Page 1 of 15
EN3.1 | Oto Microscopic Examination — SDL Guide
Learning Objectives
- State the clinical indications for oto-microscopic examination and explain why it supersedes naked-eye otoscopy for diagnostic and therapeutic ear procedures
- Describe the optical components of the binocular operating microscope and explain the principle of coaxial illumination and variable magnification
- Describe the step-by-step technique of oto-microscopic examination including patient positioning, speculum selection, focal adjustment, and systematic tympanic membrane survey
- Interpret common oto-microscopic findings including normal TM landmarks, central perforation (safe), attic/marginal perforation with cholesteatoma (unsafe), myringosclerosis, retraction pocket, and otitis media with effusion
- Explain the procedure of aural toilet under oto-microscopic vision and why it is preferred over blind syringing
INSTRUCTIONS
Oto-microscopic examination is the cornerstone of modern ENT clinical practice. The operating microscope provides magnification, coaxial illumination, and a stable working field that allows precise diagnosis and micro-surgical access to the ear — capabilities that a hand-held auriscope simply cannot match. The NMC EN3.1 competency requires you to observe and describe the indications and procedural steps of oto-microscopy. As a final-year student you will observe this procedure in the ENT outpatient department during your clinical posting; understanding its principles, technique, and interpretive findings will allow you to contribute meaningfully to the clinical encounter and to apply what you observe to patient management decisions.
References
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th ed., Ch. 1: Anatomy of Ear; Ch. 5: Chronic Suppurative Otitis Media (textbook)
- Hazarika P — Textbook of Ear, Nose and Throat, 3rd ed., Ch. 2: Clinical Methods of Examination of the Ear (textbook)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th ed., Vol. 2: Otology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old primary school teacher presents with a three-year history of persistent mucopurulent discharge from the left ear, mild conductive hearing loss, and occasional dull ache. You conduct a basic otoscopic examination in the outpatient cubicle, but wax and debris obscure your view of the tympanic membrane. The ENT surgeon takes over, seats the patient under the operating microscope, clears the canal under direct vision in less than two minutes, and then surveys the entire tympanic membrane with 16× magnification. In the attic region she identifies a white, pearly mass eroding the posterior canal wall. She turns to you and says: 'Cholesteatoma — this patient needs a mastoidectomy.' The auriscope gave you nothing; the microscope gave her the diagnosis. How does this instrument make that possible, and what would you look for if you were in her seat?
WHY THIS MATTERS
Oto-microscopic examination is not a procedure confined to tertiary-care operating theatres — it is performed daily in ENT outpatient departments across India and is the minimum standard of care for any patient presenting with chronic ear disease, suspected cholesteatoma, pre-operative assessment before middle-ear surgery, or any ear requiring aural toilet. As a final-year MBBS student you are expected, under EN3.1, to observe this procedure in your clinical posting and to describe its indications and steps. More broadly, understanding what the microscope can reveal prepares you to triage referrals from primary care: a patient who comes to a PHC with a chronically discharging ear and a pars flaccida retraction that you can describe accurately is correctly and promptly referred — one who is examined only with an auriscope may wait years before the atticoantral disease is recognised.
RECALL
Recall from your anatomy sessions that the tympanic membrane (TM) is divided into two distinct parts: the pars tensa, the taut lower four-fifths anchored by the fibrocartilaginous tympanic annulus, and the pars flaccida (Shrapnell's membrane), the flaccid upper one-fifth above the anterior and posterior malleolar folds, which lacks the fibrous intermediate layer. The handle (manubrium) of the malleus is embedded in the fibrous layer of the pars tensa, its lower end forming the umbo and its upper end the lateral process. The light reflex (cone of light) is seen in the antero-inferior quadrant — at approximately the 5 o'clock position on the right TM and 7 o'clock on the left TM — and is caused by reflection of the otoscope/torch light off the concave TM surface. Recall also from your PY sessions that the external auditory canal (EAC) follows an S-shaped course: the outer cartilaginous part runs upward-backward, and gentle traction on the pinna upward, backward, and outward in adults straightens this junction and aligns the canal for inspection.
Clinical Indications for Oto-microscopy
The hand-held auriscope is adequate for a screening examination of a healthy ear, but its limitations become critical in the setting of chronic or complex ear disease. The auriscope provides monocular vision, limited magnification (approximately 2–4×), a fixed light source that often casts shadows across the very structures one needs to see, and no working channel for instruments. Oto-microscopy overcomes each of these limitations by combining a binocular optical system, a coaxial light path, variable high magnification, and a stable fixed head that frees both the surgeon's hands for instrumentation. This combination is why oto-microscopy has become the gold standard for diagnostic and therapeutic ear examination in ENT practice — not just in teaching hospitals but in well-equipped district ENT outpatient departments across India. The procedure is particularly indispensable in the assessment of any patient with chronic or recurrent ear disease, where a definitive diagnosis determines whether the patient needs medical management alone or a surgical referral for mastoid exploration. Without oto-microscopy, the distinction between the benign tubotympanic type of CSOM and the dangerous atticoantral type with cholesteatoma is unreliable, and the consequences of missing cholesteatoma can include facial nerve palsy, meningitis, and death.
The principal clinical indications for oto-microscopy can be organised into three categories:
Diagnostic indications:
- Assessment of a chronically discharging ear where auriscopy cannot clearly visualise the TM through wax or debris
- Suspected cholesteatoma — the attic (pars flaccida) and the posterior marginal region of the TM must be inspected in detail at high magnification to exclude or confirm keratinising squamous epithelium
- Pre-operative assessment before any middle-ear or mastoid surgery, to map the extent of disease
- Detection of subtle TM perforations, retraction pockets, or myringosclerosis that are missed on routine auriscopy
- Assessment of TM mobility (combined with pneumatic otoscopy) in children with suspected otitis media with effusion
Therapeutic indications (procedure under microscopic vision):
- Aural toilet: removal of wax, discharge, crusts, granulation tissue, or polyps from the ear canal and middle ear under direct, magnified, bimanual vision
- Myringotomy and grommet insertion in children with persistent OME — the antero-inferior quadrant is selected precisely under microscopy
- Office procedures including removal of foreign bodies from the EAC, dressing application, and localised topical treatment of granulations
- Suction-clearance of a Eustachian tube-blocked ear
Surgical planning indications:
- Acoustic ear impressions and oto-acoustic emission testing in the clinic setting are complemented by microscopic TM survey
- Postoperative surveillance after tympanoplasty, ossiculoplasty, or canal-wall-down mastoidectomy — inspection of graft take, residual disease
Binocular Operating Microscope for Ear Examination
The Operating Microscope: Instrument and Optical Principles
Understanding the optical architecture of the operating microscope enables you to use it correctly, troubleshoot a blurred image, and communicate effectively with the surgeon when assisting in theatre. The operating microscope is not a single lens but an integrated optical system in which several components work together to produce a bright, shadow-free, stereoscopic image at variable magnification. Each component has a specific role, and a problem with any one of them — a dirty eyepiece, a misaligned focal length, a poorly set interpupillary distance — degrades the image in a characteristic way that you can diagnose and correct if you understand the optics. When you observe oto-microscopy during your clinical posting, you should be able to identify the objective lens, the magnification selector, the eyepieces, and the light source, and to describe their functions if asked by the supervising surgeon.
The binocular operating microscope used in ENT consists of four integrated optical components:
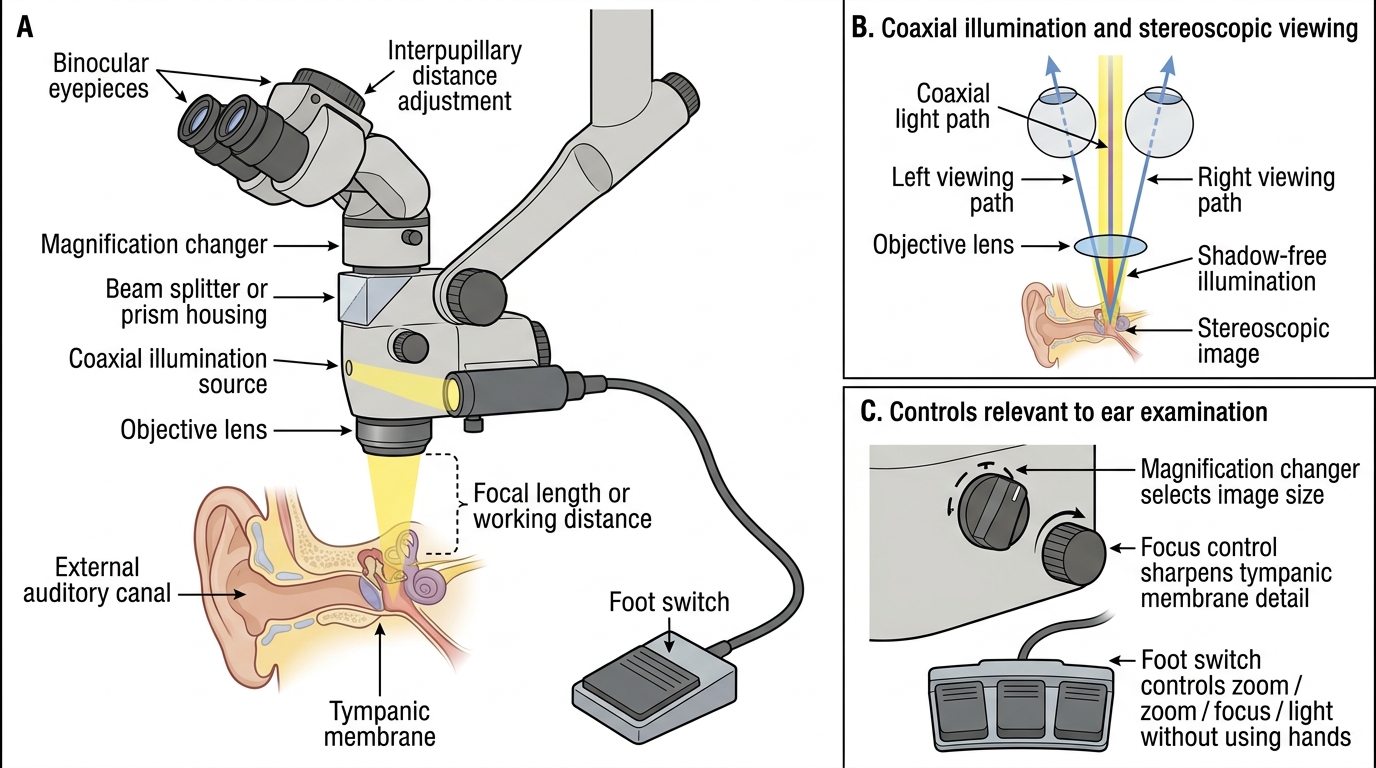
- Objective lens (working distance lens): The large bottom lens. Its focal length determines the working distance between the lens and the operative field. For otology the standard objective focal length is 250 mm (some surgeons use 200 mm or 300 mm depending on preferred working distance). The longer the focal length, the greater the working distance — useful for introducing instruments into the ear canal without fouling the lens.
- Magnification changer (zoom or step-change): A rotating drum or foot-switch-controlled zoom mechanism that switches between discrete magnification steps (commonly 6×, 10×, 16×, 25×, 40×). The surgeon starts at lower magnification to orient the field and increases magnification for detailed inspection. The image field decreases as magnification increases, so systematic survey at a lower step precedes high-power inspection of areas of interest.
- Binocular eyepieces (oculars): Two eyepiece tubes, typically 12.5× each, set at an interpupillary distance for the operator. The binocular configuration provides stereoscopic (three-dimensional) depth perception — critical for judging the depth of a retraction pocket or the distance to a dehiscent jugular bulb. This is the single greatest optical advantage over the monocular auriscope.
- Coaxial illumination system: A halogen or xenon light source whose beam is directed through the objective lens along the same optical axis as the observation path. Because the light and vision axes are coaxial, there are no shadows in the operative field — every surface, including the recesses of a mastoid cavity or the anterior recess of the TM, is evenly illuminated. The coaxial design also allows the surgeon's hands to work freely under the microscope without blocking the light.
The auriscope by comparison uses a speculum that partially occludes its own light source, provides monocular vision at fixed low magnification (~3×), and requires one hand to hold it — leaving only one hand for instruments.
A motorised foot switch or joystick allows the surgeon to move the microscope in X-Y-Z directions without breaking the sterile field during theatre work. In the outpatient clinic, manual adjustment of the microscope arm is standard.
Speculum Selection and Preparation
Speculum selection is the first practical decision in oto-microscopy and has a direct effect on the quality of the examination. The aural speculum is a funnel-shaped metallic or plastic tube that is inserted into the external auditory canal to keep its walls apart and hold the canal open during the examination. The speculum is the only instrument in contact with the patient, and an ill-fitting speculum causes pain, canal laceration, and an obstructed view.
Principle of speculum sizing: the correct speculum is the largest diameter that can be inserted comfortably into the bony-cartilaginous junction of the EAC without excessive force. Commonly available sizes for adults are 3, 4, and 5 mm in internal diameter (some sets include 2.5 mm for children or narrow canals). A speculum that is too small sits loosely in the canal, introduces a narrow viewing field, and requires more retraction pressure. A speculum that is too large causes pain, may lacerate the sensitive skin at the bony-cartilaginous junction, and can injure the posterior canal wall.
Material: Steel specula are reusable and autoclavable. Disposable single-use plastic specula are used in clinics following infection control protocols to prevent cross-transmission of ear organisms between patients.
Speculum insertion technique: The speculum is held between the thumb and index finger and directed along the long axis of the bony canal — neither directly inward nor superiorly but slightly downward and forward following the canal curvature. The pinna is simultaneously retracted upward, backward, and outward by the clinician's non-dominant hand (or by an assistant) to straighten the cartilaginous part of the EAC and align it with the bony part. Insertion is made in one smooth motion to the bony-cartilaginous junction; going further risks pressing the speculum rim against the sensitive bony canal wall, which is acutely painful.
Once the speculum is seated, the position is maintained either by the clinician's hand or, in theatre, by speculum-holding devices that free both hands for instrumentation.
SELF-CHECK
During oto-microscopy, which optical feature of the operating microscope enables the surgeon to see the anterior recess of the tympanic membrane without shadows, even when instruments are introduced into the canal?
A. High magnification (40×) objective lens
B. Coaxial illumination — light travels along the same axis as the observation path
C. Binocular eyepieces providing stereoscopic depth perception
D. Long focal-length objective lens of 300 mm
Reveal Answer
Answer: B. Coaxial illumination — light travels along the same axis as the observation path
Coaxial illumination means the light beam and the observation optical axis are aligned — light enters and exits along the same path, so there are no shadows anywhere in the field, including anterior recesses and deep canal walls. Binocular vision provides stereopsis (depth perception) but does not eliminate shadows. High magnification narrows the field without eliminating shadows. A long focal length increases working distance but does not affect shadow elimination.