Page 1 of 29
EN4.21 | Nasal Obstruction — SDL Guide
Learning Objectives
- Elicit a structured clinical history from a patient presenting with nasal obstruction, identifying the pattern, laterality, and associated symptoms
- Describe the anatomical and pathophysiological mechanisms underlying the major causes of nasal obstruction
- Demonstrate the examination technique for anterior rhinoscopy and interpret findings relevant to the common aetiologies
- Choose appropriate investigations — anterior rhinoscopy, nasal endoscopy, CT PNS, allergy testing — and justify the choice based on clinical context
- Describe the principles of management for structural, inflammatory, and neoplastic causes of nasal obstruction, distinguishing medical from surgical indications
- Identify red-flag features that require urgent specialist referral
INSTRUCTIONS
Nasal obstruction is among the most common ENT complaints presenting to both primary care and specialist outpatient departments in India. It ranges from a trivial self-limiting mucosal swelling to a sign of nasopharyngeal malignancy. The competency EN4.21 requires you to elicit a correct history, select appropriate investigations, and describe principles of management — this module builds the clinical reasoning scaffold that connects a patient's symptom to the correct aetiological diagnosis and the right management pathway.
References
- Dhingra PL, Dhingra S. Diseases of Ear, Nose and Throat & Head and Neck Surgery. 8th ed. Chapter on Nasal Obstruction and DNS (textbook)
- Hazarika P, Nayak DR, Balakrishnan R. Textbook of Ear, Nose and Throat — Head and Neck Surgery. Chapter on Nasal Obstruction (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery. 8th ed. Vol 2: Rhinology section (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old software engineer presents to your ENT OPD with a 3-year history of progressive difficulty breathing through the left nostril. He sleeps with his mouth open, snores loudly, and his wife reports brief pauses in his breathing at night. He has tried saline nasal sprays with no improvement. On anterior rhinoscopy, you see the nasal septum clearly deviated to the left, with the inferior turbinate on the right appearing hypertrophied to compensate. There are no polyps, no discharge, no bleeding. The right nasal airway looks clear. The left side is nearly completely occluded by the deviated septum. What do you do next? What tests will confirm your clinical impression, and at what point is a medical trial no longer appropriate?
WHY THIS MATTERS
Nasal obstruction is one of the three or four most common reasons patients attend an ENT clinic in India, and it is also a symptom encountered daily at primary health centres, general practice settings, and emergency departments. Its causes span from benign — allergic rhinitis, a simple DNS, adenoid hypertrophy in a child — to serious and occasionally life-threatening conditions such as nasopharyngeal angiofibroma in adolescent males or malignancy in older patients. The clinical cost of missing a red-flag cause of nasal obstruction is high. Equally, the burden of undertreated nasal obstruction is large: chronic mouth breathing in children impairs facial development, disrupts sleep, reduces academic performance, and predisposes to recurrent upper respiratory infections. As a final-year MBBS student at the SH (supervised/history-taking) level, EN4.21 requires you to take a complete and correct history, select the right investigation, and describe management principles — this is foundational clinical ENT that you will use in every posting and in general practice.
RECALL
Before proceeding, recall from your anatomy (AN) sessions the structure of the nasal cavity. The paired nasal passages are separated by the nasal septum, composed anteriorly of the quadrilateral cartilage and posteriorly of the perpendicular plate of the ethmoid and the vomer. Projecting from the lateral wall of each nasal cavity are three paired bony scrolls — the inferior turbinate (a separate bone, the largest), middle turbinate, and superior turbinate (both parts of the ethmoid). The space below each turbinate is called its corresponding meatus — the inferior meatus receives the nasolacrimal duct; the middle meatus contains the ostiomeatal complex (OMC), the drainage pathway for the maxillary, frontal, and anterior ethmoid sinuses. From physiology (PY), recall the nasal cycle: a physiological alternating congestion and decongestion of the two nasal passages every 2–6 hours, mediated by autonomic innervation of the submucosal vascular sinusoids of the inferior turbinate. This cycle means that partial nasal obstruction on one side is normal — it is only pathological when obstruction becomes persistent, bilateral, or severe enough to impair breathing.
Clinical Presentation of Nasal Obstruction
The clinical history of nasal obstruction must answer five essential questions: Which side is obstructed? Is it constant or intermittent? When did it start and how has it progressed? What are the associated symptoms? And are there any red-flag features? The answers to these questions together narrow the differential diagnosis considerably before any physical examination is performed.
Laterality is the first and most important question. Unilateral nasal obstruction is strongly suggestive of a structural or neoplastic cause — most commonly a deviated nasal septum (DNS), a unilateral polyp (antrochoanal polyp, i.e., Killian's polyp), a nasal foreign body (especially in children), or, critically, a vascular tumour such as juvenile nasopharyngeal angiofibroma (JNA) in a young male. Bilateral obstruction is more likely to reflect a mucosal cause — allergic rhinitis, vasomotor rhinitis, bilateral nasal polyps (ethmoidal polyps), or bilateral inferior turbinate hypertrophy.
Onset and progression matter enormously. Sudden unilateral obstruction in a child raises the suspicion of a nasal foreign body. Gradual onset over months to years suggests DNS or a slow-growing structural lesion. Episodic obstruction that varies with season, time of day, or environment points toward an allergic or vasomotor aetiology.
Associated symptoms provide crucial aetiological clues:
- Rhinorrhoea (runny nose): watery, profuse discharge suggests allergic rhinitis; thick purulent discharge suggests chronic rhinosinusitis.
- Sneezing: prominent sneezing (particularly paroxysmal) points to allergic rhinitis.
- Anosmia or hyposmia (loss of smell): this localises to pathology involving the olfactory cleft — most commonly nasal polyps blocking airflow to the olfactory epithelium.
- Post-nasal drip and throat clearing: common in sinusitis and vasomotor rhinitis.
- Snoring and mouth breathing: especially in children — raises concern for adenoid hypertrophy.
- Headache and facial pain/pressure: sinusitis or mucosal oedema blocking sinus drainage.
- Epistaxis (nosebleed) with nasal obstruction: this combination is a red flag — the most important cause to exclude urgently is juvenile nasopharyngeal angiofibroma (JNA) in an adolescent male. Recurrent unilateral epistaxis with progressive nasal obstruction in a teenage boy demands imaging, NOT biopsy (biopsy of JNA causes catastrophic haemorrhage).
- Facial swelling, trismus, or diplopia with nasal obstruction: these suggest a malignant process — nasopharyngeal carcinoma, maxillary sinus malignancy, or a locally aggressive benign tumour.
Age of the patient provides context: nasal foreign bodies and adenoid hypertrophy are most common in children aged 1–10; DNS and vasomotor rhinitis peak in early adulthood; JNA is essentially confined to adolescent males; malignancy is more common after age 40.
A systematic history inquiry should also cover prior nasal trauma (predisposes to DNS), family history of atopy (allergic rhinitis), occupational exposure to dusts or chemicals (occupational rhinitis), previous nasal surgery, and any drug history — notably prolonged use of topical nasal decongestants causes rhinitis medicamentosa (rebound mucosal congestion after the decongestant wears off).
Anatomy of the Nasal Airway and Mechanisms of Obstruction
Understanding how the nasal airway can become obstructed requires a precise mental model of normal anatomy and the functional regions that are most vulnerable to pathological narrowing. Nasal airway resistance accounts for approximately 50% of total airway resistance during quiet breathing — the nasal airway is far narrower than the trachea, and small reductions in cross-sectional area have disproportionately large effects on airflow (Poiseuille's law: resistance is inversely proportional to the fourth power of the radius).
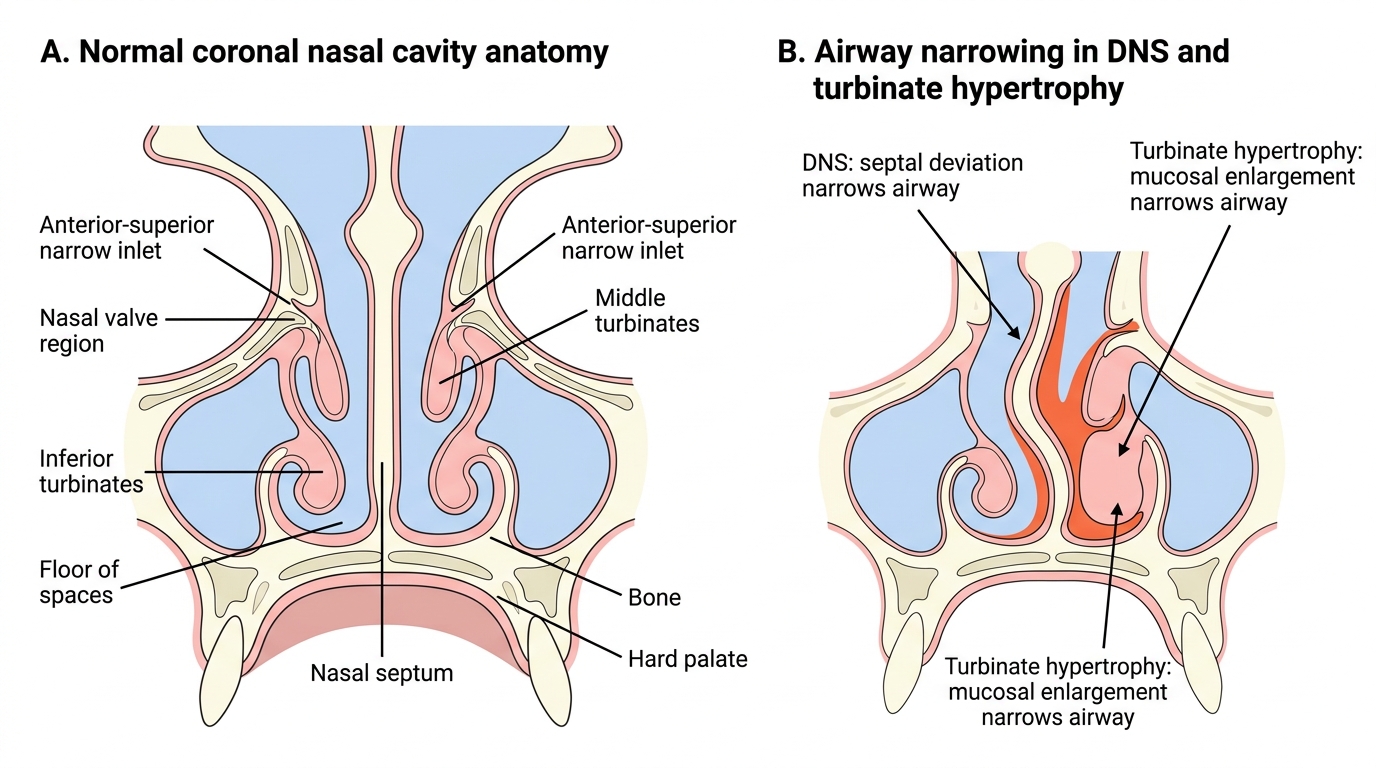
The narrowest region of the nasal airway is the nasal valve — the area bounded anteriorly by the alar cartilages and posteriorly by the anterior end of the inferior turbinate and the nasal septum. In adults, the minimum cross-sectional area here is approximately 0.5–0.7 cm². This is the critical flow-limiting zone: even minor swelling of the inferior turbinate mucosa at the nasal valve region can double airway resistance.
The inferior turbinate is the largest turbinate and the one most relevant to nasal obstruction. It is a separate bone covered by a thick erectile mucosa containing large venous sinusoids innervated by the autonomic nervous system. Sympathetic stimulation causes vasoconstriction and turbinate decongestion; parasympathetic stimulation causes vasodilatation and turbinate engorgement. This is the mechanism of the physiological nasal cycle and of the turbinate swelling seen in allergic rhinitis (parasympathetic predominance) and in rhinitis medicamentosa.
The nasal septum ideally lies in the midline. A deviated nasal septum shifts the midline, narrowing one nasal passage. The deviated side experiences chronic obstruction; the contralateral (open) side frequently develops compensatory hypertrophy of the inferior turbinate — the turbinate enlarges to fill the space left by the deviation, paradoxically reducing airflow on the nominally 'open' side. This bilateral functional obstruction from a unilateral structural lesion is important to explain to patients.
Mechanisms of obstruction can be grouped into three categories:
1. Structural narrowing — DNS, septal hematoma/abscess, synechia (adhesions), choanal atresia, stenotic nasal valve.
2. Mucosal swelling — allergic rhinitis, vasomotor rhinitis, rhinitis medicamentosa, acute viral rhinitis, sinusitis-associated mucosal oedema.
3. Mass occupying the nasal cavity or nasopharynx — nasal polyps (ethmoidal or antrochoanal), adenoids, foreign body, benign tumours (JNA, papilloma), malignant tumours.
Coronal Anatomy of Nasal Airway Narrowing
SELF-CHECK
A 14-year-old boy presents with a 6-month history of progressive right-sided nasal obstruction and three episodes of profuse right-sided nosebleeds requiring hospital admission. His mother reports no history of trauma. On anterior rhinoscopy, a firm, pinkish mass is seen in the right posterior nasal cavity. The most important next step is:
A. Biopsy the mass immediately under general anaesthesia to obtain a tissue diagnosis
B. Arrange urgent contrast-enhanced CT of the nose and nasopharynx — do NOT biopsy
C. Start the patient on high-dose intranasal corticosteroids for presumed nasal polyp
D. Perform nasal packing and arrange elective polypectomy
Reveal Answer
Answer: B. Arrange urgent contrast-enhanced CT of the nose and nasopharynx — do NOT biopsy
The clinical triad of adolescent male + progressive unilateral nasal obstruction + recurrent profuse epistaxis is the classic presentation of juvenile nasopharyngeal angiofibroma (JNA) — a highly vascular benign fibrovascular tumour. The single most important rule about JNA is DO NOT BIOPSY: the tumour's rich vascularity means biopsy in an outpatient or even inpatient setting can cause catastrophic, potentially fatal haemorrhage. Diagnosis is made on contrast-enhanced CT (showing an intensely enhancing mass in the nasopharynx, often with the pathognomonic 'antral sign' of anterior bowing of the posterior maxillary wall) and/or MRI. Angiography is performed pre-operatively to embolise feeding vessels. Intranasal corticosteroids are for polyps, not for JNA.
Examination and Investigations for Nasal Obstruction
The ENT examination of a patient with nasal obstruction follows a systematic sequence: external inspection, anterior rhinoscopy, posterior rhinoscopy (or nasal endoscopy), and relevant systemic examination. Each step yields information that the previous step cannot provide. A clinician who jumps straight to anterior rhinoscopy without first observing the patient from a distance will miss the adenoid facies of a mouth-breathing child, the saddle-nose deformity of prior nasal trauma, or the facial asymmetry of a unilateral maxillary mass. The sequence also mirrors how a consultant documents examination findings — mastering the format now saves time and errors in clinical practice.
External examination: Look for nasal pyramid deformity (trauma, DNS), skin changes, nasal tip asymmetry, flaring of the alae, and mouth breathing at rest. The adenoid facies in children — open mouth, elongated face, narrow maxillary arch, high-arched palate, and prognathism — develops as a consequence of chronic mouth breathing due to adenoid or turbinate obstruction.
Anterior rhinoscopy (using a Thudichum's nasal speculum and a headlight) is the primary bedside examination. It allows inspection of the anterior third to half of the nasal cavity:
- Nasal septum: position (midline/deviated/which side), surface (smooth/irregular), spurs (sharp bony projections at the septal floor that contact the inferior turbinate — a common cause of unilateral obstruction and headache).
- Inferior turbinate: size (normal/hypertrophied), colour (pale and boggy in allergy; red and swollen in infection; pale grey with polyps), surface.
- Nasal polyps: smooth, pale grey, translucent, insensitive (do not bleed or pain when probed — distinguishes them from the turbinate mucosa and from tumours), often described as 'grape-like'. Bilateral and multiple in ethmoidal polyposis; single and arising from the middle meatus or posterior nasal cavity in antrochoanal polyp.
- Discharge: character — watery, mucoid, mucopurulent.
- Foreign body: visible in the anterior nasal cavity in children — often unilateral purulent nasal discharge with foul odour is the clue.
Nasal endoscopy (rigid 0°/30°, or flexible nasopharyngoscope) provides a complete view of the nasal cavity and nasopharynx, including the posterior nasal space, adenoids, the ostiomeatal complex, and the nasopharyngeal opening of the Eustachian tube. It is the gold standard examination for evaluating chronic nasal obstruction and is essential when a mass is suspected.
Investigations:
- CT scan of PNS (paranasal sinuses): the investigation of choice for structural causes (DNS extent, turbinate anatomy, polyp extent, sinus involvement, bony erosion suggesting malignancy or aggressive lesion). Done in coronal sections for ENT planning.
- MRI nose and nasopharynx: superior soft-tissue detail; preferred for suspected JNA (intensely enhancing vascular mass) or malignancy.
- Allergy testing: skin prick test (SPT) or serum-specific IgE for aeroallergens — investigates the allergic aetiology in rhinitis.
- Rhinomanometry: objective measurement of nasal airway resistance — useful for pre-operative assessment and research; not always available.
- X-ray nasopharynx (lateral soft tissue neck): older investigation for adenoids — shows the adenoid shadow encroaching on the nasopharyngeal airway. Largely replaced by nasal endoscopy and CT.