Page 3 of 15
EN3.1 | Oto Microscopic Examination — SDL Guide (Part 3)
Interpretation of Oto-microscopic Findings
Accurate interpretation of oto-microscopic findings is the clinical endpoint of the examination. The ability to distinguish between normal variants, inflammatory changes, safe disease, and the dangerous atticoantral cholesteatoma pattern is the key knowledge tested by the EN3.1 competency.
Provided image
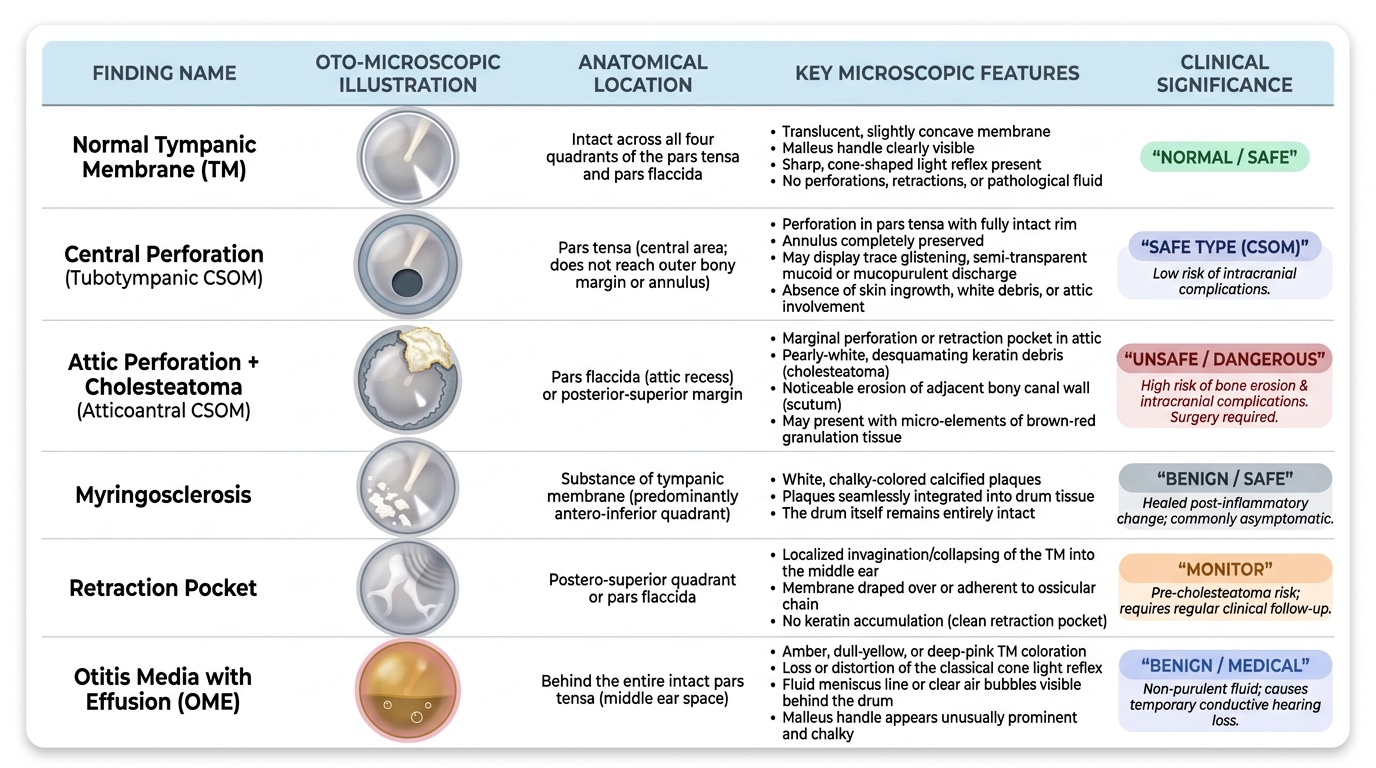
Normal tympanic membrane:
The TM is pearly-grey, translucent, and slightly concave. All four quadrants of the pars tensa are intact. The handle of malleus is visible as a white vertical stripe. The light reflex is present and cone-shaped. The pars flaccida above the lateral process is intact and not retracted. Transmitted movements of the ossicular chain may be seen as subtle TM flickering on phonation.
Abnormal findings and their significance:
Central perforation (tubotympanic CSOM — safe type):
A hole in the pars tensa with an intact rim of TM remaining all around the perforation. The annulus is preserved. Mucoid or mucopurulent discharge may be visible through the perforation. No skin ingrowth, no white debris, no attic involvement. This is the hallmark of tubotympanic disease — the 'safe' type of CSOM. 'Safe' here refers to the low risk of intracranial complications (not zero risk), reflecting the absence of cholesteatoma.
Attic perforation + cholesteatoma (atticoantral CSOM — unsafe type):
The pars flaccida (attic) shows a retraction pocket or a marginal perforation at the posterior-superior quadrant or in the attic. The key finding is cholesteatoma — white, pearly, desquamating keratin debris visible in the attic recess or extending into the posterior-superior quadrant. Bony erosion of the posterior canal wall (scutum) may be seen. Brown-red granulation tissue may mask underlying cholesteatoma. This is the 'unsafe' type, carrying a risk of bony erosion of the ossicles, facial nerve canal, lateral semicircular canal, tegmen, and sigmoid sinus — leading to potentially life-threatening intracranial complications. This type requires surgical management (mastoidectomy). Never call an atticoantral/cholesteatoma case 'safe.'
Myringosclerosis:
White chalky-coloured calcified plaques in the substance of the TM — most often in the antero-inferior quadrant. They represent healed inflammatory or post-grommet-insertion fibrous deposition. Myringosclerosis does not always cause conductive hearing loss — if the plaques do not immobilise the TM or ossicular chain, hearing may be near normal.
Retraction pocket:
A localised inward indrawing of a segment of the TM, most commonly in the posterior-superior quadrant or the pars flaccida. Retraction develops from negative middle ear pressure. Shallow retraction pockets may be managed conservatively; deep pockets reaching the incus or stapes, or becoming self-cleaning keratin reservoirs, progress to cholesteatoma and require surgery.
Dull amber TM (otitis media with effusion — 'glue ear'):
The TM is intact but dull, amber or grey-yellow, with loss of the light reflex and sometimes visible fluid level or air bubbles behind the TM. Tympanosclerosis and retraction change the TM colour and mobility. Pneumatic otoscopy confirms reduced TM mobility.
CLINICAL PEARL
The single most important decision in ear surgery is the distinction between 'safe' tubotympanic CSOM and 'unsafe' atticoantral CSOM with cholesteatoma — and this distinction is almost always made at the operating microscope, not with the auriscope. A central perforation in the pars tensa = tubotympanic = mucosal disease = can be observed or medically managed. Any finding in the pars flaccida (attic) or a posterior marginal perforation with white pearly debris = atticoantral = cholesteatoma must be excluded = surgical referral. This classification is not academic — missing a cholesteatoma allows it to erode bone silently for years until it presents as facial nerve palsy, labyrinthine fistula, or meningitis. The operating microscope, by providing magnification and shadow-free coaxial illumination, is what makes the pars flaccida inspection reliable enough to stake this clinical decision on.
Applied Practice: Case Scenarios
Working through these structured cases prepares you to interpret oto-microscopic findings during your clinical posting. For each case, formulate your interpretation and management decision before reading the discussion.
Case 1 — The teacher with a discharging ear (safe CSOM):
A 40-year-old female teacher presents with intermittent right ear discharge for 8 years, worse in the monsoon season. Audiometry shows a 30 dB conductive hearing loss at 500–2000 Hz. Oto-microscopy after aural toilet: a central perforation occupying the lower half of the pars tensa (antero-inferior and postero-inferior quadrants), mucopurulent discharge visible, pars flaccida intact, no bony erosion, no white debris.
Interpretation: Tubotympanic CSOM, right ear. Central perforation, mucoid disease, pars flaccida intact — consistent with safe mucosal type. No cholesteatoma features.
Management decision: Aural toilet, topical antibiotics (quinolone drops), medical management of any contributing rhinosinusitis, and when the ear is dry for 6 weeks, consideration for myringoplasty to close the perforation and restore hearing. No mastoidectomy required.
Case 2 — The man with attic disease (unsafe CSOM):
A 28-year-old man presents with foul-smelling right ear discharge, a sensation of fullness, and mild vertigo. Oto-microscopy reveals a deep retraction pocket in the pars flaccida with white pearly debris visible in the attic, granulation tissue at the posterior canal wall, and a scutum that appears eroded. The pars tensa has a small posterior-superior marginal perforation.
Interpretation: Atticoantral CSOM, unsafe type. Pars flaccida retraction with cholesteatoma confirmed by white keratinous debris and scutum erosion. Marginal perforation in the postero-superior quadrant. Vertigo suggests possible labyrinthine fistula from erosion of the lateral semicircular canal.
Management decision: CT temporal bone (non-contrast, high resolution) to map the extent of bony erosion. Urgent referral for tympanomastoid surgery (mastoidectomy). Do NOT manage conservatively — this is the 'unsafe' type with risk of life-threatening intracranial complications.
Case 3 — The child with hearing loss (otitis media with effusion):
A 7-year-old boy is brought by his parents with reduced hearing in both ears for 6 months. His school performance has declined. Oto-microscopy: both TMs are intact but dull, amber-coloured, with loss of the light reflex. The light reflex is absent bilaterally. A faint fluid level is visible in the left TM.
Interpretation: Bilateral otitis media with effusion (glue ear). Intact TMs, amber discolouration, absent light reflex, and visible fluid level on the left are classical signs. The chronicity and bilateral nature, combined with educational impact, meet the threshold for active management.
Management decision: Hearing assessment (pure tone audiometry or BERA in young children), tympanometry (type B flat curve confirms OME). If hearing loss >25 dB persisting >3 months with educational impact: myringotomy and grommet (ventilation tube) insertion under oto-microscopy. Address any underlying adenoid hypertrophy.
SELF-CHECK
A 12-year-old girl is seen with a painless right ear discharge and a white flaky mass visible in the attic region on oto-microscopy. The posterior canal wall appears eroded. The most important immediate management step is:
A. Prescribe oral amoxicillin-clavulanate for 2 weeks and review in 1 month
B. Arrange high-resolution CT of the temporal bone and urgent referral for mastoidectomy
C. Reassure as this is a normal variant (myringosclerosis) in a child
D. Perform myringoplasty in the outpatient department under local anaesthesia
Reveal Answer
Answer: B. Arrange high-resolution CT of the temporal bone and urgent referral for mastoidectomy
The clinical picture — white flaky mass in the attic (pars flaccida region), posterior canal wall erosion — is diagnostic of cholesteatoma with atticoantral CSOM (unsafe type). Bony erosion indicates the cholesteatoma is already expanding and destroying the ossicular chain or canal wall. The correct management is high-resolution CT temporal bone to map erosion and urgent surgical referral for mastoidectomy. Antibiotics address only infection, not the cholesteatoma itself. Myringosclerosis is a white patch in the pars tensa, not white debris with bony erosion. Myringoplasty repairs a perforation and is contraindicated in the presence of active cholesteatoma.
Self-Assessment
Before attending your ENT clinical posting, assess your ability to answer these questions without reference materials. They represent the minimum knowledge standard for the EN3.1 competency. This self-assessment is structured around the six arc steps of the EN-skills arc — indication, instrument, technique, interpretation, applied practice, and synthesis — so that your answers form a coherent clinical picture rather than isolated facts. A student who can describe the indications and procedure steps but cannot correctly classify a set of oto-microscopic findings has not yet met the competency; equally, a student who can classify findings but cannot describe why the operating microscope is used instead of the auriscope has gaps that will hamper their ability to communicate with ENT colleagues and triage patients correctly at the primary-care level. If you find any question difficult, re-read the corresponding section before your clinical posting rather than after.
- Name four clinical indications for oto-microscopic examination that go beyond what an auriscope can provide.
- Explain what coaxial illumination means and why it is important for inspecting the anterior recess of the tympanic membrane.
- What is the correct direction and technique for aural speculum insertion in an adult patient, and what pinna manoeuvre accompanies it?
- Describe the four quadrants of the tympanic membrane. In which quadrant is myringotomy performed, and why is that quadrant chosen?
- Distinguish tubotympanic CSOM from atticoantral CSOM: give the perforation location, presence or absence of cholesteatoma, and 'safe' vs 'unsafe' designation for each.
- A patient has a white pearly mass in the pars flaccida with scutum erosion. Name the diagnosis and state the surgical management.
If you cannot answer question 5 and 6 with confidence, re-read the interpretation section. The safe/unsafe classification of CSOM is the highest-stakes factual point in ear surgery and a frequent examination question.