Page 1 of 20
EN4.30 | Head and Neck Trauma — SDL Guide
Learning Objectives
- Describe the clinical features of common head and neck injuries including ear, nasal, laryngeal, and neck trauma
- Explain the pathophysiology and anatomical basis of temporal bone fractures, septal haematoma, and penetrating neck trauma
- Outline the systematic ENT examination and appropriate investigations following head and neck trauma
- Distinguish between longitudinal and transverse temporal bone fractures on clinical and radiological grounds
- Describe the principles of management of ear, nasal, laryngeal, and neck injuries, including emergency airway management
INSTRUCTIONS
Head and neck trauma encompasses a broad spectrum of injuries — from a footballer's pinna haematoma to a road traffic accident victim with a shattered larynx and expanding neck haematoma threatening the airway. The ENT surgeon is called upon in every setting, often urgently. Understanding the anatomical basis of these injuries and the principles of management allows you to prioritise correctly, prevent complications such as saddle-nose deformity and facial nerve palsy, and recognise when surgical intervention is immediately life-saving. EN4.30 requires you to describe the clinical features, investigations, and management principles across this entire domain.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 28: Injuries of the Ear; Ch. 38: Trauma to the Nose; Ch. 49: Trauma to the Larynx and Trachea (textbook)
- Hazarika P — Textbook of ENT and Head-Neck Surgery, 4th ed., Ch. 25: Head and Neck Trauma (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 2, Ch. 89: Temporal Bone Trauma; Ch. 137: Laryngeal Trauma (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old motorcyclist is brought to the emergency department after a high-speed collision. He has a Glasgow Coma Scale of 14/15, and the trauma team has completed the primary ATLS survey — airway clear, breathing adequate, circulation controlled with one IV line. The ENT registrar is called because he has blood trickling from his right ear, bruising behind his right ear (Battle's sign), a deviated nose with a left-sided septal swelling, and hoarse, stridulous breathing. His neck is immobilised in a collar. Which of these ENT findings is immediately life-threatening, and which can wait? What do you assess first, and why?
WHY THIS MATTERS
Injuries to the head and neck region are encountered in every clinical setting — road traffic accidents, assault, sports injuries, blast injuries, and iatrogenic trauma from intubation or rigid endoscopy. In India, road traffic accidents account for a large proportion of maxillofacial and ENT trauma; sports injuries (boxing, wrestling, cricket) and occupational trauma (machinery, falls) add to the burden. The ENT surgeon's role is dual: first, as part of the trauma team addressing airway, vascular, and neurological emergencies; second, as a specialist managing subacute and elective complications (hearing loss from temporal bone fractures, septal deformity from missed haematoma, voice changes from laryngeal injury). NMC competency EN4.30 is a KH (Knows How) level skill — you must not only know the facts but understand the clinical reasoning behind management priorities. Missing a septal haematoma leads to permanent saddle-nose deformity; missing a penetrating neck injury leads to death. These are preventable tragedies if the correct assessment is done.
RECALL
Before proceeding, recall from your anatomy sessions: the temporal bone contains the middle ear and inner ear, and the facial nerve traverses it in the Fallopian canal (from the geniculate ganglion through the mastoid segment to the stylomastoid foramen). The nasal septum consists of the quadrilateral cartilage anteriorly, the vomer posteriorly, and the perpendicular plate of the ethmoid superiorly; the septal perichondrium provides the avascular cartilage with its blood supply. The laryngeal skeleton comprises the thyroid, cricoid, and arytenoid cartilages — the cricoid is the only complete ring in the airway. The neck is divided into three surgical zones for penetrating trauma: Zone I (below the cricoid to thoracic inlet), Zone II (cricoid to angle of mandible), and Zone III (above the angle of mandible to skull base). Recall from physiology that the vestibulo-cochlear nerve and cochlea are sensitive to concussive and barotraumatic forces, explaining sensorineural hearing loss after temporal bone fractures.
Clinical Presentations of Head and Neck Trauma
Head and neck trauma presents across a wide spectrum of severity, and the initial clinical assessment must rapidly triage life-threatening from non-life-threatening injuries. Understanding the characteristic presentations of each anatomical region allows the clinician to anticipate complications and avoid delays in intervention.
Ear and temporal bone injuries typically follow blunt head trauma, barotrauma, or penetrating wounds. The patient may report blood from the ear (otorrhagia), hearing loss, tinnitus, vertigo, or facial weakness. On examination, a haematoma auris (cauliflower ear) presents as a fluctuant, bluish swelling over the pinna after a direct blow — the blood collects between the perichondrium and auricular cartilage. Traumatic tympanic membrane (TM) perforation presents with sudden ear pain, hearing loss, and otorrhagia, typically after a blast, direct slap to the ear, or barotrauma during diving or air travel. When basal skull fracture involves the temporal bone, CSF otorrhoea — clear or blood-mixed fluid from the ear — and Battle's sign (postauricular bruising, appearing 24–48 hours after injury) are pathognomonic. Bleeding from the ear in the absence of external canal laceration strongly suggests a temporal bone fracture.
Nasal injuries are the most common facial fractures. The patient presents with nasal pain, swelling, epistaxis, and deformity. The critical examination finding in all nasal injuries is inspection of the nasal septum: a septal haematoma presents as a smooth, bilateral or unilateral, bluish, fluctuant swelling obscuring the normal mucosal markings — it is often painful to palpation. It must not be confused with a deviated septum. If missed, septal haematoma organises and undergoes avascular necrosis, resulting in the permanent "saddle-nose" deformity.
Laryngeal and tracheal injuries present with hoarseness, dysphonia, dyspnoea, stridor, subcutaneous emphysema of the neck, and haemoptysis. The severity ranges from minor mucosal contusion (managed conservatively) to cricotracheal separation (surgical emergency). Blunt trauma — a steering wheel, strangulation, or a direct blow — is the most common mechanism in civilian practice. A patient with stridor after neck trauma has a compromised airway until proven otherwise.
Penetrating neck injuries range from low-velocity stab wounds to high-velocity gunshot wounds. The clinical presentation depends on the zone of injury and structures involved. Hard signs of vascular injury (active haemorrhage, expanding haematoma, absent distal pulse, bruit) or aerodigestive injury (subcutaneous emphysema, dysphagia, haemoptysis) indicate immediate surgical exploration. Soft signs (stable haematoma, minor haemoptysis) allow further imaging.
Anatomy Relevant to Head and Neck Trauma
The pattern of injury in head and neck trauma is dictated by the local anatomy — the position of structures, their rigidity, their proximity to vital neurovascular elements, and the direction of force applied.
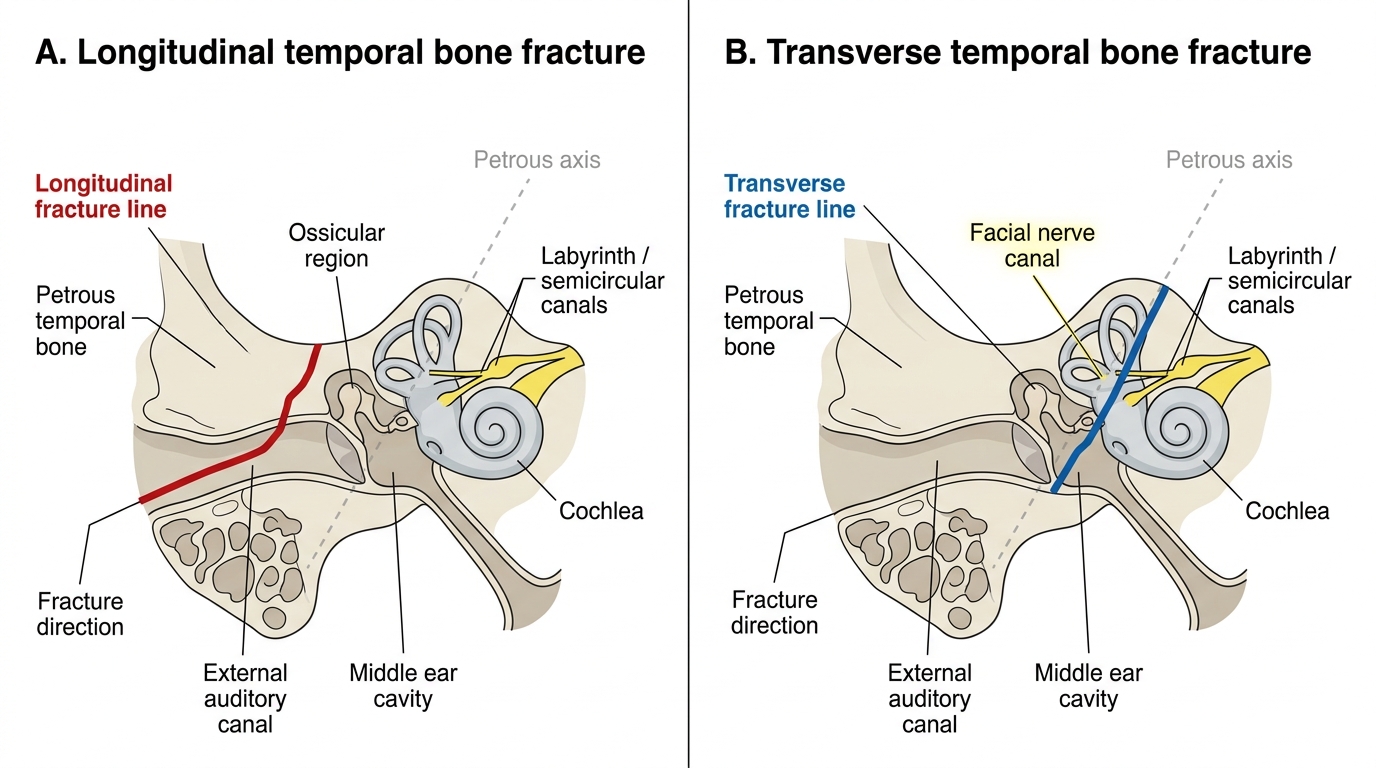
The temporal bone has a complex architecture. The petrous portion houses the bony labyrinth (cochlea and semicircular canals), the internal auditory canal (with the facial and vestibulocochlear nerves), and the middle ear with ossicular chain. The squamous portion forms the lateral skull wall and the roof of the external auditory canal. Fractures follow lines of weakness determined by the direction of force applied to the skull: a blow to the temporoparietal skull drives a fracture line parallel to the long axis of the petrous bone (longitudinal fracture), passing through the squamous temporal bone, roof of the EAC, middle ear, and then running anterior to the labyrinth toward the petrous apex. A blow to the occiput or frontal bone drives the force transverse to the petrous axis (transverse fracture), crossing directly through the labyrinth. This anatomical distinction determines whether the cochlea and labyrinth are spared or destroyed, and hence the audiological outcome.
The facial nerve within the temporal bone traverses three segments: the labyrinthine segment (from the fundus of the IAC to the geniculate ganglion), the tympanic segment (horizontal, crossing the medial wall of the middle ear), and the mastoid segment (vertical, descending to the stylomastoid foramen). Longitudinal fractures most commonly injure the tympanic (horizontal) segment or the geniculate ganglion, causing delayed or incomplete palsy. Transverse fractures often transect the labyrinthine segment, causing immediate, severe, usually permanent palsy.
The nasal skeleton is the most prominent and most commonly fractured facial bone. The paired nasal bones articulate superiorly with the frontal bone at the nasofrontal suture and laterally with the frontal processes of the maxillae. The intranasal septum consists of the quadrilateral cartilage anteriorly (extending from the columella to the dorsum) and bony components (vomer, perpendicular plate) posteriorly. The septal cartilage receives its blood supply entirely from the perichondrium; disruption of this supply leads to avascular necrosis.
The laryngeal framework — thyroid and cricoid cartilages, arytenoid cartilages — protects the airway but is itself vulnerable to fracture by direct anterior blows ('clothesline injuries'). The cricoid cartilage, as the only complete ring in the airway, is particularly significant: a fracture at the cricotracheal junction can cause complete airway separation.
Longitudinal and Transverse Temporal Bone Fractures
Pathophysiology of Key Head and Neck Injuries
Understanding the pathophysiology of each injury type allows the clinician to predict complications and time interventions correctly.
Haematoma auris (pinna haematoma) results from shear force between the perichondrium and the auricular cartilage, tearing the subperichondrial blood vessels. The haematoma is contained in the space between the two layers. Because the cartilage of the pinna has no intrinsic blood supply (relying entirely on the overlying perichondrium), the accumulation of blood separates the cartilage from its nutritional source. If the haematoma is not promptly evacuated, it organises over 7–10 days: fibroblasts from the perichondrium invade the clot, and new cartilage is deposited in a disorganised pattern, producing the irregular, firm, wrinkled cauliflower ear deformity. This is entirely preventable if the haematoma is aspirated or surgically drained and a pressure dressing applied within the first week.
Traumatic TM perforation results from a sudden increase in external auditory canal pressure (blast, slap) or a direct penetrating injury. Barotrauma — a rapid increase in pressure differential between the external canal and middle ear — is the mechanism in aircraft descent and underwater diving. The pars tensa is the most vulnerable portion. Most traumatic perforations are small and heal spontaneously; however, contamination at the time of injury (water entry), large perforations, or those with ossicular disruption require formal surgical repair (myringoplasty/tympanoplasty). A perforation that fails to heal can become the nidus for a secondary acquired cholesteatoma.
Temporal bone fractures are caused by high-energy trauma to the skull. Longitudinal fractures (70–80% of temporal bone fractures) follow a force applied to the temporoparietal region, driving the fracture line anterosuperiorly through the squamous bone, EAC, and middle ear anterior to the otic capsule. The otic capsule is usually spared, explaining the preservation of sensorineural function — the hearing loss is conductive (ossicular disruption, haemotympanum, TM rupture). Transverse fractures (approximately 20%) follow frontal or occipital forces, driving the fracture line across the petrous apex and through the otic capsule, destroying the cochlea and labyrinth — hence the complete sensorineural hearing loss and severe vertigo.
Septal haematoma follows trauma that shears the mucoperichondrium off the septal cartilage on one or both sides. Blood accumulates in the subperichondrial plane. The mechanism of necrosis is ischaemic: the perichondrium is separated from the cartilage surface, cutting off nutrient diffusion. Without intervention within 24–48 hours, the central cartilage begins to liquefy; subsequently the haematoma organises and is replaced by fibrous tissue and new disorganised cartilage, causing permanent septal thickening, deviation, and nasal dorsal collapse (saddle-nose deformity).
Laryngeal trauma mechanisms include direct blunt injury (the 'clothesline' mechanism — the outstretched neck meets a fixed object such as a dashboard or rope) and intubation-related injury (arytenoid dislocation, subglottic stenosis). The thyroid cartilage may fracture (vertical fractures are most common), and the hyoid bone may fracture at its greater cornua. The mucosal lining, if disrupted, allows air to track into the soft tissue — subcutaneous emphysema is the clinical sign.
SELF-CHECK
A 30-year-old rugby player is brought to casualty after a direct blow to his right ear. On examination, the right pinna shows a fluctuant, bluish, non-tender swelling over the anterior surface of the auricle. He presents 4 hours after the injury. The most appropriate immediate management is:
A. Reassure and review in 48 hours; most haematomas resolve spontaneously
B. Aspirate the haematoma under sterile conditions and apply a pressure dressing
C. Incise the haematoma, drain the blood, and apply a bolster (tie-through) dressing
D. Refer for urgent CT of the temporal bone to exclude fracture before intervention
Reveal Answer
Answer: B. Aspirate the haematoma under sterile conditions and apply a pressure dressing
Haematoma auris must be evacuated promptly to prevent cauliflower ear deformity. Early (within 7 days, ideally within 24-48 hours) aspiration of a fresh, non-organised haematoma is appropriate; a bolster dressing prevents re-accumulation. If the haematoma is recurrent after aspiration or already organised, incision and drainage with a through-and-through bolster suture is the definitive approach. CT temporal bone is not required for an isolated pinna haematoma without head injury. Watchful waiting invariably leads to cartilage necrosis and permanent deformity.