Page 4 of 20
EN4.35 | Salivary Gland Diseases — SDL Guide
Learning Objectives
- Describe the clinical features of common salivary gland diseases including sialadenitis, sialolithiasis, and neoplasms
- Identify appropriate investigations for salivary gland disorders including ultrasonography, CT, MRI, and fine-needle aspiration cytology
- Outline the principles of management of salivary gland diseases including medical and surgical approaches
- Recognise the distinguishing features of benign and malignant salivary gland tumours
- Apply knowledge of Sjögren's syndrome and systemic causes of salivary gland swelling
INSTRUCTIONS
Diseases of the salivary glands are common in ENT practice and range from acute infections threatening the airway to slow-growing tumours harbouring malignant potential. An understanding of salivary gland anatomy, the ductal system, and the spectrum of pathology — inflammatory, obstructive, neoplastic, and systemic — equips you to assess and triage these patients efficiently in a primary-care or specialist setting. Critically, recognising when a salivary swelling is a parotid tumour requiring FNAC and surgical referral versus a salivary calculus manageable with conservative measures is a core clinical skill at the MBBS level.
References
- Dhingra PL, Dhingra S — Diseases of Ear, Nose & Throat, 8th ed., Chapter 42: Salivary Gland Diseases (textbook)
- Hazarika P — Textbook of Ear, Nose & Throat, 4th ed., Chapter on Salivary Glands (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Chapter: Salivary Gland Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old schoolteacher presents with a painful swelling in front of his right ear that worsens every time he eats. He first noticed a dull ache in the right cheek three weeks ago, which intensified after meals. Today, the swelling is tense and tender, and he has low-grade fever. On examination, there is diffuse swelling over the right parotid region, the overlying skin is slightly erythematous, and pus can be seen dripping from Stensen's duct opposite the upper right second molar when the parotid is compressed. Meanwhile, in the adjacent waiting room, a 62-year-old woman has been waiting with a painless, slow-growing swelling in the same region for eight months. She is otherwise well and has no facial weakness. Two patients, same region, completely different pathologies — one acute bacterial parotitis, one likely parotid neoplasm. Your ability to differentiate them determines everything about their management.
WHY THIS MATTERS
Salivary gland disease is encountered in general practice, emergency medicine, and ENT outpatient clinics with considerable frequency. The parotid gland alone is responsible for a wide spectrum of problems — mumps parotitis in unvaccinated populations, suppurative sialadenitis in elderly debilitated patients, and the largest variety of benign and malignant tumours of any organ in the body. At the MBBS level, competency EN4.35 (KH domain) requires you to describe the clinical features, investigations, and management principles for this entire group. Beyond examination relevance, the consequences of mismanagement are serious: a missed parotid malignancy may involve the facial nerve; an untreated salivary calculus can lead to recurrent abscesses and eventual gland fibrosis; Sjögren's syndrome masquerading as bilateral parotid enlargement requires systemic immunological workup. The salivary glands also serve as a diagnostic window — HIV-associated lymphoepithelial cysts present as bilateral parotid swellings; parotid swelling can be the first sign of sarcoidosis or Sjögren's in a young woman.
RECALL
Bring to mind your anatomy of the head and neck. The parotid gland is the largest of the three paired major salivary glands, occupying the pre-auricular and infra-auricular region. The facial nerve (CN VII) emerges from the stylomastoid foramen, enters the parotid from its deep surface, and divides within the gland into two main divisions — the upper temporofacial and lower cervicofacial — which then branch into five terminal branches (temporal, zygomatic, buccal, marginal mandibular, and cervical). This anatomical relationship means that any surgery on the parotid risks the facial nerve if it is not carefully identified and preserved. Stensen's duct exits the anterosuperior surface of the parotid, traverses the masseter muscle, pierces the buccinator, and opens into the oral cavity opposite the crown of the upper second molar — the key landmark for both examining the duct opening and for cannulating it in sialography. The submandibular gland lies in the submandibular triangle, partly superficial and partly deep to the mylohyoid muscle, with its duct (Wharton's duct) passing forward to open at the sublingual papilla on the floor of the mouth, just lateral to the frenulum. The sublingual glands lie under the mucosa of the floor of the mouth and drain via multiple small ducts of Rivinus and sometimes a common duct of Bartholin into Wharton's duct.
Clinical Presentation of Salivary Gland Diseases
The clinical presentation of salivary gland disease is highly variable, and recognising the characteristic patterns of each category — inflammatory, obstructive, neoplastic, and systemic — allows the clinician to narrow the differential even before investigations are ordered. The three major salivary glands differ in their anatomical sites, secretory physiology, and disease predispositions, and this knowledge directly informs the clinical encounter.
The most important clinical presentation patterns are:
Acute painful swelling over one gland suggests an inflammatory or infective process. When it involves the parotid in an elderly, debilitated, or post-operative patient with a dry mouth, the diagnosis is almost certainly acute suppurative parotitis — bacterial infection ascending retrograde through Stensen's duct due to reduced salivary flow. The swelling is tense and tender, the overlying skin is erythematous and warm, there may be trismus (due to masseter irritation), and pus can be expressed from the duct opening on compression. Mumps parotitis differs critically in that it is bilateral, affects adolescents or young adults, and occurs in unimmunised populations — the swelling is less fluctuant, no pus is expressed, and the systemic symptoms (fever, malaise, orchitis) are prominent.
Episodic mealtime swelling — swelling of a salivary gland that appears or worsens during eating and subsides within 1–2 hours after the meal — is the hallmark presentation of salivary duct obstruction by a calculus. The mechanism is straightforward: eating stimulates salivary secretion; obstructed outflow raises intraductal pressure; the gland swells painfully against its tight capsule; when the secretory drive subsides post-meal, pressure drops and swelling resolves. This mealtime syndrome is most commonly felt over the submandibular region (because 80% of calculi occur in Wharton's duct) and is essentially pathognomonic of sialolithiasis.
Painless, slowly growing swelling in the parotid or submandibular region, present for months to years, is the typical presentation of a salivary gland neoplasm. Most parotid neoplasms (80%) are benign, and the commonest is pleomorphic adenoma — a firm, lobulated, non-tender, mobile swelling in the lower parotid that has been growing slowly for years and is entirely asymptomatic apart from the swelling. Any change in this picture — rapid growth, onset of pain, skin fixation, or facial weakness — immediately raises the suspicion of malignant transformation or primary malignancy.
Bilateral painless gland enlargement with dry mouth and dry eyes in a middle-aged woman is the classic presentation of Sjögren's syndrome — an autoimmune exocrinopathy that destroys glandular acini and causes the sicca complex.
Anatomy and Physiology of the Major Salivary Glands
The three major salivary glands — parotid, submandibular, and sublingual — together with hundreds of minor salivary glands distributed throughout the oral mucosa produce approximately 1–1.5 litres of saliva per day. Understanding their individual anatomical and secretory characteristics explains why specific pathologies preferentially affect specific glands.
The parotid gland is entirely serous in secretion, producing watery, enzyme-rich saliva high in amylase and proline-rich proteins. Its facial nerve relationship has been described above. The parotid is bounded anteriorly by the masseter and ramus of mandible, posteriorly by the mastoid process and sternomastoid, superiorly by the zygomatic arch and external auditory meatus, and inferiorly by the posterior belly of digastric. Because the parotid is enclosed in a relatively tight fascial capsule, acute inflammatory swelling within it produces significant pain and overlying skin erythema. Importantly, the parotid is the only salivary gland with intraglandular lymph nodes — there are 20–30 lymph nodes embedded within the gland — which is why parotid swelling can result from lymph node pathology (reactive, lymphoma, or salivary lymphoepithelial cysts in HIV).
The submandibular gland produces mixed serous-mucous secretion. Its ductal anatomy explains its susceptibility to calculi: Wharton's duct is long (approximately 5 cm), courses uphill against gravity from the gland to its anterior opening, and the submandibular gland secretes a more alkaline, calcium-rich, mucous-laden saliva that promotes crystal formation — explaining why 80% of salivary calculi are found in the submandibular ductal system. Wharton's duct makes two bends (at the posterior edge of mylohyoid and at the sublingual gland), providing ledges where calculi can lodge. The duct is also closely related to the lingual nerve (which hooks under it twice — first passing medially to it then looping below and lateral to it anteriorly) and the hypoglossal nerve inferiorly, creating surgical risk in gland excision.
The sublingual gland is the smallest major salivary gland, predominantly mucous in secretion. It is the least commonly affected by calculi or neoplasms.
Saliva has multiple functions beyond digestion: it maintains oral mucosal integrity, provides buffering capacity (bicarbonate), contains antimicrobial proteins (lysozyme, immunoglobulin A, lactoferrin), lubricates speech, and protects tooth enamel. Reduction of salivary flow (xerostomia) from any cause — Sjögren's syndrome, radiation, anticholinergic drugs, dehydration — leads to dental caries, mucositis, dysphagia, and increased infection risk.
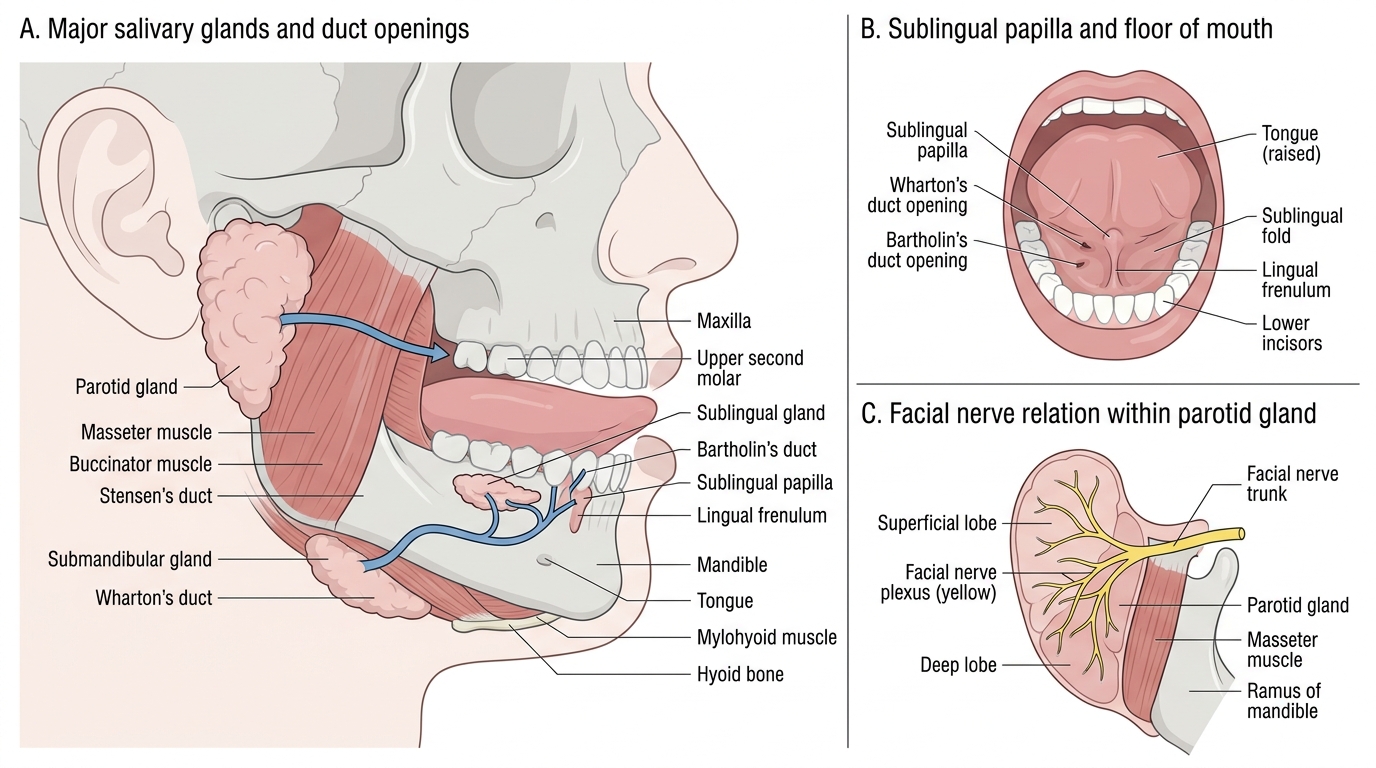
Major Salivary Glands, Duct Openings, and Facial Nerve Relation
Pathophysiology of Common Salivary Gland Conditions
Salivary gland diseases can be grouped into four broad pathophysiological categories: inflammatory/infective, obstructive, neoplastic, and systemic — and these categories often overlap (e.g., obstruction leading to secondary infection).
Inflammatory / infective causes begin with disruption of the normal antimicrobial properties of salivary flow. Reduced salivary flow — from dehydration, anticholinergics, or debility — allows retrograde bacterial colonisation of the duct from the oral cavity. The predominant organisms in acute suppurative sialadenitis are Staphylococcus aureus (most common, including MRSA in healthcare settings), viridans streptococci, and oral anaerobes. Acute bacterial parotitis is classically seen in elderly debilitated, dehydrated, or post-operative patients with poor oral hygiene. Mumps (paramyxovirus) produces bilateral parotitis in unimmunised children and young adults, associated with orchitis and meningitis. Chronic recurrent parotitis occurs in children (often resolving by puberty) and in adults with sialectasis — progressive duct dilatation and acinar atrophy.
Obstructive causes (sialolithiasis) arise from precipitation of calcium phosphate and calcium oxalate crystals in the ductal system, forming salivary calculi (sialoliths). The submandibular duct is the most common site (approximately 80% of all calculi) for the anatomical and physiological reasons described above. Calculi range from 1 mm to >10 mm and may be solitary or multiple. Obstruction raises intraductal pressure, causing glandular swelling, pain, and reduced secretion — the classic mealtime syndrome (swelling and pain provoked by eating, subsiding after 1–2 hours as salivary drive diminishes). Prolonged obstruction leads to secondary infection and eventually to gland fibrosis.
Neoplastic causes represent the most important diagnostic category to exclude: 80% of parotid tumours are benign (Dhingra's rule for the parotid), but submandibular and minor gland tumours have a higher malignant rate (approximately 50% and 80% respectively). Pleomorphic adenoma (benign mixed tumour) is the commonest salivary tumour overall — it has a bilobed capsule with microscopic pseudopod projections, explaining why enucleation alone (without adequate cuff of normal tissue) leads to recurrence. Warthin's tumour (papillary cystadenolymphoma) is a benign tumour exclusive to the parotid, bilateral in approximately 10% of cases, more common in men and smokers, and has a characteristic oncocytic epithelium with interspersed lymphoid stroma. Mucoepidermoid carcinoma is the commonest malignant salivary tumour overall; adenoid cystic carcinoma has a propensity for perineural invasion (skip lesions along nerve sheaths) and late haematogenous spread to lungs.
Systemic and autoimmune causes: Sjögren's syndrome is an autoimmune exocrinopathy — lymphocytic infiltration of salivary and lacrimal glands leading to xerostomia (dry mouth) and xerophthalmia (dry eyes — the sicca complex). Primary Sjögren's is the isolated form; secondary Sjögren's occurs in association with other connective tissue diseases (rheumatoid arthritis, SLE). Serological markers include anti-Ro(SSA) and anti-La(SSB) antibodies. Sarcoidosis, lymphoma, and HIV-associated lymphoepithelial cysts are other systemic causes of salivary gland enlargement.
SELF-CHECK
A 65-year-old man, three days post-abdominal surgery, develops painful swelling and erythema over the right parotid region with pus visible at Stensen's duct on compression. He is dehydrated and has had poor oral intake. The most likely diagnosis and causative organism are:
A. Mumps parotitis caused by paramyxovirus
B. Acute suppurative parotitis caused by Staphylococcus aureus
C. Pleomorphic adenoma with secondary infection
D. Sialadenosis secondary to alcoholic liver disease
Reveal Answer
Answer: B. Acute suppurative parotitis caused by Staphylococcus aureus
This is a classic presentation of acute suppurative (bacterial) parotitis in a post-operative, dehydrated patient. Reduced salivary flow from dehydration and poor oral intake allows retrograde bacterial contamination of Stensen's duct from the oral flora, with Staphylococcus aureus the commonest causative organism. The key signs are unilateral painful parotid swelling, overlying erythema, and expressible pus from the duct. Mumps would present bilaterally in a younger, unvaccinated patient without a post-surgical context. Pleomorphic adenoma is a slow-growing painless swelling. Sialadenosis is painless bilateral enlargement.