Page 4 of 21
EN4.32 | Acute and Chronic Sinusitis with Complications — SDL Guide
Learning Objectives
- Elicit and document a structured history distinguishing acute rhinosinusitis from chronic rhinosinusitis, identifying features that indicate bacterial rather than viral aetiology
- Describe the clinical features of acute and chronic sinusitis and their orbital and intracranial complications
- Choose appropriate investigations including CT paranasal sinuses and interpret findings
- Describe the Chandler classification of orbital complications of sinusitis and the principles of management at each stage
- Describe the principles of medical and surgical management of acute and chronic rhinosinusitis
INSTRUCTIONS
Sinusitis is among the most common conditions encountered in ENT practice and general medicine, yet it is frequently mismanaged — antibiotics are over-prescribed for viral disease, and the serious orbital and intracranial complications of bacterial sinusitis are sometimes missed until irreversible damage has occurred. This module gives you the framework to distinguish viral from bacterial acute rhinosinusitis, recognise the alarming features of orbital and intracranial spread, manage acute disease appropriately, and understand the stepwise approach to chronic rhinosinusitis. The complications section is especially high-yield for finals examination and for clinical practice.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Ch 30-32 (textbook)
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd ed., Ch 22-23 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old engineering student presents to the casualty department at 11 PM with a 5-day history of a 'cold' that seemed to be getting better but suddenly worsened today. He now has severe right-sided facial pain, fever of 39.2°C, and right-sided periorbital swelling. On examination, the right eyelid is oedematous and erythematous, but he can open it and his visual acuity is 6/6 bilaterally. There is no proptosis and eye movements are full. What is the most likely diagnosis, and what is the single most important clinical question you must ask him right now to determine whether this is an emergency requiring surgical intervention tonight?
WHY THIS MATTERS
Rhinosinusitis — inflammation of the nasal mucosa and paranasal sinus mucosa — is one of the most prevalent conditions worldwide, affecting up to 15% of the population and accounting for approximately 20% of all antibiotic prescriptions in primary care. In India, where environmental pollution, perennial allergens, and crowded living conditions drive high rates of chronic nasal inflammation, rhinosinusitis is a major cause of outpatient ENT consultations. Despite its frequency, it is managed poorly at primary care level: viral ARS (which constitutes over 90% of cases) is routinely treated with antibiotics that provide no benefit and drive resistance. Chronic rhinosinusitis significantly impairs quality of life through nasal obstruction, anosmia, headache, sleep disruption, and fatigue — a burden comparable to chronic heart failure in patient-reported outcome measures. Most critically, the orbital and intracranial complications of untreated or inadequately treated bacterial sinusitis — orbital abscess, meningitis, brain abscess, cavernous sinus thrombosis — can cause blindness, permanent neurological deficit, or death, and they occur more often than they should because the warning signs are missed or acted upon too slowly.
RECALL
Recall from anatomy that the paranasal sinuses — frontal, maxillary (bilateral), ethmoidal (multiple air cells bilaterally), and sphenoidal — are pneumatic extensions of the nasal cavity lined by ciliated pseudostratified columnar epithelium (respiratory epithelium). They all communicate with the nasal cavity via narrow ostia. The frontal, maxillary, and anterior ethmoidal sinuses drain via the ostiomeatal complex (OMC) in the middle meatus; the posterior ethmoidal sinuses drain to the superior meatus; the sphenoidal sinus opens in the sphenoethmoidal recess above the superior turbinate. The key anatomical neighbour relationships to remember for complications are: the ethmoid sinus is separated from the orbit only by the paper-thin lamina papyracea; the frontal sinus posterior wall abuts the anterior cranial fossa dura; the sphenoidal sinus lies adjacent to the cavernous sinus, the optic nerves, the pituitary gland, and the internal carotid arteries. From your physiology revision, recall the mucociliary escalator: cilia beat in coordinated waves to propel the mucus blanket toward the ostia; any disruption of ciliary function (viral damage, desiccation, pollutants) or ostial obstruction causes mucus stagnation, creating a culture medium for bacterial secondary infection.
Clinical Presentation of Acute and Chronic Sinusitis
Rhinosinusitis is defined as inflammation of the nasal mucosa and the mucosa of one or more paranasal sinuses, and is classified by duration and clinical pattern. Understanding the symptom profile of acute versus chronic disease — and within acute disease, recognising the transition from viral to bacterial — is the foundation of appropriate management.
Acute rhinosinusitis (ARS) is defined as up to 4 weeks of symptoms. It almost always begins as a viral upper respiratory tract infection (rhinovirus, influenza virus, parainfluenza, adenovirus). The cardinal symptoms are: nasal blockage/congestion, nasal discharge (anterior or posterior), facial pain or pressure (most often over the affected sinus — cheek pain for maxillary, frontal headache for frontal, periorbital for ethmoid, vertex or occipital for sphenoidal), and hyposmia (reduced sense of smell). Fever may be present, particularly in children.
The clinical distinction between viral and bacterial ARS is crucial because it determines whether antibiotics are warranted. The 'double sickening' pattern is the classic indicator of bacterial secondary infection: the patient initially improves after 5–7 days of a viral URTI, then worsens with return of fever, purulent discharge, and facial pain. Alternatively, bacterial ARS is suggested by: persistent symptoms beyond 10 days without any improvement, severe symptoms from the outset (fever ≥38.5°C, purulent discharge, severe unilateral facial pain), or symptoms in an immunocompromised patient.
Key history points for ARS:
- Duration and pattern (worsening after initial improvement = 'double sickening');
- Severity of pain and fever;
- Dental history — maxillary sinusitis can originate from periapical infections of the upper molar/premolar teeth (the roots of the first and second upper molars lie immediately beneath the floor of the maxillary sinus); a history of recent dental pain, extraction, or root canal treatment is diagnostically important;
- Immunocompromise — diabetes, chemotherapy, HIV — which shifts the differential toward aggressive fungal sinusitis;
- Allergic history — allergic rhinitis predisposes to recurrent ARS.
Chronic rhinosinusitis (CRS) is defined as persistent symptoms of rhinosinusitis for more than 12 weeks, WITH objective evidence of mucosal disease on nasal endoscopy (polyps, purulence from middle meatus) or CT scan (mucosal thickening, sinus opacification). The symptom profile of CRS differs from ARS: facial pain is less prominent (or absent), while nasal obstruction, nasal discharge (anterior or posterior), hyposmia/anosmia, and a sense of facial fullness predominate. Headache in CRS is typically a dull pressure rather than the acute severe pain of ARS. The absence of fever and the chronicity of symptoms distinguish CRS from recurrent ARS. CRS is further subclassified into CRSwNP (with nasal polyps, eosinophilic phenotype) and CRSsNP (without polyps, more neutrophilic/bacterial phenotype) — covered in detail in the nasal polyps SDL.
Anatomy and Pathophysiology of Rhinosinusitis
The pathogenesis of rhinosinusitis follows a mechanistic sequence that begins with ostial obstruction, proceeds through mucociliary failure and mucus stagnation, and ends in bacterial or fungal colonisation and mucosal invasion. Understanding this sequence explains both why sinusitis occurs and why certain sinuses are more often affected.
The initiating event — ostial obstruction: The OMC is anatomically narrow and functionally vulnerable. Viral URTI causes mucosal oedema throughout the nasal lining, including at the delicate OMC; within hours, this oedema partially or completely obstructs the drainage pathways of the maxillary, frontal, and anterior ethmoid sinuses. The resulting negative pressure within the affected sinuses draws transudative fluid into the sinus lumen. Simultaneously, the viral infection directly damages ciliated epithelium — ciliary beat frequency falls, mucociliary transport slows, and the mucus blanket becomes stationary. The combination of a fluid-filled, poorly ventilated sinus and static mucus creates optimal conditions for bacterial overgrowth.
Bacterial secondary infection: The pathogens that colonise the nasopharynx and gain access to the obstructed sinus are predominantly Streptococcus pneumoniae (~30%), Haemophilus influenzae (~20%), and Moraxella catarrhalis (~10%) in ARS. These bacteria invade the stagnant mucus, proliferate, provoke a neutrophilic inflammatory response, and produce the mucopurulent exudate that defines bacterial ARS. In CRS, the microbial profile shifts toward Staphylococcus aureus (including MRSA in recurrent disease), Pseudomonas aeruginosa (especially in cystic fibrosis and post-surgical patients), and anaerobes (particularly in odontogenic maxillary sinusitis, where anaerobic bacteria from the oral flora predominate).
Odontogenic sinusitis deserves specific mention because it has a distinct clinical profile and different bacteriology. The roots of the first and second upper molar and second premolar teeth extend close to or through the floor of the maxillary sinus in a significant proportion of individuals. Periapical infection, dental extraction, or root canal treatment can introduce oral bacteria directly into the maxillary sinus, producing a unilateral maxillary sinusitis with a particularly foul-smelling purulent discharge. The diagnosis should be considered in any unilateral maxillary sinusitis, especially if there is an associated dental symptom or history of recent dental work.
Fungal sinusitis is increasingly important in immunocompromised patients. Allergic fungal rhinosinusitis (AFRS) is the commonest form in immunocompetent hosts — an IgE-mediated type 1 hypersensitivity to environmental moulds (Aspergillus, Bipolaris, Curvularia), producing thick eosinophilic mucin ('peanut-butter' appearance on CT) within expanded sinuses. In contrast, invasive fungal sinusitis (mucormycosis, invasive aspergillosis) is a rapidly progressive, life-threatening infection in patients with diabetic ketoacidosis, haematological malignancy, or organ transplantation; it invades blood vessel walls and causes ischaemic necrosis of the mucosa, bone, orbit, and brain.
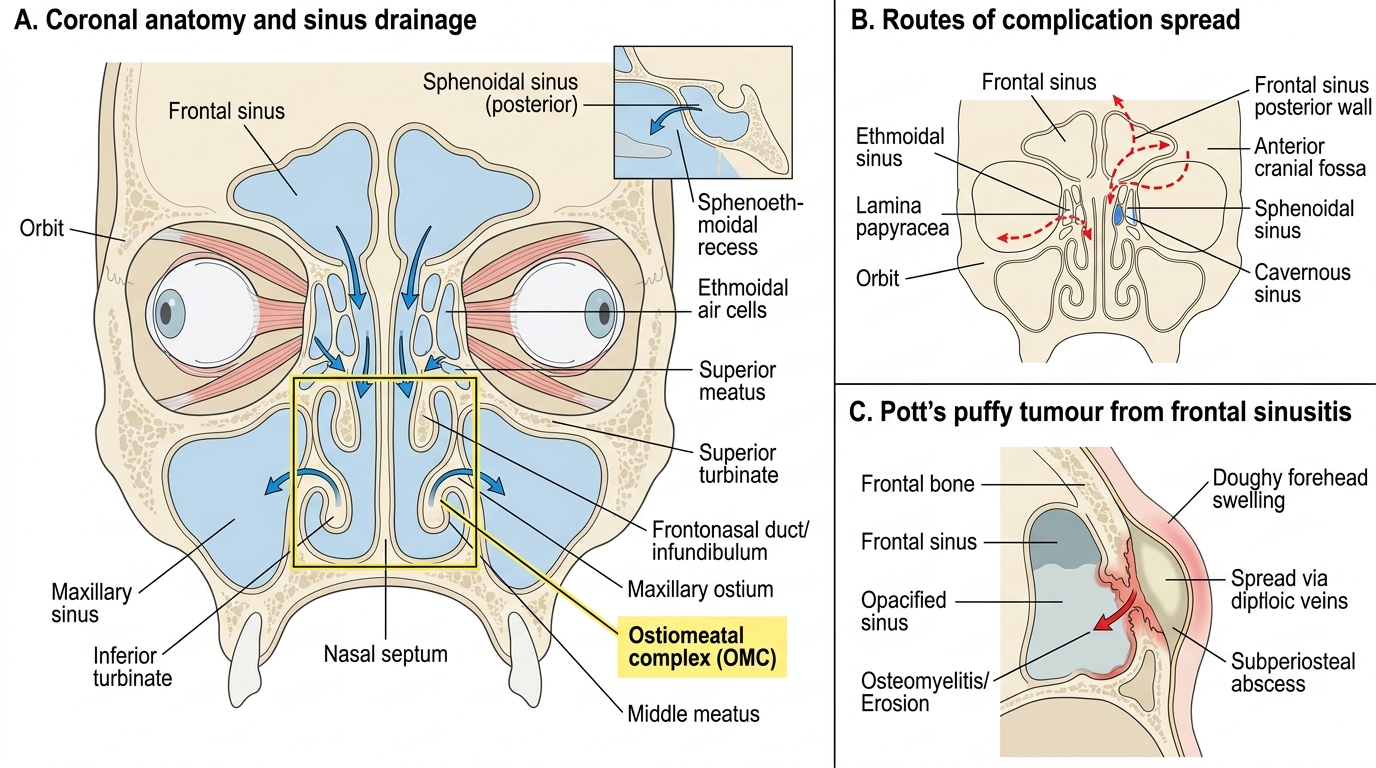
Sinonasal Drainage and Routes of Complication Spread
SELF-CHECK
A 16-year-old boy presents with a 3-week history of frontal headache and purulent nasal discharge following a 'bad cold' 4 weeks ago. Examination reveals a doughy swelling over the right forehead. He is febrile at 38.7°C. CT scan shows opacification of the right frontal sinus with erosion of the anterior table and a subperiosteal collection overlying the frontal bone. The most likely diagnosis is:
A. Orbital cellulitis secondary to frontal sinusitis
B. Pott's puffy tumour — osteomyelitis of the frontal bone with subperiosteal abscess
C. Cavernous sinus thrombosis presenting with forehead swelling
D. Frontal mucocoele expanding through the anterior orbital roof
Reveal Answer
Answer: B. Pott's puffy tumour — osteomyelitis of the frontal bone with subperiosteal abscess
Pott's puffy tumour is osteomyelitis of the frontal bone secondary to frontal sinusitis, with secondary subperiosteal abscess formation. The characteristic presentation is a doughy, tender, fluctuant swelling over the frontal bone (forehead) following frontal sinusitis — caused by spread of infection through diploic veins (venous system without valves) from the frontal sinus mucosa to the frontal bone and subperiosteal space. CT showing frontal sinus opacification with anterior table erosion and extracranial subperiosteal collection is diagnostic. It is named after Percivall Pott (of Pott's spine fame). Orbital cellulitis produces periorbital swelling, not forehead swelling. Cavernous sinus thrombosis causes proptosis, chemosis, and ophthalmoplegia. A mucocoele expands slowly and does not produce acute fever and doughy forehead swelling.
ENT Examination and Investigations
The clinical examination in rhinosinusitis serves two functions: confirming the diagnosis and screening for complications. A systematic approach ensures neither function is neglected. The examination begins with general assessment (temperature, look for periorbital swelling, facial asymmetry, forehead swelling) and then proceeds to nasal and oral cavity examination.
General and facial examination: Document temperature and heart rate (septic complications present with systemic toxicity). Inspect the periorbital region — preseptal (periorbital) cellulitis produces diffuse eyelid oedema without proptosis or ophthalmoplegia; these features, if present, indicate postseptal disease and require urgent imaging. Inspect the forehead for swelling (Pott's puffy tumour). Palpate the cheeks (maxillary tenderness), supraorbital ridge (frontal), and medial canthus (ethmoidal tenderness).
Anterior rhinoscopy: Examine for mucosal oedema, purulent discharge (especially from the middle meatus — the 'pus in the middle meatus' sign is highly specific for bacterial sinusitis of the anterior group of sinuses), nasal polyps (which may be the predisposing condition), and septal deviation (which may contribute to OMC obstruction).
Oral cavity: Examine the upper teeth for tenderness on percussion — a tender upper molar raises the possibility of odontogenic maxillary sinusitis.
Investigations:
1. CT paranasal sinuses (coronal and axial sections, without contrast for routine sinusitis; with contrast for suspected orbital or intracranial complications) is the investigation of choice for confirming sinusitis severity, identifying the affected sinuses, demonstrating OMC obstruction, and revealing complications. It provides the road map for surgical planning. Plain X-rays (Waters' view, Caldwell view) have largely been superseded because of their poor sensitivity and specificity — an air-fluid level on Waters' view has a sensitivity of ~75% for maxillary sinusitis, missing many cases and unable to assess the ethmoid and sphenoid sinuses adequately.
2. MRI paranasal sinuses: preferred over CT for suspected intracranial complications (superior soft-tissue contrast for brain abscess, epidural empyema, meningeal enhancement) and for distinguishing tumour from inflammatory disease (tumour signal differs from fluid). CT is faster and better for bone and orbital complications; MRI is complementary.
3. Endoscopy-guided middle meatal swab for culture and sensitivity: the gold standard for microbiological diagnosis when needed (refractory CRS, immunocompromised patients, suspected resistant pathogens). Simple nasal swabs are unreliable because they sample the anterior nares, which are colonised by skin flora that do not reflect the pathogens in the sinus.
4. Allergy testing (skin prick test, serum specific IgE): to identify allergic triggers in recurrent ARS or CRS with associated allergic rhinitis.
5. Laboratory investigations in suspected complications: full blood count (leucocytosis in bacterial sinusitis, particularly complications), CRP/ESR (elevated), blood cultures if systemic sepsis suspected. Lumbar puncture (if no raised ICP on CT) for suspected meningitis.