifying the sound produced at the larynx. The nasal consonants /m/, /n/, /ŋ/ (ng) are entirely produced by nasal resonance with the oral cavity occluded. Hyponasality (reduced nasal resonance — adenoid hypertrophy, nasal obstruction) and hypernasality (excessive nasal resonance — velopharyngeal insufficiency, cleft palate) are clinical signs of nasal/pharyngeal dysfunction detectable on speech assessment.
Anatomy of the Throat: Pharynx, Tonsils, and Larynx
The throat encompasses the pharynx and larynx — structures where the aerodigestive tract shares common pathways and then separates. The clinical consequences of disease here (aspiration, airway obstruction, dysphagia, hoarseness) reflect the anatomical precision of this sharing and separation mechanism.
The Pharynx
The pharynx is a musculomembranous tube, approximately 12–14 cm long, extending from the base of skull to the lower border of the cricoid cartilage (C6 level), where it continues as the oesophagus. It is divided into three levels: The pharynx, in particular, is a structure with no equivalent elsewhere in the body — a muscular tube that simultaneously conducts inspired air downward to the larynx and trachea, and guides swallowed food posteriorly into the oesophagus, relying on millisecond-precise laryngeal closure to prevent aspiration with every meal. Understanding the pharynx's three levels, the lymphoid tissue within it, and the laryngeal cartilaginous framework is therefore not optional anatomy — it is the prerequisite for understanding every major throat disease from tonsillitis to laryngeal carcinoma.
1. Nasopharynx (epipharynx): from the skull base to the lower border of the soft palate. Anterior communication: posterior choanae. Lateral walls: the Eustachian tube orifices (flanked by the torus tubarius — the cartilaginous ridge of the tube) and the fossa of Rosenmüller (lateral pharyngeal recess — the commonest site of nasopharyngeal carcinoma). Posterior wall/roof: the adenoid (pharyngeal tonsil) lies here on the posterior and superior walls; it is part of Waldeyer's ring.
2. Oropharynx (mesopharynx): from the soft palate to the pharyngoepiglottic folds (the level of the hyoid). Anterior communication: the oropharyngeal isthmus (bounded by the anterior faucial pillars/palatoglossal arches, the soft palate, and the posterior third of the tongue). The palatine tonsils occupy the tonsillar fossae between the anterior and posterior faucial pillars (palatoglossal and palatopharyngeal arches). Blood supply to the tonsil: primarily the tonsillar branch of the facial artery (from the external carotid artery) — with contributions from the ascending palatine, ascending pharyngeal, lingual, and dorsal lingual arteries. The external carotid artery lies just lateral to and deep to the tonsil — a critical surgical risk in tonsillectomy and peritonsillar abscess drainage.
3. Laryngopharynx (hypopharynx): from the pharyngoepiglottic folds to the lower border of the cricoid. Contains the pyriform sinuses (sinus piriformis) — lateral channels on either side of the laryngeal inlet where swallowed food is channelled around the larynx before entering the oesophagus. Hypopharyngeal carcinoma commonly arises here.
Waldeyer's Ring
The pharyngeal lymphoid tissue is arranged in a tonsillar ring at the junction of the aerodigestive tract — Waldeyer's ring — serving as a first-line immunological defence against inspired/ingested pathogens. It comprises:
- Adenoid (pharyngeal tonsil): roof and posterior wall of nasopharynx; prominent in children 3–7 years, involutes in adolescence.
- Palatine tonsils (bilateral): in the tonsillar fossae of the oropharynx; most frequently affected by tonsillitis.
- Lingual tonsil: base of tongue (posterior third).
- Tubal tonsils: near the Eustachian tube orifices in the nasopharynx.
The Larynx
The larynx occupies the midline of the neck at C3–C6 (opposite C4–C5 in adult males), suspended from the hyoid bone above and continuous with the trachea below. It serves three functions: airway protection (especially during swallowing), phonation, and contribution to cough and Valsalva. Its framework consists of nine cartilages:
- Thyroid cartilage (paired superior and inferior cornua): the largest cartilage, forming the anterior/lateral shield. The laryngeal prominence (Adam's apple) is its anterior midline fusion.
- Cricoid cartilage: the only complete ring of the larynx; the only complete ring in the airway. Signet-ring shaped — broad posteriorly, narrow anteriorly. Its posterior lamina supports the arytenoid cartilages. The cricothyroid membrane connects the inferior thyroid cartilage to the superior cricoid — the site for emergency cricothyroidotomy (NOT elective tracheostomy).
- Epiglottis: leaf-shaped, attached to the thyroid cartilage by the thyroepiglottic ligament; retroflexes during swallowing to cover the laryngeal inlet and divert food into the pyriform sinuses.
- Arytenoid cartilages (paired): sit on the posterior cricoid lamina; their vocal processes anchor the posterior end of the vocal cords; their muscular processes are attachment sites for the intrinsic laryngeal muscles that abduct, adduct, and tense the cords.
- Corniculate and cuneiform cartilages (paired): small, in the aryepiglottic folds; create the aryepiglottic eminences visible on indirect laryngoscopy.
Laryngeal Compartments
- Supraglottis (above the true vocal cords): contains the epiglottis, aryepiglottic folds, false vocal folds (vestibular folds), and the laryngeal ventricles. Rich lymphatic drainage → early nodal spread of supraglottic carcinoma.
- Glottis (vocal folds): the true vocal cords and the anterior/posterior commissures. The glottis is the anatomical level where phonation occurs. The glottic region has minimal lymphatic drainage — explaining why glottic carcinoma presents early with hoarseness but has excellent prognosis before nodal spread.
- Subglottis (below the true cords to the lower cricoid margin): the narrowest part of the paediatric airway (the cricoid ring limits expansion — critical in subglottic croup and foreign body lodgement).
Nerve Supply of the Larynx
All laryngeal structures are supplied by branches of the vagus nerve (CN X) via the superior laryngeal nerve (SLN) and the recurrent laryngeal nerve (RLN):
- SLN: divides into the internal branch (sensory to the supraglottis and epiglottis, enters the thyrohyoid membrane) and the external branch (motor to the cricothyroid muscle only — the only intrinsic laryngeal muscle NOT supplied by the RLN; tenses the vocal cord to change pitch).
- RLN: supplies motor fibres to all other intrinsic laryngeal muscles (posterior cricoarytenoid — the only abductor of the vocal cords; lateral cricoarytenoid, interarytenoid, thyroarytenoid). The RLN has an important asymmetrical course: the left RLN loops under the arch of the aorta (a long intrathoracic course), while the right RLN loops under the right subclavian artery (a shorter course). This explains why the left RLN is more frequently injured by mediastinal pathology (aortic aneurysm, lung carcinoma, mediastinal lymphadenopathy).
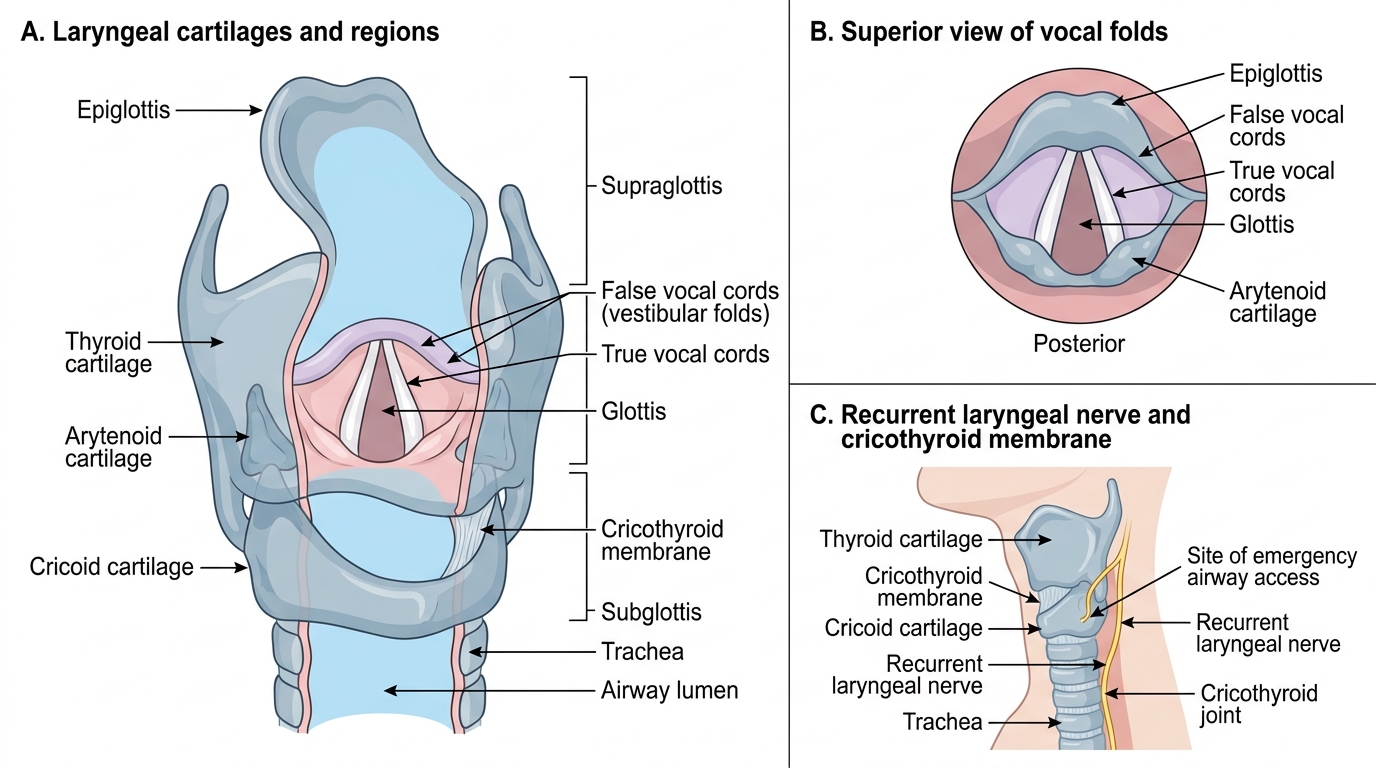
Laryngeal Cartilages, Vocal Folds, and Nerve Supply