Page 6 of 20
EN4.35 | Salivary Gland Diseases — SDL Guide (Part 3)
Management of Salivary Gland Diseases
Management principles depend on the underlying pathology — inflammatory disease is primarily medical; obstructive disease is managed by relieving obstruction; neoplastic disease requires surgical removal.
Acute suppurative sialadenitis:
The first priority is increasing salivary flow to flush the gland: encourage oral hydration, oral hygiene, use sialagogues (lemon juice, citric acid lozenges). Systemic antibiotics covering S. aureus and oral streptococci are the cornerstone — flucloxacillin (or co-amoxiclav for broader oral flora coverage, including anaerobes) is the standard first-line regimen; MRSA should be suspected in healthcare-acquired infections. Warm compresses and regular gland massage help. If an abscess forms (fluctuant swelling, failure to respond to 48 hours of antibiotics), surgical incision and drainage is required. In the parotid, incision must be designed to avoid facial nerve branches — vertical incisions parallel to facial nerve branches, avoiding the classical "S"-shaped incision for superficial parotidectomy.
Salivary calculi (sialolithiasis):
Small, distal duct stones may pass spontaneously with increased hydration and massage. If the stone is palpable or visible at the duct orifice, duct incision (sialoductoplasty) under local anaesthesia allows direct removal without gland excision. For stones within the gland or those causing recurrent acute sialadenitis, submandibular gland excision is the definitive treatment. In selected cases, sialoendoscopy (salivary gland endoscopy) or extracorporeal shock-wave lithotripsy (ESWL) can fragment and retrieve stones endoscopically without open surgery. For parotid calculi, conservative management is usually preferred; parotidectomy for recurrent disease.
Salivary gland tumours — surgical principles:
The operative treatment of benign parotid tumours is superficial parotidectomy: the superficial lobe of the parotid containing the tumour is removed with the facial nerve carefully identified, dissected, and preserved. The key operative principle is to identify the main facial nerve trunk as it exits the stylomastoid foramen (using anatomical landmarks — tragal pointer, digastric muscle) before dissecting around the tumour. Malignant parotid tumours require total parotidectomy with assessment of the facial nerve: if the nerve is involved by tumour, sacrifice and post-operative radiotherapy may be necessary; if not involved, nerve preservation is attempted. Elective neck dissection is indicated for high-grade tumours or clinically positive nodes. Submandibular gland excision (submandibular gland excision through a submandibular approach) is the operation for submandibular gland disease — the key surgical risks are the marginal mandibular branch of the facial nerve (runs superficial to the gland) and the lingual and hypoglossal nerves.
Sjögren's syndrome: management is largely symptomatic — artificial saliva sprays, oral lubricants (pilocarpine, a muscarinic agonist, can stimulate residual secretion), and ophthalmological management for dry eyes. Systemic immunosuppression (hydroxychloroquine, corticosteroids) may be used for the underlying autoimmune component.
| Tumour Type | Behaviour | Treatment |
|---|---|---|
| Pleomorphic adenoma | Benign, recurrence if enucleated | Superficial parotidectomy with nerve preservation |
| Warthin's tumour | Benign | Conservative excision or observation |
| Mucoepidermoid carcinoma (low grade) | Low-grade malignant | Total parotidectomy ± neck dissection |
| Adenoid cystic carcinoma | Perineural invasion, late spread | Total parotidectomy + post-op radiotherapy |
| Carcinoma ex pleomorphic adenoma | Malignant, arises in pre-existing PA | Wide excision + radiotherapy |
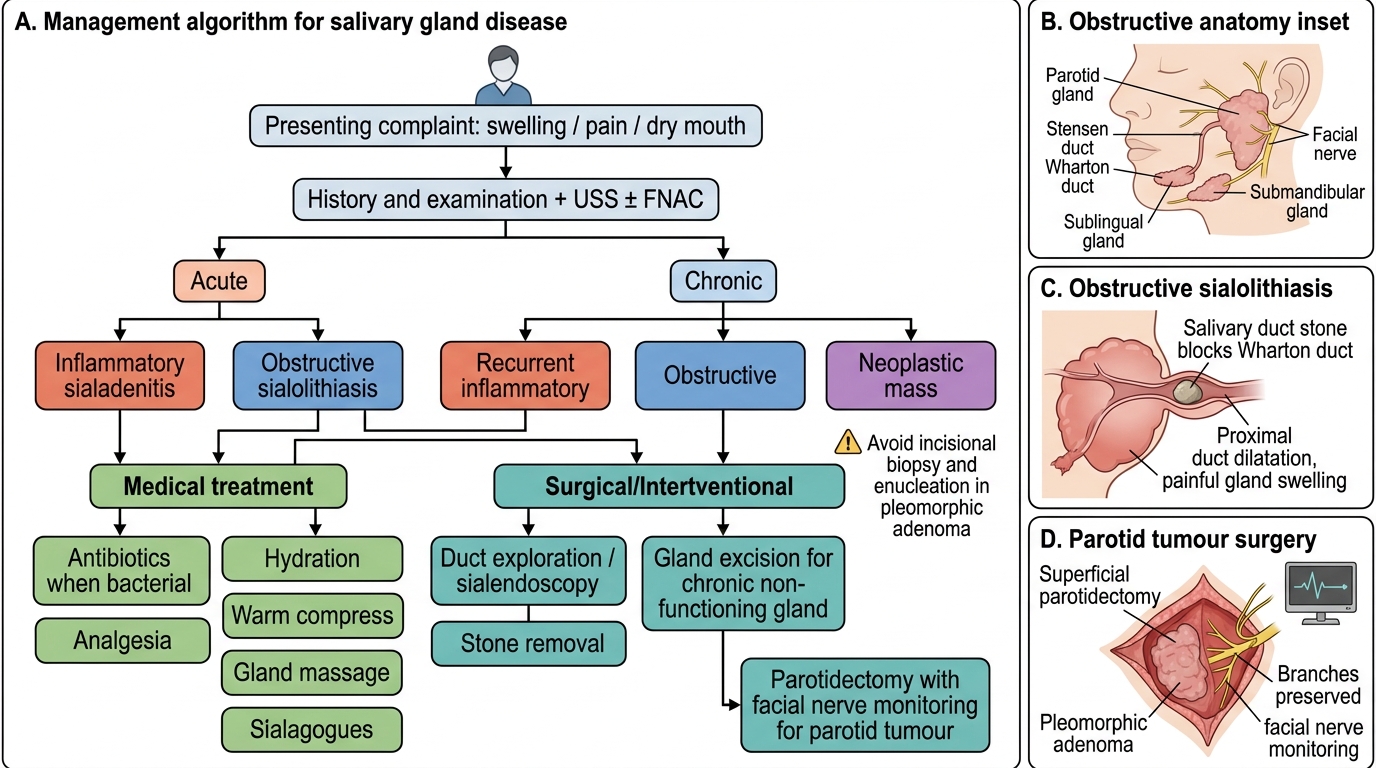
Management Algorithm for Salivary Gland Disease
SELF-CHECK
A 55-year-old woman is found to have a 3.5 cm firm, non-tender, lobulated swelling in the left parotid region of 5 years' duration. There is no facial palsy, no skin fixity, and no lymphadenopathy. USS confirms a solid intraparotid mass. FNAC is reported as 'features consistent with pleomorphic adenoma.' The correct management is:
A. Incisional biopsy to confirm the FNAC diagnosis before any intervention
B. Enucleation of the tumour through a small skin-crease incision
C. Superficial parotidectomy with identification and preservation of the facial nerve
D. Conservative observation with serial USS as she is asymptomatic
Reveal Answer
Answer: C. Superficial parotidectomy with identification and preservation of the facial nerve
Pleomorphic adenoma should be treated by superficial parotidectomy — not enucleation and not incisional biopsy. Enucleation is specifically contraindicated because the tumour has pseudopod projections through a thin capsule; enucleation seeds the field and leads to multi-focal recurrence. Incisional biopsy is also contraindicated (risks seeding and facial nerve injury — FNAC is the appropriate pre-operative tissue diagnosis tool). Conservative observation is incorrect because pleomorphic adenomas, although benign, may undergo malignant transformation (carcinoma ex pleomorphic adenoma) and will continue to grow. The correct operation identifies the main facial nerve trunk at the stylomastoid foramen, preserves all branches, and removes the superficial parotid lobe containing the tumour with a cuff of normal tissue.
Self-Assessment: Key Principles in Salivary Gland Disease
Before reviewing the summary, take a moment to consolidate your learning by working through the following self-assessment questions without returning to the earlier sections. This retrieval practice is one of the most evidence-backed strategies for durable learning — the effort of recalling information under conditions of uncertainty strengthens long-term retention far more than re-reading. These questions are structured at the level of NMC competency EN4.35 (KH — knowledge and higher-order application) and mirror the style expected in final-year university written examinations, OSPE stations, and clinical viva assessments in ENT. Each question tests not just factual recall but also your ability to reason through a clinical scenario using the principles you have studied in this module. The deliberate inclusion of questions spanning all five topic areas — inflammatory disease, sialolithiasis, benign tumour management, and systemic causes — ensures breadth of self-testing before you move to the summary.
Consider each of the following clinical scenarios and decide on the most appropriate next step:
- A 70-year-old woman on furosemide and oxybutynin presents with acute painful right parotid swelling 4 days after a major hip replacement. What is the diagnosis, and what is the first-line management?
- A 30-year-old man notices his right submandibular region swells painfully every time he eats and subsides within an hour. Plain occlusal X-ray shows a radio-opaque shadow in the right submandibular duct. What is the likely location of the calculus and how would you manage it?
- A 50-year-old woman has a 4 cm non-tender firm left parotid swelling of 7 years. FNAC reports pleomorphic adenoma. She asks why she cannot just have it 'popped out' under local anaesthetic. How do you explain the need for formal parotidectomy?
- A 45-year-old woman presents with bilateral parotid swelling, dry mouth, and dry eyes. Her anti-Ro antibody is positive and lip biopsy shows focal lymphocytic sialadenitis with focus score 2. What is the diagnosis and how do you manage it?
Review your answers by cross-referencing the management and diagnosis sections. Ensure you can articulate the reasoning — not just the answer — for each scenario, as clinical vivas reward mechanistic thinking over pattern-matching.