Page 9 of 20
EN4.36 | Deep Neck Space Infection — SDL Guide (Part 2)
Clinical Features and Examination of Deep Neck Space Infection
Recognising deep neck space infection demands systematic clinical assessment, because the superficial examination alone will significantly underestimate the extent of the disease. The infection lies within fascial spaces deep to the skin and superficial musculature — external signs may be misleading or late to appear. The approach must be structured and must always include an airway assessment as the first priority.
General assessment — airway first:
Before examining the neck, assess the airway. Is the patient phonating normally or with a muffled 'hot-potato' voice (suggesting pharyngeal wall displacement)? Is there drooling (inability to swallow secretions = serious pharyngeal/supraglottic involvement)? Is there stridor (inspiratory = supraglottic/glottic obstruction)? Is the oxygen saturation compromised? Any of these signs mandates an immediate call for anaesthetic assistance and preparation for emergency airway management.
Systemic signs: Fever, tachycardia, and rigors indicate sepsis. Haemodynamic instability (hypotension, low urine output) indicates severe systemic involvement.
Neck examination:
- Inspection: neck swelling, its site (submandibular = Ludwig's; posterior to angle of mandible = parapharyngeal; midline/posterior = retropharyngeal), skin erythema, neck stiffness (torticollis = parapharyngeal or retropharyngeal involvement).
- Palpation: tenderness, consistency (brawny non-fluctuant induration = Ludwig's; fluctuant = abscess), extent of induration.
- Trismus: inability to open the mouth — measured as the inter-incisal distance. Trismus (<30 mm inter-incisal) indicates masticator or parapharyngeal space involvement.
Oral and pharyngeal examination:
- Floor of mouth: elevation and induration (Ludwig's).
- Tonsils: displaced medially by a lateral parapharyngeal bulge, or a direct tonsillar abscess with uvular deviation (peritonsillar).
- Posterior pharyngeal wall: bulging = retropharyngeal abscess.
- Indirect laryngoscopy (or flexible nasolaryngoscopy if available): assess supraglottis, epiglottis, and pyriform sinuses for oedema or deviation.
| Space | Cardinal Signs | Airway Risk |
|---|---|---|
| Ludwig's angina | Bilateral submandibular induration, floor of mouth elevation, tongue displacement | Very high |
| Parapharyngeal | Trismus, medial tonsillar displacement, neck swelling at angle of jaw | Moderate–high |
| Retropharyngeal | Neck hyperextension, posterior pharyngeal bulge, stridor | High (children) |
| Danger space | Chest pain, mediastinal signs, worsening sepsis | — |
Investigations for Deep Neck Space Infection
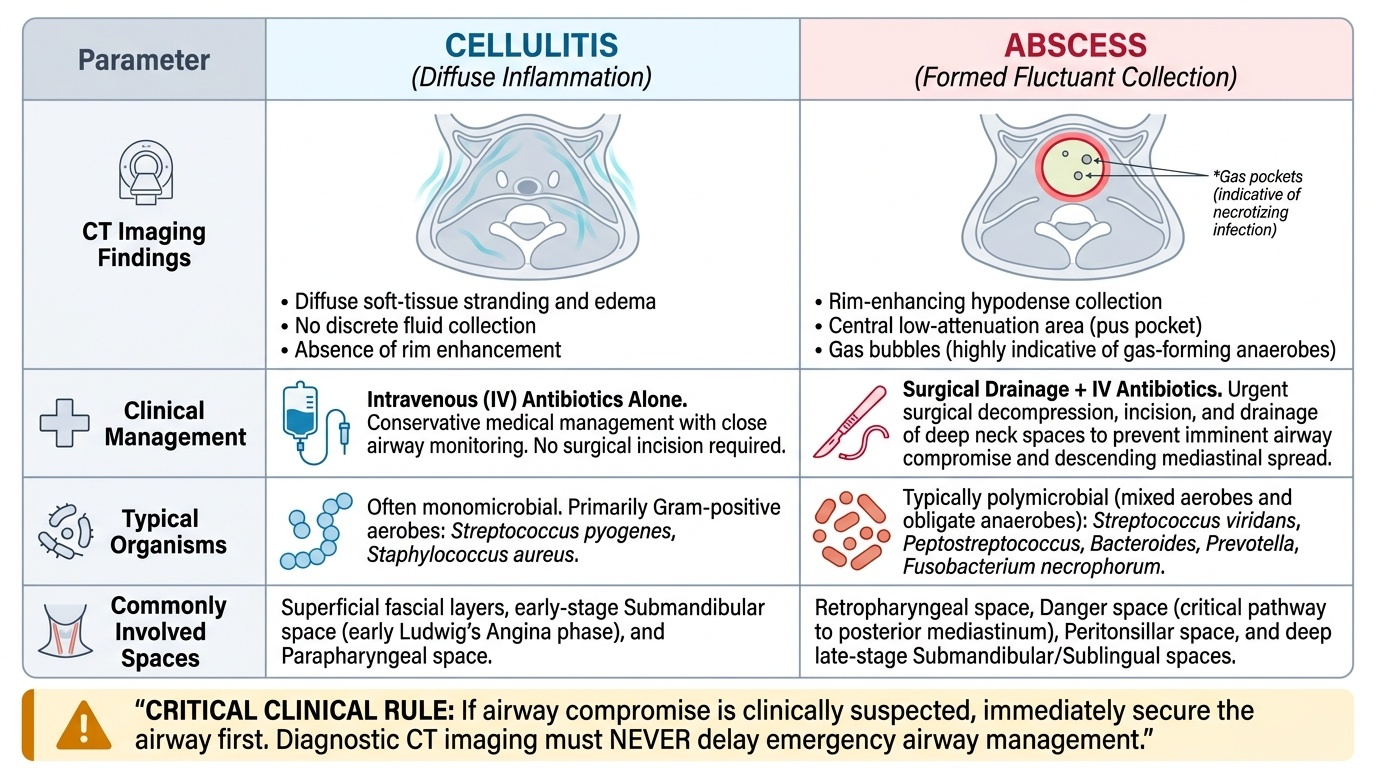
Investigation selection in deep neck space infection is driven by the need to answer three critical questions: Is there a formed abscess or only diffuse cellulitis? How far has the infection spread — has it reached the retropharyngeal space or entered the danger space towards the mediastinum? Is the airway narrowed or compromised? The answers to these three questions determine whether the patient needs surgery, the extent of surgery required, and the urgency of airway management. The investigations below are chosen specifically to address these questions, ordered from the most time-critical to the adjunctive. In a patient with overt airway compromise, the airway must be secured before imaging — CT must never delay emergency airway management.
Provided image
CT neck with contrast is the gold standard investigation for deep neck space infection. It is fast (minutes), widely available, and provides precise answers to all three questions. The key CT findings are:
- Cellulitis: soft-tissue stranding and oedema without a discrete low-density collection.
- Abscess: a rim-enhancing hypodense collection (ring of enhancement around a central low-attenuation area representing pus). The presence of gas within the collection (gas-forming organisms) is a sign of severe necrotising infection.
- CT maps the full extent of infection — which spaces are involved, whether there is retropharyngeal spread approaching the mediastinum, mediastinal extension (dense streaking in the superior mediastinum, pleural effusion), and whether the carotid sheath is involved.
- CT also demonstrates airway narrowing — deviation or compression of the trachea and subglottis.
Full blood count and inflammatory markers: FBC (leukocytosis = bacterial infection, neutrophilia + band forms = severe sepsis), CRP and ESR (markedly elevated), serum albumin (low albumin = poor nutritional state, predicts complicated course).
Blood cultures: should be obtained before antibiotics — positive in 10–20% of cases, guides definitive antimicrobial therapy.
Dental panoramic X-ray (OPG) or intraoral periapical X-ray: to identify the odontogenic source — periapical abscess, caries extending to the root tip, or alveolar bone loss. Should not delay CT or airway management.
Chest X-ray: for all patients — look for superior mediastinal widening, pleural effusion, and pneumomediastinum as signs of descending mediastinitis.
Wound swab / pus culture: obtained at surgical drainage — culture-directed antibiotic therapy is important in a polymicrobial infection.
SELF-CHECK
A 40-year-old diabetic man presents with right submandibular swelling, trismus, and a CT neck with contrast that shows a rim-enhancing collection in the right parapharyngeal space extending inferiorly to the retropharyngeal space. He has been on IV amoxicillin-clavulanate for 36 hours with no improvement. His oxygen saturation is 98% and he can maintain his airway. The most appropriate next step is:
A. Continue IV antibiotics for another 48 hours and repeat CT
B. Add IV metronidazole to cover anaerobes and observe
C. Surgical drainage of the parapharyngeal and retropharyngeal collections under general anaesthesia
D. Needle aspiration under local anaesthesia as a temporising measure
Reveal Answer
Answer: C. Surgical drainage of the parapharyngeal and retropharyngeal collections under general anaesthesia
This patient has a confirmed CT abscess with extension to the retropharyngeal space, failure of 36 hours of broad-spectrum IV antibiotics (co-amoxiclav covers both aerobes and anaerobes), and a concurrent risk factor for aggressive polymicrobial infection (diabetes). The indications for surgical drainage are met: confirmed abscess on CT + failure to respond to IV antibiotics. Continuing antibiotics alone risks further spread — the retropharyngeal extension already creates a pathway to the mediastinum via the danger space. Needle aspiration is inadequate for a deep-space parapharyngeal abscess (access is poor, incomplete drainage, and risk of vascular injury). Surgery should include transoral or transcervical drainage depending on accessibility, with careful attention to the carotid sheath. The airway should be secured (preferably awake fibreoptic intubation or tracheostomy under local anaesthesia) before the definitive drainage procedure.
Diagnosis and Differential Diagnosis
The diagnosis of deep neck space infection is primarily clinical and radiological, but the differential diagnosis must be considered carefully to avoid mismanagement. The most important distinction is between deep neck infection and other causes of neck swelling and pain that do not require surgical drainage, and between the different deep space syndromes with their differing urgency profiles.
Differentiating the specific deep neck space syndromes:
Ludwig's angina is distinguished from a submandibular lymph node abscess by the bilateral involvement, floor of mouth elevation, absence of discrete fluctuance, and the brawny non-pitting induration. A submandibular lymph node abscess is typically unilateral, fluctuant, and does not produce floor of mouth elevation or trismus.
Peritonsillar abscess (quinsy) is often confused with parapharyngeal abscess. In peritonsillar abscess, the tonsil and soft palate are displaced medially, the uvula deviates to the contralateral side, and there is hot-potato voice, drooling, and severe odynophagia — but the infection is confined to the peritonsillar space and does not produce a neck mass or trismus to the same degree as parapharyngeal infection. On CT, peritonsillar abscess does not extend lateral to the pharyngeal constrictors.
Epiglottitis (Haemophilus influenzae type b in unvaccinated children, mixed organisms in adults) presents with sudden onset sore throat, high fever, muffled voice, drooling, and stridor — and can mimic retropharyngeal abscess. Laryngoscopy shows a cherry-red oedematous epiglottis. CT is not the initial investigation for suspected epiglottitis (risk of precipitating airway obstruction during the procedure).
Complications to recognise:
- Mediastinitis (descending necrotising mediastinitis): worsening sepsis + chest pain + CT showing mediastinal oedema/gas/fluid. Requires thoracic surgical consultation.
- Lemierre's syndrome: IJV thrombosis post-pharyngitis → septic emboli to lungs (bilateral nodular infiltrates/cavitation on CXR) + metastatic septic arthritis. Diagnosis = CT venography + blood culture for Fusobacterium.
- Carotid artery erosion: sudden massive haemorrhage from the neck or oropharynx in a patient with parapharyngeal or retropharyngeal infection — an immediately life-threatening complication.
CLINICAL PEARL
The airway in deep neck infection must be secured BEFORE the patient deteriorates — not after. An anticipated difficult airway in an elective setting is managed with an awake fibreoptic intubation or awake tracheostomy under local anaesthesia. A patient with Ludwig's angina or parapharyngeal abscess who loses their airway in the emergency department has a catastrophically difficult airway — brawny induration, trismus, and pharyngeal wall displacement make standard laryngoscopy nearly impossible. The rule is: if you can see airway compromise coming, manage it now, in a controlled setting. Waiting until the saturation falls is waiting too long.