Page 2 of 20
EN4.30 | Head and Neck Trauma — SDL Guide (Part 2)
Examination and Investigation in Head and Neck Trauma
The ENT examination in trauma is conducted after the primary ATLS survey has been completed and life-threatening injuries have been addressed. The airway is the priority — if stridor, hoarseness, or subcutaneous emphysema is present, airway assessment and secure comes before ENT examination.
Provided image
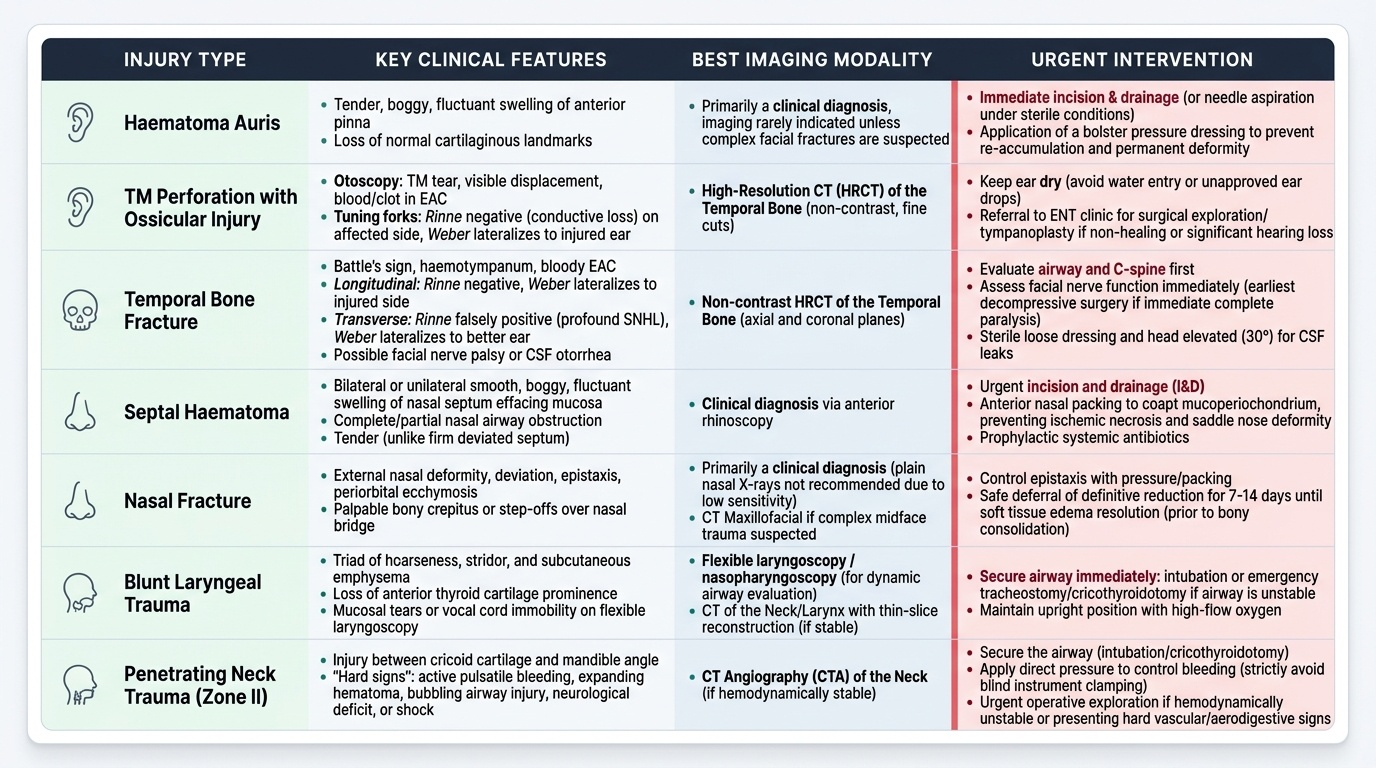
Systematic ENT examination after head and neck trauma:
Ear: Inspect the pinna for haematoma and lacerations. Examine the external auditory canal — blood in the EAC suggests TM rupture or temporal bone fracture; a step deformity in the canal wall suggests posterior wall fracture. Otoscopy: look for haemotympanum (blue or red behind the TM, indicating middle ear blood), TM perforation, or TM displacement. Check for Battle's sign (postauricular bruising, appearing 24–48 hours after fracture) and haemotympanum. Perform tuning fork tests: Rinne and Weber (see known-traps below for correct interpretation). In longitudinal temporal bone fracture, the Rinne is negative (bone conduction > air conduction = conductive hearing loss) and Weber lateralises to the injured ear; in transverse fracture, the Rinne is falsely positive but AC and BC are both reduced, and Weber lateralises to the better (uninjured) ear.
Nose: Inspect for deformity, ecchymosis, and epistaxis. With a nasal speculum, examine the nasal cavity: look for mucosal lacerations and, critically, for septal haematoma — a smooth, bilateral or unilateral boggy swelling of the septum that effaces the normal mucosal corrugations. Probe gently with a cotton swab — the haematoma is soft and fluctuant, unlike a deviated septum which is firm. Any clear watery nasal discharge in a head-injured patient must be tested for beta-2-transferrin (CSF marker) — the halo sign on a gauze pad (a clear ring around a blood spot) is a bedside indicator.
Larynx and neck: Examine the anterior neck for tenderness, swelling, step deformity of the laryngeal cartilages, and subcutaneous emphysema (palpable crepitus). Perform indirect laryngoscopy (or flexible nasopharyngoscopy) to assess the vocal cord mobility, arytenoid position, mucosal tears, and subglottic oedema if the airway is stable.
Investigations:
- Audiometry (pure tone audiogram) — to document and characterise hearing loss (conductive vs sensorineural) after temporal bone fracture; tuning fork tests give a bedside approximation.
- High-resolution CT temporal bone (axial 1 mm slices, bone window) — gold standard for temporal bone fracture classification, evaluation of ossicular chain disruption, and assessment of facial nerve canal integrity.
- CT face/paranasal sinuses — for nasal/frontal/maxillary fractures and evaluation of CSF rhinorrhoea; the coronal and axial cuts show the bony defect at the cribriform plate or frontal sinus posterior wall.
- CT angiography or Doppler ultrasound — for penetrating neck trauma to assess vascular injury (carotid, vertebral arteries).
- Beta-2-transferrin assay — from nasal fluid; gold standard for confirming CSF rhinorrhoea.
- Flexible nasopharyngoscopy / direct laryngoscopy — to assess laryngeal mucosal injury in blunt laryngeal trauma.
SELF-CHECK
A 28-year-old man is brought to the emergency department following a road traffic accident. He has blood from the right ear. Otoscopy shows an intact but blue-coloured tympanic membrane and no external auditory canal laceration. Tuning fork tests (512 Hz): Rinne negative on the right, Weber lateralises to the right ear. There is no facial nerve palsy and no sensorineural complaint. The most likely diagnosis is:
A. Transverse temporal bone fracture with labyrinthine disruption
B. Longitudinal temporal bone fracture with haemotympanum and conductive hearing loss
C. TM perforation from blast barotrauma
D. Sensorineural hearing loss from cochlear concussion
Reveal Answer
Answer: B. Longitudinal temporal bone fracture with haemotympanum and conductive hearing loss
The clinical picture — intact but blue TM (haemotympanum = blood in middle ear), Rinne negative (bone conduction > air conduction = conductive hearing loss), Weber lateralising to the affected (right) ear, and no sensorineural features — is classic for a longitudinal temporal bone fracture. Longitudinal fractures account for 70-80% of temporal bone fractures, pass anterior to the otic capsule (sparing the cochlea and labyrinth), and cause conductive hearing loss from haemotympanum/ossicular disruption. Transverse fractures disrupt the labyrinth, causing SNHL and severe vertigo with Weber lateralising to the unaffected ear. TM perforation from blast would show a visible TM defect on otoscopy.
Diagnosis and Differential Diagnosis
Accurate diagnosis in head and neck trauma requires integrating the mechanism of injury, the clinical signs elicited on examination, the audiological findings from tuning fork tests and audiometry, and the imaging results from high-resolution CT. Several distinctions are clinically critical because they directly determine urgency of intervention and long-term prognosis. The most important of these are: the distinction between longitudinal and transverse temporal bone fractures — which determines whether the cochlea is intact and whether facial nerve palsy will recover spontaneously or require surgical exploration; the distinction between septal haematoma and a simple deviated septum — which determines whether urgent drainage is needed within 24 to 48 hours; and the distinction between CSF rhinorrhoea and ordinary post-traumatic rhinitis — which determines whether the patient faces a meningitis risk requiring neurosurgical involvement. Each of these requires active clinical search — passive waiting for the diagnosis to declare itself is a common and costly error in the management of head and neck trauma.
Provided image
Temporal bone fractures: longitudinal vs transverse
The clinical differentiation of longitudinal from transverse temporal bone fractures is based on three domains — audiological findings, facial nerve palsy characteristics, and vestibular features:
| Feature | Longitudinal fracture | Transverse fracture |
|---|---|---|
| Frequency | 70–80% | ~20% |
| Direction | Parallel to petrous axis | Perpendicular to petrous axis |
| Otic capsule | Usually spared | Disrupted |
| Hearing loss | Conductive (haemotympanum, ossicular disruption) | Sensorineural (cochlear destruction) |
| TM | Lacerated/haemotympanum | Usually intact (haemotympanum possible) |
| Facial nerve palsy | ~20%; usually delayed (neuropraxia); good prognosis | ~50%; usually immediate and severe (transection); poor prognosis |
| Vestibular features | Mild/absent | Severe vertigo, nausea, positional nystagmus |
| Battle's sign | Present | Present |
| Imaging | CT shows fracture line anterior to labyrinth | CT shows fracture line through otic capsule |
Immediate facial nerve palsy after temporal bone fracture suggests nerve transection and mandates early surgical exploration. Delayed onset palsy (appearing hours to days after injury) suggests oedema and neuropraxia — conservative management with corticosteroids and monitoring is appropriate, as most recover spontaneously.
Septal haematoma vs deviated septum: Septal haematoma is smooth, fluctuant, bilateral (or may be asymmetric initially), and obstructs the nasal airway; a deviated septum is firm, cartilaginous, and present on one side only. Probe gently — haematoma yields, deviated septum does not. The history of recent trauma clinches the diagnosis.
CSF rhinorrhoea vs rhinitis: CSF rhinorrhoea is clear, watery, unilateral, increases on leaning forward (Ommaya's test or positional test), and does not cause nasal congestion. The beta-2-transferrin test is the gold standard diagnostic. Untreated, it risks ascending meningitis.
Blunt laryngeal trauma severity (Schaefer classification): Group I — minor haematoma/oedema, no fracture; Group II — oedema, mucosal disruption, minor fracture without exposed cartilage; Group III — massive oedema, exposed cartilage, fractures without/with anterior commissure injury; Group IV — above with unstable fractures; Group V — complete cricotracheal separation. Groups I–II: conservative management. Groups III–IV: tracheostomy + exploration and repair. Group V: emergency surgical airway + reconstruction.
Principles of Management
Management of head and neck trauma follows the ATLS hierarchy: airway, breathing, circulation, and neurological assessment take precedence over all ENT-specific interventions. The ENT surgeon must first collaborate in securing the airway and achieving haemostasis before proceeding to regional examination and ENT-specific procedures. This sequential approach is essential because errors in prioritisation — attempting nasal fracture reduction before the airway is secured, or delaying treatment of a septal haematoma while managing other injuries — can convert a manageable injury into a permanent disability or a life-threatening crisis. The sections below describe the management of each anatomical region in sequence, with the understanding that in a polytrauma patient, all life-threatening issues are addressed concurrently by the trauma team before any ENT intervention begins unless the ENT injury is itself immediately life-threatening (laryngeal obstruction, major neck vessel haemorrhage).
Ear injuries:
- Pinna haematoma: Aspirate under sterile conditions with an 18–20 gauge needle if fresh and uniloculated. Apply a firm pressure bandage or bolster suture (tie-through dressing using dental rolls on both sides of the pinna) to obliterate the dead space and prevent re-accumulation. Antibiotic cover to prevent secondary perichondritis (which would itself destroy cartilage). Surgical drainage is required for recurrent, multiloculated, or organised haematomas.
- Traumatic TM perforation: Most small-to-medium perforations (up to 50% of TM area) heal spontaneously within 4–8 weeks with dry ear precautions and topical antibiotic drops to prevent secondary infection. Keep the ear dry — water entry triggers infection and impedes healing. Surgical repair (myringoplasty) is indicated for perforations that fail to heal at 3 months, or for large perforations, or when there is associated ossicular disruption requiring tympanoplasty.
- Temporal bone fracture: Immediate management includes neurological stabilisation (co-managed with neurosurgery). Facial nerve palsy that is immediate and complete warrants high-resolution CT and consideration for surgical decompression; delayed/incomplete palsy is managed conservatively with systemic corticosteroids. Sensorineural hearing loss from cochlear disruption is treated with high-dose systemic corticosteroids (analogous to sudden SNHL protocol), though functional recovery is limited. CSF otorrhoea (beta-2-transferrin positive) is managed initially conservatively (head elevation, avoidance of Valsalva, 7–10 days); persistent CSF leak requires neurosurgical consultation for repair.
Nasal injuries:
- Septal haematoma: URGENT drainage within 24–48 hours. Under local anaesthesia, a horizontal incision is made on the mucosal surface of the haematoma, the blood is evacuated, and a through-and-through suture or nasal packing is placed to prevent re-accumulation. Antibiotic cover to prevent perichondritis (secondary infection of the evacuated space causes pyoderma/abscess with rapid cartilage destruction — a septal abscess is a surgical emergency).
- Nasal fractures: Closed reduction is performed ideally within 7–10 days of injury — after the acute swelling settles (usually at day 3–5) but before fibrous union occurs (after 10–14 days). Under local or general anaesthesia, the nasal bones are manipulated back to position using Walsham's forceps (for lateral displacement) or Asche's forceps (for depressed or septal fractures) and nasal packing/external splint applied. Missed fractures presenting after fibrous union require formal rhinoplasty/septorhinoplasty.
- CSF rhinorrhoea: Conservative management (head-up position, avoid nose-blowing, stool softeners to avoid Valsalva) for 7–10 days; 70–80% resolve spontaneously. Persistent CSF rhinorrhoea requires endoscopic skull base repair (neurosurgical collaboration).
Laryngeal trauma:
- Schaefer Group I–II: humidification, voice rest, observation; systemic corticosteroids to reduce oedema; intubation only if airway deteriorates.
- Schaefer Group III–V: secure the airway first — preferably via tracheostomy under local anaesthesia (to avoid the risk of complete airway loss during intubation in a shattered larynx). Rigid endoscopy/microlaryngoscopy to assess the mucosal damage, followed by open exploration and repair (reduction of fractures, mucosal repair, laryngeal stent placement in severe cases).
- Cricotracheal separation (Group V): the most dangerous laryngeal injury. If the patient arrives awake with a partially maintained airway, a tracheostomy tube may be passed through the injury site into the trachea under local anaesthesia — attempting oral intubation risks complete airway loss. Definitive reconstruction involves anastomosis of the trachea to the cricoid/subglottis.
Penetrating neck trauma:
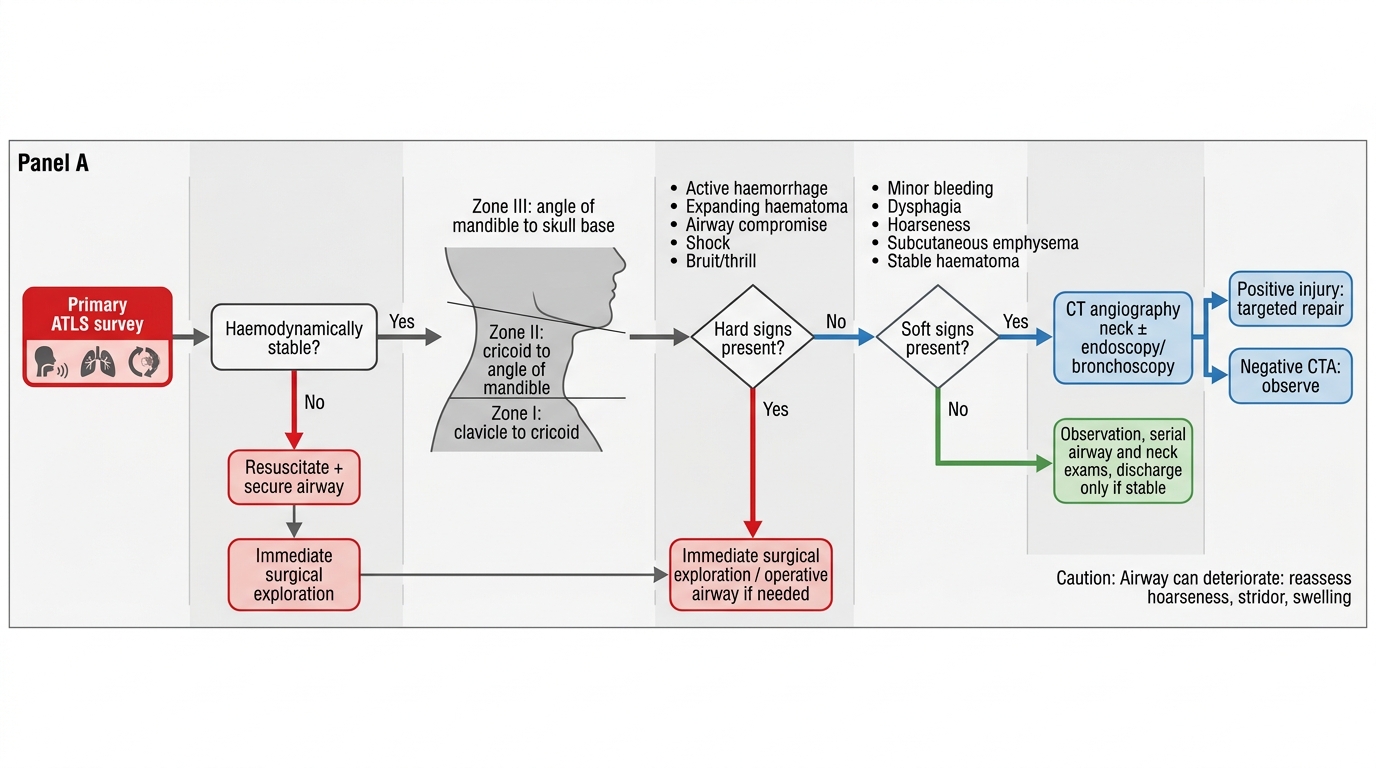
Management is governed by the zone of injury and the clinical signs:
- Hard signs (active haemorrhage, expanding or pulsatile haematoma, absent distal pulse, tracheal deviation, stridor, subcutaneous emphysema with crepitus, air bubbling from wound) → immediate surgical exploration regardless of zone.
- Zone II (cricoid to angle of mandible) with hard signs → direct surgical exploration. With soft signs (stable haematoma, minor haemoptysis, dysphagia without hard signs) → CT angiography of the neck to characterise vascular/aerodigestive injury before exploration.
- Zone I and Zone III → CT angiography preferred (surgical access is more difficult at these zones; endovascular management of vascular injuries is preferred when feasible).
Initial Management of Penetrating Neck Trauma
CLINICAL PEARL
The most preventable catastrophe in ENT trauma is a missed septal haematoma. Every patient presenting with nasal injury — however trivial-seeming — must have the nasal cavity examined with a speculum and the septum specifically inspected. A bilateral boggy soft swelling of the anterior septum that obscures the usual mucosal reflections is a septal haematoma until proved otherwise. The window for avascular necrosis prevention is 24–48 hours. A patient discharged with an undiagnosed septal haematoma will return weeks later with a permanent saddle-nose deformity — an iatrogenic preventable injury. Similarly, in laryngeal trauma, the patient who presents with 'only mild hoarseness' but develops stridor 4 hours later has progressive oedema compromising the airway: early reassessment and a low threshold for airway intervention are life-saving.
Self-Assessment
Before reviewing the summary, test your understanding with these focused questions. Each question below represents a common examination scenario or a clinical decision point that could appear in your ENT written papers or OSCE stations during the final year examinations. These questions are specifically designed to verify not just knowledge recall but clinical reasoning — you must be able to justify your answer with the correct anatomical and pathophysiological explanation, not simply select the correct option. Work through each scenario independently and construct your full answer before checking your reasoning against the summary section above. Pay particular attention to the tuning fork interpretation questions, the septal haematoma timing question, and the laryngeal trauma airway decision question — these represent high-stakes clinical judgements that distinguish adequate from excellent management of head and neck trauma.
- A 25-year-old presents 5 days after a fist fight with bilateral boggy soft swelling obliterating the normal nasal septal mucosa on both sides. He has moderate nasal obstruction and mild nasal pain. What is the diagnosis, and what immediate action is required?
- A 35-year-old woman has facial nerve palsy after a road traffic accident. CT temporal bone shows a longitudinal fracture anterior to the otic capsule. The palsy began immediately at the time of injury and is complete (House-Brackmann Grade VI). What does this presentation suggest about the nerve injury, and how does the immediate onset change management compared with a delayed-onset palsy?
- A 22-year-old motorcyclist has clear watery unilateral nasal discharge after a frontoparietal head injury. Describe the investigation of choice to confirm the diagnosis, and the two management steps you would take.
- List the hard signs in penetrating neck trauma that mandate immediate surgical exploration without further imaging.
- In blunt laryngeal trauma, why is elective oral intubation considered dangerous before airway assessment, and what is the preferred method of securing the airway in Schaefer Group III–IV injuries?