Page 5 of 21
EN4.32 | Acute and Chronic Sinusitis with Complications — SDL Guide (Part 2)
Diagnosis: ARS vs CRS and Differential Diagnosis
The diagnostic classification of rhinosinusitis follows a duration-and-phenotype framework that directly determines management. Applying it correctly requires clinical judgement, not just timeline counting. It is not sufficient to note that a patient has nasal discharge and facial pain — the clinician must determine whether the disease is acute or chronic, viral or bacterial, complicated or uncomplicated, because each of these determinations changes management fundamentally. Over-diagnosis of bacterial ARS leads to unnecessary antibiotic prescribing; under-recognition of CRS leads to years of inadequately managed disease; failure to classify CRS by phenotype (CRSwNP vs CRSsNP) means the wrong drugs are prescribed. The objective evidence requirement for CRS diagnosis — endoscopy or CT — exists specifically to exclude the large group of patients with facial headache and congestion who do not have sinonasal mucosal disease and therefore would not benefit from ENT-directed treatment.
Diagnostic criteria for ARS: Symptoms of rhinosinusitis (nasal obstruction, nasal discharge, facial pain/pressure, and/or hyposmia) lasting up to 4 weeks. Objective confirmation with CT or endoscopy is NOT required for uncomplicated ARS — the diagnosis is clinical. The EPOS 2020 guidelines use a visual analogue scale (VAS): mild ARS (VAS 0–3), moderate (VAS >3–7), severe (VAS >7–10).
Viral vs bacterial ARS — the critical distinction:
| Feature | Viral ARS | Bacterial ARS |
|---|---|---|
| Onset | Gradual with URTI | Double sickening or worsening after day 5–7 |
| Discharge | Clear or mucopurulent | Persistently purulent |
| Fever | Low-grade or absent | ≥38.5°C common |
| Unilateral pain | Uncommon | More typical |
| Duration | Usually resolves 7–10 days | Symptoms beyond 10 days without improvement |
| Antibiotic indicated | NO | Yes (amoxicillin/co-amoxiclav first-line) |
Diagnostic criteria for CRS: Symptoms persisting for >12 weeks PLUS objective evidence of mucosal inflammation on nasal endoscopy (mucopurulent discharge, mucosal oedema, or nasal polyps at the middle meatus) OR CT scan (mucosal thickening >5 mm, air-fluid level, or sinus opacification). The 12-week threshold distinguishes CRS from subacute rhinosinusitis (4–12 weeks). Objective documentation is mandatory for CRS — chronic symptoms without endoscopic or CT evidence of sinonasal disease should prompt reconsideration of the diagnosis (migraine, tension headache, or facial pain of dental or temporomandibular origin).
Differential diagnosis:
- Migraine/tension headache: no nasal discharge, no purulence on endoscopy, normal CT; headache often relieved by triptans; may be confused with 'sinusitis headache,' especially with periorbital location.
- Dental abscess: periapical infection mimics facial pain; dental X-ray demonstrates periapical lucency; the pain is tooth-localised with percussion tenderness.
- Nasal malignancy: unilateral symptoms, bloody discharge, bone erosion on CT, cranial nerve involvement — never diagnose sinusitis without considering malignancy in unilateral cases.
- Allergic rhinitis without sinusitis: no mucosal thickening on CT; sneezing, watery discharge, nasal itch; no facial pain.
- Wegener's granulomatosis / GPA: bloody crusting, septal perforation, saddle-nose deformity; consider in refractory CRS especially with systemic features (renal, pulmonary).
Complications of Sinusitis: Orbital and Intracranial
The complications of sinusitis represent the most dangerous aspect of this otherwise benign condition and demand prompt recognition and action. They arise from direct spread through bone (osteitis), haematogenous spread via the valveless diploic veins, or direct erosion of the sinus walls. Frontal and ethmoid sinusitis produce orbital and intracranial complications most frequently; maxillary sinusitis less often; sphenoidal sinusitis, though rare, is particularly dangerous because of the sinus's proximity to the cavernous sinus, optic nerves, and pituitary. The key anatomical substrate is the diploic venous system — the emissary veins within the bony tables of the skull lack valves, allowing bidirectional blood flow; infection can therefore spread from sinus mucosa to the adjacent bone, subperiosteal space, epidural space, subdural space, and ultimately to intracranial venous sinuses. Recognising that a patient with sinusitis is developing a complication requires vigilance for a small set of alarming clinical signs — periorbital swelling, proptosis, eye movement restriction, visual change, high fever out of proportion to nasal symptoms, and meningism — that must never be dismissed as part of routine sinus disease.
Provided image
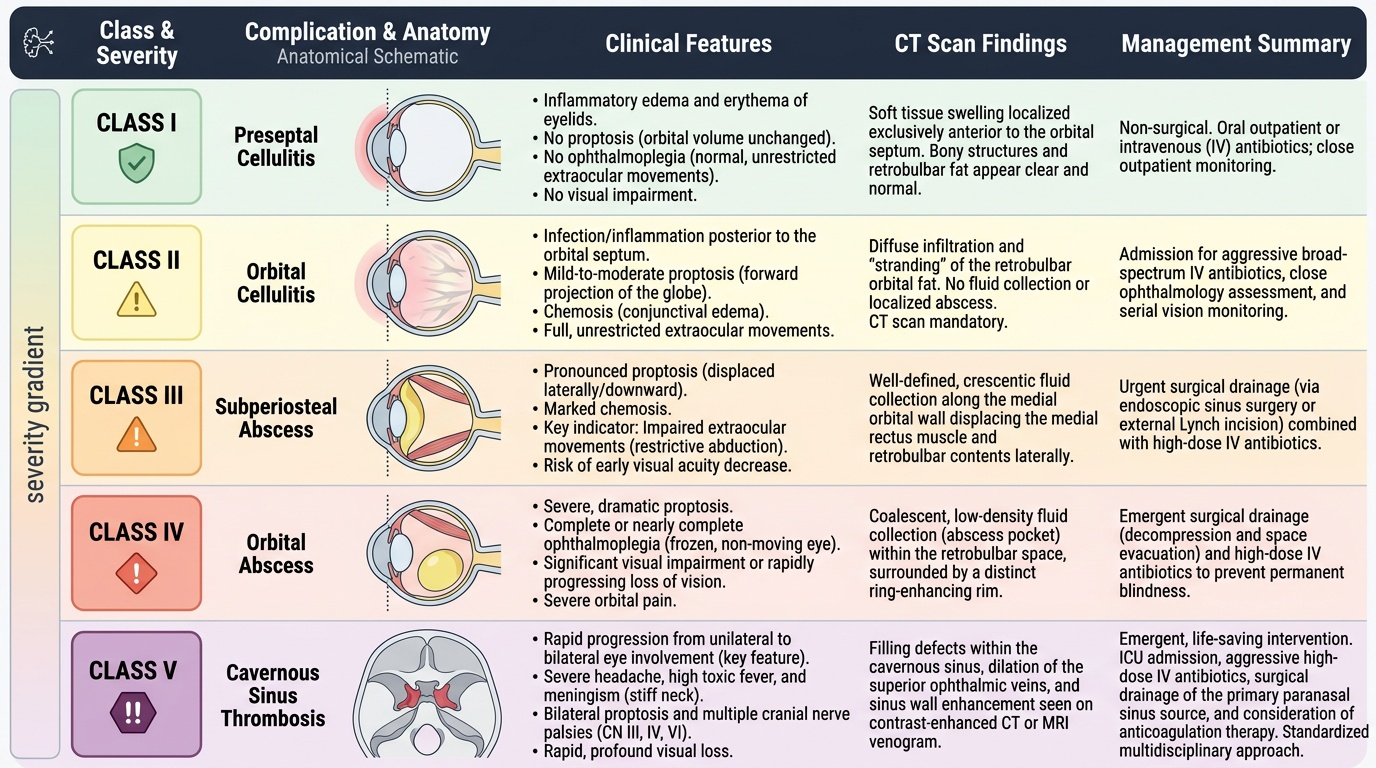
Orbital complications — Chandler classification:
Orbital complications are the commonest complication of acute sinusitis, most often from ethmoid sinusitis spreading through the lamina papyracea. The Chandler classification describes five progressively severe stages:
- Class I — Preseptal (periorbital) cellulitis: Inflammatory oedema of the eyelids anterior to the orbital septum. No proptosis, no ophthalmoplegia, no visual change. Treat with IV antibiotics; no surgical drainage required at this stage.
- Class II — Orbital cellulitis: Infection has spread posterior to the orbital septum into the orbital fat. Some proptosis and chemosis (conjunctival oedema) may be present but eye movements are full. IV antibiotics; CT scan mandatory to exclude abscess.
- Class III — Subperiosteal abscess: Collection of pus between the periorbita and the bony orbital wall (usually the medial wall, from ethmoid sinusitis). Proptosis, chemosis, impaired eye movements (particularly abduction on the affected side). CT shows medial subperiosteal collection. Requires urgent surgical drainage (endoscopic or external) unless the patient is improving rapidly on IV antibiotics under close monitoring.
- Class IV — Orbital abscess: Collection of pus within the orbital fat, displacing the globe. Severe proptosis, complete ophthalmoplegia, chemosis, eyelid oedema, severe pain. Reduced vision is a serious threat from optic nerve compression or ischaemia. Emergency surgical drainage required.
- Class V — Cavernous sinus thrombosis: Septic thrombosis of the cavernous sinus from direct spread or retrograde thrombophlebitis via the ophthalmic veins. Bilateral proptosis and ophthalmoplegia (involvement of CN III, IV, VI), high fever, prostration, meningism. High mortality. Treat with IV antibiotics (including anticoagulation if cavernous sinus thrombosis confirmed), neurosurgical review.
Key clinical rule: Any sinusitis patient with proptosis, restricted eye movements, or reduced visual acuity must be treated as a surgical emergency until Class III–IV is excluded by CT. The window between preseptal and orbital abscess can be hours in a rapidly progressing infection.
Intracranial complications:
Intracranial spread occurs predominantly from frontal sinusitis (through the posterior wall) and ethmoid sinusitis. Routes include direct erosion of bone, retrograde thrombophlebitis via diploic veins, and spread along the olfactory nerves. Intracranial complications include:
- Meningitis — fever, meningism (neck stiffness, Kernig's sign, photophobia), altered consciousness. CSF analysis after imaging (LP only if no raised ICP on CT).
- Epidural abscess — pus between the inner table of skull and dura. Often presents with persistent headache and fever; may be clinically subtle until large.
- Subdural empyema — pus in the subdural space; rapidly progressive, high mortality. Headache, fever, seizures, focal neurological deficits. Emergency neurosurgical drainage.
- Intracerebral abscess — frontal lobe abscess from frontal sinusitis; presents with frontal lobe syndrome (personality change, headache, seizures). CT with contrast or MRI demonstrates ring-enhancing lesion.
- Pott's puffy tumour — osteomyelitis of the frontal bone with subperiosteal abscess of the forehead; the swelling is characteristically doughy and pitting. Not directly intracranial, but often associated with intracranial involvement.
SELF-CHECK
A 30-year-old man with a 4-day history of severe frontal sinusitis develops right-sided proptosis, complete inability to move the right eye in any direction, and his visual acuity in the right eye is now counting fingers only. He also has bilateral eyelid swelling and is febrile at 40°C. The most urgent next step is:
A. Start oral amoxicillin and review in 48 hours
B. Urgent CT scan of the orbits and paranasal sinuses, and prepare for emergency surgical drainage
C. Perform lumbar puncture immediately to exclude bacterial meningitis
D. Start topical nasal decongestants and nasal saline irrigations
Reveal Answer
Answer: B. Urgent CT scan of the orbits and paranasal sinuses, and prepare for emergency surgical drainage
This presentation — bilateral proptosis, complete ophthalmoplegia (inability to move the eye in any direction), reduced visual acuity (counting fingers), and bilateral eyelid involvement — is strongly consistent with cavernous sinus thrombosis (Chandler Class V) or at minimum a severe orbital abscess (Class IV) with impending vision loss. This is a surgical and ophthalmological emergency. The immediate priority is urgent CT of the orbits and paranasal sinuses (with contrast) to define the extent of disease, followed by IV broad-spectrum antibiotics (including coverage for S. aureus and anaerobes — e.g. ceftriaxone + metronidazole + vancomycin), and urgent surgical drainage. LP would be dangerous before imaging excludes raised ICP. Oral antibiotics and topical treatments are wholly inadequate for this severity.
CLINICAL PEARL
In a patient with sinusitis and periorbital swelling, the single most important examination finding to assess is whether the proptosis is present and eye movements are full or restricted. Preseptal cellulitis (Class I) — eyelid swelling but no proptosis, full eye movements, normal vision — can be treated with IV antibiotics without surgical drainage. Any sign of proptosis, reduced eye movement, or visual change escalates immediately to Class III or IV territory and demands CT imaging and likely surgical drainage within hours. Do not be falsely reassured by the absence of fever in orbital abscess — the threshold for imaging should be low whenever the eye is involved.
Principles of Management of Sinusitis
Management of rhinosinusitis is stratified by severity, duration, and the presence of complications. The overarching principle — especially relevant for ARS — is that most disease is viral and self-limiting, and overprescribing antibiotics fuels antibiotic resistance without benefit to the majority of patients.
Management of ARS:
Mild-to-moderate viral ARS (duration <10 days, no severe symptoms, no fever ≥38.5°C): symptomatic treatment only — analgesics/antipyretics (paracetamol, ibuprofen), saline nasal irrigation (isotonic or hypertonic), and optionally topical nasal decongestants (oxymetazoline, xylometazoline) for short-term use only (maximum 5–7 days — risk of rhinitis medicamentosa with prolonged use). Topical intranasal corticosteroids reduce mucosal oedema and are recommended as an adjunct in patients with background allergic rhinitis. Antibiotics are NOT indicated.
Antibiotic therapy is indicated in ARS when: symptoms persist beyond 10 days without improvement, severe symptoms (fever ≥38.5°C, unilateral severe facial pain), 'double sickening' pattern, or immunocompromised host. First-line antibiotic: amoxicillin or co-amoxiclav (amoxicillin-clavulanate) for 5–7 days. Co-amoxiclav is preferred when there is high suspicion of beta-lactamase-producing H. influenzae or M. catarrhalis, or in dental sinusitis (anaerobic cover). For penicillin-allergic patients: azithromycin or a fluoroquinolone. Antral lavage (irrigation of the maxillary sinus via puncture of the inferior meatus under the inferior turbinate) is a diagnostic and therapeutic procedure for refractory maxillary sinusitis — it confirms bacterial infection by obtaining pus for culture and provides immediate symptom relief by draining the sinus.
Management of CRS:
CRS management follows the EPOS 2020 stepwise approach:
- Saline nasal irrigation + topical intranasal corticosteroids for 12 weeks — the evidence-based first-line for both CRSwNP and CRSsNP.
- Short-course systemic corticosteroids: for CRSwNP with grade 3 polyps or severe anosmia — short course prednisolone provides rapid shrinkage before topical steroids can take effect.
- Long-term macrolide antibiotics (azithromycin 250 mg three times weekly or clarithromycin 250 mg daily × 12 weeks): for CRSsNP without polyps — macrolides have anti-inflammatory (immunomodulatory) effects on neutrophilic sinusitis independent of their antibiotic action; evidence from studies in CRSsNP but NOT for CRSwNP.
- FESS (functional endoscopic sinus surgery): for CRS refractory to ≥12 weeks of adequate medical treatment. FESS opens the OMC, removes polyp tissue, and restores sinus ventilation and drainage. Post-operative topical corticosteroids are mandatory.
- Biologics (dupilumab): for severe uncontrolled CRSwNP after FESS failure or steroid dependence.
Management of complications:
- Chandler Class I (preseptal cellulitis): IV antibiotics (e.g. co-amoxiclav or ceftriaxone), admit for observation, daily vision and eye movement checks.
- Chandler Class II (orbital cellulitis): IV antibiotics, CT scan, monitor closely — proceed to drainage if no improvement within 24 hours or if any visual change.
- Chandler Class III–IV (subperiosteal/orbital abscess): urgent endoscopic or external surgical drainage in addition to IV antibiotics.
- Chandler Class V (cavernous sinus thrombosis): IV antibiotics (broad-spectrum including S. aureus cover), anticoagulation (evidence suggests heparin reduces mortality — specialist decision), ICU care.
- Intracranial complications (meningitis, empyema, abscess): joint neurosurgical and ENT management; neurosurgical drainage of empyema/abscess; FESS to drain the primary sinusitis; IV antibiotics guided by cultures.