Page 8 of 20
EN4.36 | Deep Neck Space Infection — SDL Guide
Learning Objectives
- Describe the clinical features of deep neck space infections including Ludwig's angina, parapharyngeal abscess, and retropharyngeal abscess
- Identify the anatomical basis for deep neck space infections — fascial planes, spaces, and pathways of spread
- Select and interpret appropriate investigations including CT neck with contrast for deep neck space infection
- Outline the principles of management including airway management, antibiotics, and surgical drainage
- Recognise life-threatening complications including mediastinitis, jugular vein thrombosis, and carotid artery erosion
INSTRUCTIONS
Deep neck space infection is one of the most serious and potentially fatal conditions in head and neck surgery. A seemingly innocuous dental infection, tonsillar abscess, or pharyngeal foreign body can spread through the fascial planes of the neck into deep spaces and from there to the mediastinum — a process that can be rapid and life-threatening. The management requires simultaneous airway control, aggressive antibiotic therapy, and prompt surgical drainage. At the MBBS level, competency EN4.36 requires you to describe the clinical features, investigations, and management principles — with the understanding that early recognition and timely referral or escalation can be the difference between a successful outcome and a fatal complication.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose & Throat, 8th ed., Chapter: Deep Neck Space Infections (textbook)
- Hazarika P — Textbook of Ear, Nose & Throat, 4th ed., Chapter on Deep Space Infections of the Neck (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Chapter: Deep Neck Space Infection (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man is brought to the emergency department by his family at 2 AM. He had a toothache for five days, took analgesics and ignored it. Over the past 24 hours he developed a painful swelling in the floor of his mouth and under his chin, his speech became muffled, and he is now drooling and leaning forward because lying flat makes his breathing worse. On examination he is febrile at 39.2°C, tachycardic, and looks anxious. The floor of his mouth is elevated and brawny-hard on palpation — there is no fluctuance and no pus. His neck is thick and tender bilaterally. His oxygen saturation is 96% on room air. The anaesthetist looks at his neck and says quietly to you: 'I'm not sure I can intubate this.' This is Ludwig's angina — a bilateral submandibular, sublingual, and submental space infection — and the airway is in immediate danger.
WHY THIS MATTERS
Deep neck space infections represent one of the true surgical emergencies in otorhinolaryngology and head and neck surgery. The neck contains multiple fascial compartments that communicate with each other and with the mediastinum through defined anatomical pathways — and infection that gains entry to these spaces can spread rapidly and silently, causing life-threatening airway compromise, mediastinitis, septic thrombophlebitis of the jugular vein (Lemierre's syndrome), or erosion of the carotid artery. The incidence of deep neck space infections has declined in the antibiotic era, but it has not disappeared — dental neglect, immunosuppression (HIV, diabetes, malnutrition), intravenous drug use, and delayed treatment continue to produce severe cases. Understanding the anatomy of the deep cervical fascial spaces and the clinical signs of each space's involvement is essential for any doctor who may encounter these patients — in emergency departments, general practice, or specialist settings. Early surgical drainage before airway compromise is established is associated with significantly better outcomes than emergency airway management in an infected, distorted, difficult airway.
RECALL
Bring to mind the deep cervical fascia and its compartments from your anatomy studies. The deep fascia of the neck is organised into three layers. The investing (superficial) layer of the deep cervical fascia is the outermost, enclosing the sternocleidomastoid, trapezius, and the infrahyoid strap muscles. The pretracheal (middle) layer has two parts: the muscular part enclosing the infrahyoid muscles, and the visceral part enclosing the thyroid, trachea, and oesophagus. The prevertebral (deep) layer covers the prevertebral muscles and the vertebral column. Between the visceral layer of the pretracheal fascia and the prevertebral fascia lies the retropharyngeal space — a potential space that runs from the skull base to the posterior mediastinum. Behind the prevertebral fascia but anterior to the vertebral bodies lies the danger space (or alar space) — a direct fascial pathway from the skull base to the diaphragm along which infections can descend into the mediastinum with alarming speed. The parapharyngeal space is an inverted cone-shaped space lateral to the pharynx that communicates with the retropharyngeal space, the pterygoid space, and the carotid sheath.
Clinical Presentation of Deep Neck Space Infection
The clinical presentation of deep neck space infection depends on which space is involved, and each space produces a characteristic symptom cluster that the clinician must recognise. The unifying features across all deep neck infections are pain, swelling, fever, and evidence of systemic sepsis — but the specific anatomical location determines the additional cardinal signs.
Ludwig's angina (bilateral submandibular/sublingual/submental infection) presents with floor of mouth swelling and elevation, trismus (inability to open the mouth >30 mm inter-incisal distance, from masseter and pterygoid spasm), dysarthria (hot-potato voice), dysphagia, and drooling. The characteristic finding on palpation is brawny, board-like induration of the floor of the mouth and submandibular region bilaterally without fluctuance — the infection spreads diffusely through the fascial spaces rather than collecting as a discrete abscess. As the floor of the mouth elevates, the tongue is pushed upward and posteriorly, threatening the airway from above. This is the most feared deep neck infection because of the high risk of sudden airway loss.
Parapharyngeal abscess presents with trismus, dysphagia, muffled voice, deviation of the lateral pharyngeal wall and tonsil medially (medial bulge in the tonsillar fossa), stiff neck (torticollis), and unilateral neck swelling posterior to the angle of the mandible. The parapharyngeal space is divided by the styloid process into the pre-styloid compartment (fat, salivary gland, lymph nodes) and the post-styloid compartment containing the carotid sheath — involvement of the post-styloid compartment risks carotid artery erosion and internal jugular vein thrombosis.
Retropharyngeal abscess is most common in children under 6 years (because the retropharyngeal lymph nodes that drain the posterior nasopharynx and adenoids are present in early childhood and involute by age 5–6). Presentation includes fever, refusal to eat, hyperextension of the neck (child holds neck in extension to maximise airway), drooling, stridor, and a bulging posterior pharyngeal wall visible on examination. In adults, retropharyngeal infection usually results from trauma (foreign body, instrumentation) or spread from vertebral osteomyelitis.
Danger space infection (spread through the alar space) is the complication most feared after any deep neck space infection — it presents as worsening sepsis, chest pain, and signs of mediastinitis out of proportion to the neck swelling.
Anatomy of the Deep Neck Spaces and Fascial Planes
A clear mental map of the deep neck spaces and their communications is the foundation for understanding how infections spread and why certain complications occur with such speed and severity. The deep cervical fascial system creates compartments — and infection, like water, fills those compartments and finds pathways to adjacent ones. Without this anatomical framework, the clinical behaviour of deep neck infections seems unpredictable; with it, every clinical sign and radiological finding makes immediate sense. Understanding the specific spaces, their boundaries, and their communications with each other and with the mediastinum is the key to understanding why a dental infection can cause a pleural effusion, and why surgery for Ludwig's angina requires bilateral decompression rather than a single incision.
The parapharyngeal space is the central crossroads of deep neck anatomy. It is an inverted cone-shaped potential space with its base at the skull base and apex at the hyoid bone. It is bounded medially by the pharyngeal constrictors, laterally by the medial pterygoid muscle and the parotid gland fascia, anteriorly by the pterygomandibular raphe, and posteriorly by the prevertebral fascia. The styloid process and its muscles divide the parapharyngeal space into:
- Pre-styloid compartment: contains fat, the deep lobe of the parotid, and lymph nodes.
- Post-styloid compartment (carotid space): contains the internal carotid artery, internal jugular vein, CN IX–XII, and the cervical sympathetic chain.
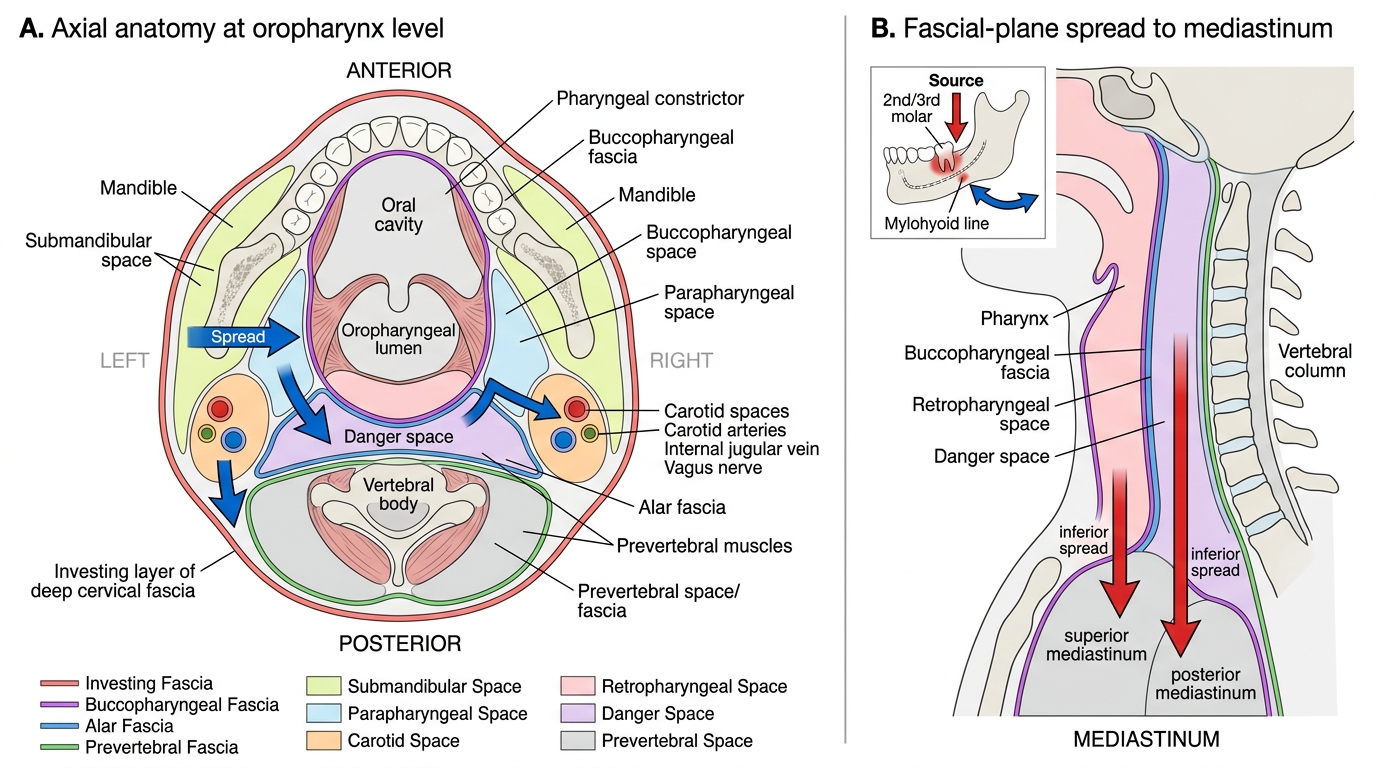
The retropharyngeal space lies between the posterior pharyngeal wall (buccopharyngeal fascia) anteriorly and the prevertebral fascia posteriorly. It extends from the skull base superiorly to the level of T1–T2 inferiorly, where it communicates with the posterior mediastinum. In children it contains retropharyngeal lymph nodes that drain the posterior nasopharynx; these involute by age 5–6, explaining why retropharyngeal abscess is predominantly a childhood disease.
The danger space (alar space) lies between the alar fascia (anterior layer) and the prevertebral fascia (posterior layer). Because the alar fascia fuses with the carotid sheath laterally only at the level of C7, the danger space has no lateral boundaries above this level — infection can descend from the skull base to the posterior mediastinum (the diaphragm level) without resistance. This direct pathway explains the devastating speed of mediastinal spread in retropharyngeal and posterior deep neck infections.
The submandibular space is bounded superiorly by the mucosa of the floor of the mouth and inferiorly by the investing fascia of the neck. The mylohyoid muscle divides it into the sublingual space (above) and the submandibular space proper (below), but the two communicate at the posterior edge of mylohyoid — meaning infection in one compartment readily spreads to the other. Both sublingual spaces and the submental space communicate, explaining the bilateral involvement in Ludwig's angina.
Deep Neck Fascial Spaces and Infection Spread
Pathophysiology: How Infections Spread in the Deep Neck
The mechanism of infection spread in the deep neck is primarily along fascial planes rather than through tissue destruction — which is why infections can reach distant anatomical sites before the external signs of severity become apparent. This 'silent spread' through fascial planes is what makes deep neck infections treacherous.
The most common source of deep neck space infection is odontogenic infection, accounting for approximately 40–50% of cases in most surgical series. Infections arise from the apical periodontium of mandibular teeth (most commonly the second and third molars, whose roots lie below the mylohyoid line and thus drain directly into the submandibular space) and spread through the buccal or lingual cortex of the mandible. From the submandibular space, infection can spread to the parapharyngeal, retropharyngeal, or pretracheal spaces depending on which fascial planes are violated.
The causative organisms are typically polymicrobial — a mixed aerobic-anaerobic flora reflecting the oral cavity's bacterial ecology. The predominant aerobes are viridans streptococci (Streptococcus milleri group — specifically S. anginosus, S. constellatus, and S. intermedius, collectively known for abscess formation). The anaerobes include Peptostreptococcus, Prevotella, Porphyromonas, and Fusobacterium species. Aerobic-anaerobic synergy — where each group creates conditions that enhance the virulence of the other (aerobes consume oxygen, creating the reduced microenvironment that favours anaerobic growth; anaerobes produce enzymes that impair phagocytosis) — dramatically accelerates tissue necrosis and spread.
Tonsillar and peritonsillar sources are the second most common, accounting for spread from quinsy (peritonsillar abscess) into the parapharyngeal space through the superior pharyngeal constrictor. Foreign body, iatrogenic (post-tonsillectomy, endoscopy, intubation) trauma, salivary gland infections, and lymphadenitis are other sources. Lemierre's syndrome (septic thrombophlebitis of the internal jugular vein due to Fusobacterium necrophorum following pharyngitis) is a specific form of deep neck sepsis with metastatic septic emboli to the lungs, joints, and long bones — it predominantly affects healthy young adults.
Once infection reaches the danger space, its descent to the mediastinum is rapid and can occur within hours. Descending necrotising mediastinitis (DNM) is the most lethal complication of deep neck infection, with a mortality of 20–40% even with aggressive surgical management.
SELF-CHECK
A 10-year-old child presents with high fever, refusal to eat, hyperextension of the neck, and mild inspiratory stridor. On oral examination, a smooth bulging of the posterior pharyngeal wall is visible, pushing the soft palate anteriorly. The most likely diagnosis and appropriate next investigation are:
A. Peritonsillar abscess; needle aspiration under local anaesthesia
B. Retropharyngeal abscess; CT neck with contrast
C. Ludwig's angina; OPG dental panoramic X-ray
D. Parapharyngeal abscess; MRI neck
Reveal Answer
Answer: B. Retropharyngeal abscess; CT neck with contrast
This is a classic presentation of retropharyngeal abscess in a child: fever, neck hyperextension (to maintain airway patency), stridor, and a smooth bulge of the posterior pharyngeal wall. The retropharyngeal lymph nodes (which drain the posterior nasopharynx and adenoids) are present in children and involute by age 5–6, explaining the childhood predominance. The gold-standard investigation is CT neck with contrast, which distinguishes retropharyngeal cellulitis (rim enhancement without central hypodensity) from an abscess (rim-enhancing hypodense collection), guiding the decision between IV antibiotics alone versus surgical drainage. Peritonsillar abscess presents laterally (displaced tonsil, uvular deviation) not posteriorly. MRI is excellent for soft tissue but is impractical in an acutely unwell child and does not visualise bony detail.