Page 2 of 29
EN4.21 | Nasal Obstruction — SDL Guide (Part 2)
Differential Diagnosis and Aetiology
Constructing a differential diagnosis for nasal obstruction is most efficiently done by combining the laterality, age, onset pattern, and associated features from the history with the examination findings. A structured framework prevents common errors such as missing malignancy in an adult or JNA in an adolescent. The single most powerful organising principle is laterality: a bilateral presentation overwhelmingly points toward mucosal inflammatory disease, while a unilateral presentation demands systematic exclusion of structural, neoplastic, and foreign-body causes before settling on a mucosal diagnosis. Within the unilateral group, the age of the patient further stratifies risk: a child with unilateral foul discharge points to foreign body; a teenage male with recurrent epistaxis points to JNA; a middle-aged adult with facial symptoms points to malignancy.
Provided image
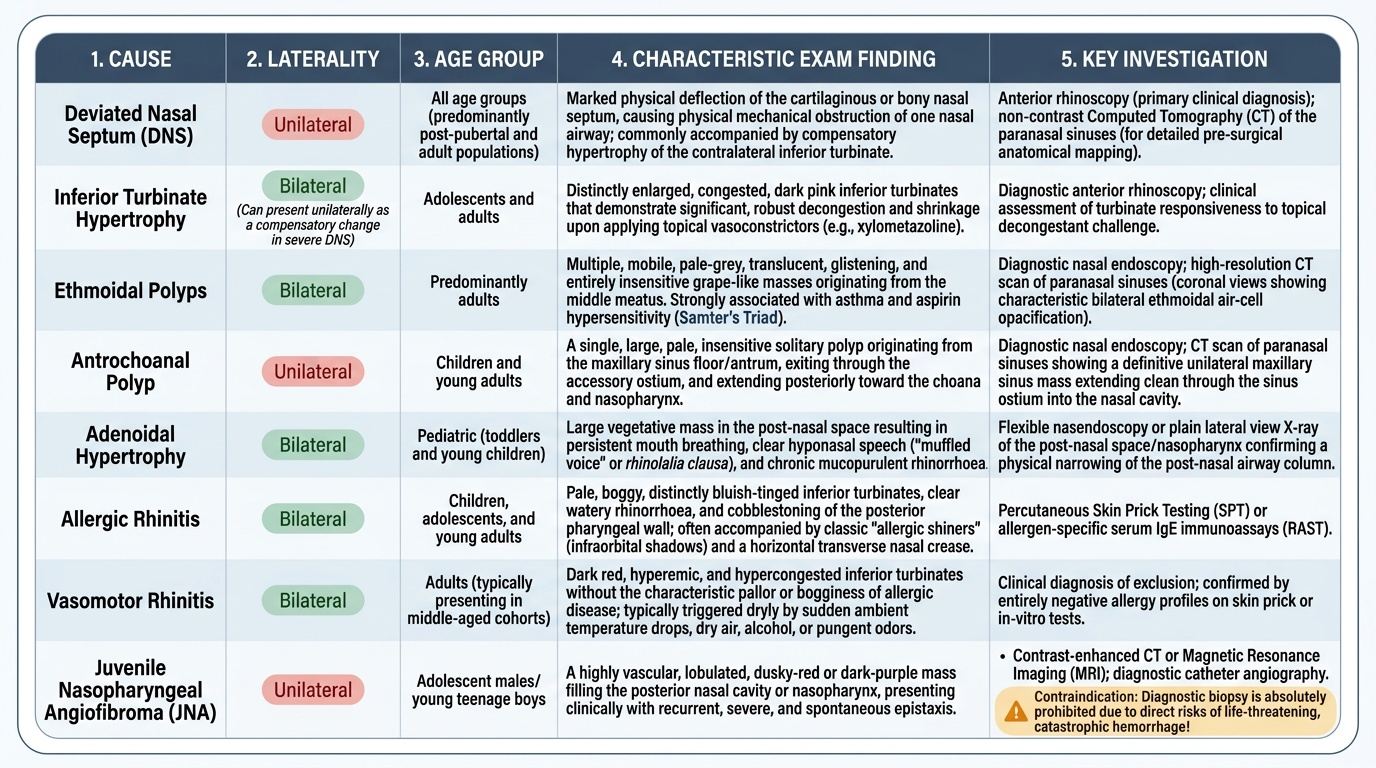
Bilateral nasal obstruction most commonly has an inflammatory mucosal cause in younger patients:
- Allergic rhinitis: commonest cause of bilateral nasal obstruction in young adults and children; associated with sneezing, watery rhinorrhoea, nasal itch, and eye symptoms; pale, boggy inferior turbinates on rhinoscopy; positive allergy test.
- Vasomotor rhinitis: non-allergic nasal hyperreactivity; perennial, triggered by temperature changes, strong smells, alcohol; no allergy on testing; inferior turbinate hypertrophy without pallor of allergy.
- Nasal polyposis (ethmoidal): bilateral, pale grey polyps arising from the middle meatus; associated with anosmia, hyposmia, and often with aspirin sensitivity and asthma (Samter's triad); adults predominantly; CT confirms extent.
- Bilateral inferior turbinate hypertrophy: often secondary to DNS compensatory hypertrophy or chronic mucosal inflammation.
Unilateral nasal obstruction demands a more vigilant approach, as structural and neoplastic causes are more likely:
- Deviated nasal septum (DNS): the commonest cause of unilateral (and often bilateral functional) nasal obstruction; structural, develops after nasal trauma or idiopathically; confirmed on anterior rhinoscopy and CT.
- Antrochoanal polyp (Killian's polyp): single, unilateral polyp arising from the maxillary antrum, passing through the accessory ostium into the nasal cavity and posteriorly through the choana into the nasopharynx; commoner in children and young adults. Key distinguisher: UNILATERAL, SINGLE — unlike ethmoidal polyps (bilateral, multiple).
- Nasal foreign body: in children aged 1–8; almost always unilateral; foul-smelling unilateral purulent discharge is the hallmark.
- Juvenile nasopharyngeal angiofibroma (JNA): ADOLESCENT MALE; progressive unilateral obstruction + recurrent epistaxis; highly vascular — DO NOT BIOPSY — diagnose on contrast CT/MRI + angiography.
- Malignancy: nasopharyngeal carcinoma, maxillary/ethmoid sinus malignancy — unilateral obstruction in middle-aged or older adults; associated features include facial swelling, diplopia, cervical lymphadenopathy, cranial nerve palsy. Any unilateral obstruction in an adult that does not respond to treatment must be investigated with nasal endoscopy and imaging.
SELF-CHECK
On anterior rhinoscopy of a 28-year-old woman with bilateral nasal obstruction, sneezing, and perennial watery rhinorrhoea, you see bilateral pale, boggy inferior turbinates with clear watery secretions. There are no polyps. Which is the most appropriate initial investigation?
A. CT scan of paranasal sinuses
B. Skin prick test for aeroallergens
C. Nasal endoscopy under general anaesthesia
D. X-ray of the nasal bones
Reveal Answer
Answer: B. Skin prick test for aeroallergens
The clinical picture — bilateral nasal obstruction, perennial sneezing, watery rhinorrhoea, pale boggy turbinates — is classic allergic rhinitis. The appropriate investigation is allergy testing: skin prick test (SPT) for common aeroallergens (house dust mite, cockroach, grass pollens, mould) or serum-specific IgE. CT PNS is for evaluating sinusitis, structural causes, or pre-surgical planning — it is not the first-line investigation for straightforward suspected allergic rhinitis. Nasal endoscopy under GA is invasive and not required at this stage. X-ray of the nasal bones is irrelevant to mucosal rhinitis.
Principles of Management
Management of nasal obstruction is directed at the specific aetiology. The two broad categories are medical management (appropriate for inflammatory and functional causes) and surgical management (required for structural, neoplastic, or medically refractory causes). The decision between the two depends on the underlying cause, severity of symptoms, and response to medical trial.
Medical management:
Intranasal corticosteroids (INCS) — e.g. mometasone furoate, fluticasone propionate, budesonide — are the most effective pharmacological treatment for nasal obstruction due to inflammatory causes (allergic rhinitis, vasomotor rhinitis, nasal polyposis). They reduce mucosal oedema, eosinophil infiltration, and vascular engorgement. Used as a first-line treatment for moderate-severe allergic rhinitis and as primary medical therapy for small nasal polyps. Require consistent use for 4–8 weeks before full efficacy is seen. Minimal systemic absorption at standard doses.
Antihistamines (oral — cetirizine, loratadine, fexofenadine; or intranasal — azelastine) — effective for sneezing, rhinorrhoea, and nasal itch in allergic rhinitis; have a lesser effect on nasal congestion compared with INCS.
Oral decongestants (pseudoephedrine, phenylephrine) — cause alpha-adrenergic-mediated vasoconstriction of turbinate sinusoids; provide short-term relief of congestion; not for long-term use (cardiovascular side effects, rebound).
Topical decongestants (oxymetazoline, xylometazoline) — highly effective for short-term relief (3–5 days maximum); prolonged use (>5–7 days) causes rhinitis medicamentosa (rebound congestion worse than the original), which itself is treated by tapering and switching to INCS.
Saline irrigation — isotonic or hypertonic nasal saline; mechanically clears mucus and crusts; improves mucociliary clearance; safe for long-term use as adjunct in any type of rhinitis.
Surgical management:
Septoplasty — the definitive surgical treatment for DNS causing significant nasal obstruction; performed under local or general anaesthesia; submucous resection of the deviated cartilage/bone with preservation of mucosal flaps. Septoplasty is performed after the age of 16–18, when nasal growth is complete, to avoid iatrogenic nasal growth disturbance in children.
Turbinate reduction surgery — for hypertrophied inferior turbinates refractory to medical therapy; options include submucous diathermy, radiofrequency ablation, partial inferior turbinectomy, or turbinoplasty.
Functional Endoscopic Sinus Surgery (FESS) — for nasal polyps with sinus extension, chronic rhinosinusitis refractory to medical therapy; removes polyps and opens the drainage pathways of the paranasal sinuses.
Adenoidectomy — for adenoid hypertrophy in children causing nasal obstruction, recurrent otitis media, or sleep-disordered breathing; typically performed between ages 3–10 before adenoids regress at puberty.
JNA management — pre-operative angiographic embolisation followed by surgical excision (endoscopic or open depending on extent). No medical treatment is curative. Surgery without prior embolisation carries very high blood loss risk.
Nasal foreign body — removal under direct vision with a hook or forceps, ideally under short general anaesthesia in an uncooperative child to prevent aspiration risk.
As a general principle, a medical trial of 4–8 weeks of INCS is appropriate before surgical referral for any inflammatory cause. For structural causes (DNS, JNA, malignancy), direct referral to ENT is appropriate. Any red-flag feature (unilateral obstruction with bleeding in a teenager, unilateral obstruction in an adult over 40 failing to respond to treatment, facial swelling, diplopia, cranial nerve involvement) should prompt urgent specialist evaluation.
CLINICAL PEARL
The single most dangerous error in the management of nasal obstruction is to biopsy a suspected vascular mass in the nasopharynx or posterior nasal cavity of an adolescent male without prior imaging. Juvenile nasopharyngeal angiofibroma (JNA) is an intensely vascular tumour — biopsy can precipitate catastrophic, life-threatening haemorrhage that may not be controllable even in an operating theatre. The rule is absolute: contrast-enhanced CT or MRI FIRST to characterise any posterior nasal or nasopharyngeal mass in a young male before any tissue sampling. The characteristic imaging appearance — an intensely enhancing vascular mass in the nasopharynx with or without the 'antral sign' (anterior bowing of the posterior maxillary sinus wall) — is diagnostic. Angiography and embolisation precede surgery.
Self-Assessment
Before moving to the self-check questions below, take a moment to mentally walk through the following scenario and structure your answer:
A 45-year-old male farmer presents with a 2-year history of progressive left-sided nasal obstruction and three episodes of blood-stained nasal discharge over the past 3 months. He has no history of trauma. He has mild left-sided facial swelling and has recently noticed diplopia (double vision). Anterior rhinoscopy shows a grey mass on the left lateral wall that appears firm and bleeds easily when probed.
Identify the red-flag features. What is the most urgent diagnostic step? What should NOT be done at this visit? What is the likely diagnosis you are most concerned about? How does this differ from the JNA scenario?
SELF-CHECK
A 7-year-old child is brought by parents for persistent left-sided nasal obstruction and a foul-smelling left-sided nasal discharge for 2 weeks. There is no history of fever or recent viral illness. On anterior rhinoscopy, the right nasal passage looks normal; the left shows purulent discharge but the nasal mucosa does not look particularly swollen or polypoidal. The most likely diagnosis is:
A. Left-sided antrochoanal polyp
B. Nasal foreign body
C. Acute left maxillary sinusitis
D. Unilateral allergic rhinitis
Reveal Answer
Answer: B. Nasal foreign body
In a young child with unilateral nasal obstruction and foul-smelling purulent discharge, a nasal foreign body is the diagnosis to consider first and foremost. Children aged 1–8 frequently insert small objects (beads, seeds, paper, food particles, rubber pieces) into the nostril, often without their parents' knowledge. The key clues are: unilateral, foul odour (the object decomposes or becomes infected), purulent discharge, and no fever/systemic illness. Antrochoanal polyp is also unilateral in children but would appear as a pale translucent mass on rhinoscopy and would not cause foul-smelling discharge. Acute maxillary sinusitis usually occurs bilaterally or with fever. Allergic rhinitis is bilateral.