Page 1 of 21
EN4.27 | Nasal Polyps — SDL Guide
Learning Objectives
- Elicit and document a structured history from a patient presenting with nasal obstruction and anosmia, identifying features that suggest nasal polyps
- Describe the clinical features of ethmoidal and antrochoanal polyps and distinguish between them
- Choose appropriate investigations including anterior rhinoscopy, nasal endoscopy, and CT of paranasal sinuses
- Describe the medical and surgical principles of management of nasal polyps
- Identify associated conditions including allergic rhinitis, asthma, and Samter's triad
INSTRUCTIONS
Nasal polyps are the commonest cause of bilateral nasal obstruction in adults and one of the most frequent presentations in an ENT outpatient clinic in India. Getting the diagnosis right requires distinguishing between bilateral ethmoidal polyps (the typical allergic-adult type) and the less common but clinically important unilateral antrochoanal polyp of children. Misidentifying a unilateral polyp as bilateral allergic disease delays the recognition of serious differential diagnoses including inverting papilloma and juvenile angiofibroma. This module equips you to take a systematic history, conduct a rhinoscopic examination, interpret a CT scan of the sinuses, and plan evidence-based medical and surgical management.
References
- Dhingra PL — Diseases of Ear, Nose & Throat, 7th ed., Ch 28-29 (textbook)
- Hazarika P — Textbook of ENT and Head & Neck Surgery, 3rd ed., Ch 20-21 (textbook)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th ed., Vol 2, Rhinology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 34-year-old schoolteacher presents with a 2-year history of worsening nasal blockage, complete loss of smell, and a constant drip down the back of her throat. She has had three courses of antibiotics from her GP over the past year with only temporary improvement. She also has longstanding 'allergic sneezing' in the mornings and uses an over-the-counter antihistamine sporadically. On anterior rhinoscopy you see pale, glistening, grape-like masses bilaterally filling both nasal cavities. She asks you, 'Can these be removed permanently?' What is the diagnosis, and what would you tell her about treatment — and recurrence?
WHY THIS MATTERS
Nasal polyps affect approximately 1–4% of the general population and are responsible for a substantial proportion of ENT outpatient attendances in India. They are the single commonest cause of bilateral nasal obstruction in adults, and chronic rhinosinusitis with nasal polyps (CRSwNP) is now recognised as a distinct phenotype with a strong eosinophilic-inflammatory basis. For the clinician, nasal polyps matter for several reasons. First, they cause significant quality-of-life impairment through anosmia, sleep disruption, and recurrent sinusitis — conditions that are often under-treated because patients accept them as 'normal.' Second, a unilateral nasal mass must not be automatically labelled a polyp: unilateral masses carry a differential that includes inverting papilloma, angiofibroma, and malignancy, and missing these diagnoses has serious consequences. Third, nasal polyps in a child — especially in association with bronchiectasis or failure to thrive — should prompt investigation for cystic fibrosis. The competency EN4.27 (SH level, K/S domain) requires you to both take a structured history and describe management principles, making this a core clinical skill for primary and specialist ENT practice.
RECALL
Recall from your anatomy teaching that the paranasal sinuses — frontal, maxillary, sphenoidal, and ethmoidal — communicate with the nasal cavity via narrow ostia. The anterior ethmoidal sinuses, the maxillary sinus, and the frontal sinus all drain via the ostiomeatal complex (OMC) — the functional unit formed by the uncinate process, the hiatus semilunaris, the ethmoid bulla, and the infundibulum — all located in the middle meatus of the lateral nasal wall. The posterior ethmoidal sinuses drain to the superior meatus, and the sphenoidal sinus opens above the superior turbinate. From your physiology revision, recall that the nasal mucosa is pseudostratified columnar epithelium with goblet cells and a rich submucosal network of seromucinous glands and a dense eosinophil-rich submucosa, particularly in atopic individuals. The mucociliary escalator clears mucus toward the ostia; when ostia are obstructed, mucus stagnates, bacteria colonise, and a cycle of chronic inflammation is established.
Clinical Presentation of Nasal Polyps
Nasal polyps present with a characteristic clinical syndrome that the student should be able to recognise from the history alone in most cases. The cardinal triad is nasal obstruction, anosmia (loss of smell), and rhinorrhoea — typically clear, mucoid, or mucopurulent discharge. Understanding the subtleties of each symptom and taking a careful allergy and drug history distinguishes a thorough ENT history from a superficial one.
Nasal obstruction in nasal polyps is typically bilateral, progressive, and constant rather than alternating (which would suggest vasomotor rhinitis). Patients often describe a sensation of 'something blocking both sides' that gradually worsens over months to years. Unlike allergic rhinitis alone, where obstruction fluctuates with allergen exposure, polyp-related obstruction tends to be irreversible without treatment and fails to improve with antihistamines.
Anosmia is arguably the most distressing symptom for patients and is under-reported because many patients assume it is a consequence of 'sinus problems' and have adapted to it. The mechanism is twofold: first, the polyp masses physically obstruct airflow to the olfactory cleft in the upper nasal cavity (mechanical anosmia); second, chronic inflammation at the olfactory neuroepithelium itself can cause sensorineural smell loss. Hyposmia or complete anosmia is present in up to 80–90% of patients with extensive bilateral polyps. Asking specifically about smell and taste (which is closely linked to olfaction) is essential.
Rhinorrhoea is usually anterior (dripping out of the nose) or posterior (post-nasal drip — constant throat-clearing, a 'tickle' in the throat, nocturnal cough). Purulent rhinorrhoea suggests complicating sinusitis. Watery, clear rhinorrhoea raises the possibility of a CSF leak if it is unilateral and positional.
Important history points:
- Duration and progression: years-long, slowly progressive history typical.
- Allergy: is there a personal or family history of allergic rhinitis, asthma, or eczema (the atopic triad)? Polyps in atopic individuals have a high recurrence rate post-treatment.
- Aspirin and NSAID sensitivity: ask explicitly. Aspirin-exacerbated respiratory disease (Samter's triad = nasal polyps + asthma + aspirin/NSAID sensitivity) is present in up to 10–15% of patients with CRSwNP and implies a leukotriene-dominant inflammatory pathway, with important treatment implications (avoidance of NSAIDs; leukotriene antagonists such as montelukast are especially useful).
- Previous treatment: prior topical steroid use, previous polypectomy (and recurrence rate — rapid recurrence within 6–12 months implies severe eosinophilic disease or inadequate medical treatment).
- In children: failure to thrive, recurrent chest infections, or bronchiectasis — these should prompt a sweat chloride test to exclude cystic fibrosis, in which nasal polyps occur in up to 40% of patients. Similarly, Kartagener syndrome (primary ciliary dyskinesia with situs inversus + bronchiectasis + chronic sinusitis) may present with nasal polyps.
- Headache and facial pain are NOT typical of uncomplicated nasal polyps — their presence suggests complicating sinusitis or another diagnosis.
Anatomy of the Ostiomeatal Complex and Pathophysiology of Polyp Formation
Understanding why nasal polyps form — and why they arise where they do — requires a clear model of the ostiomeatal complex and the inflammatory cascade that drives mucosal oedema.
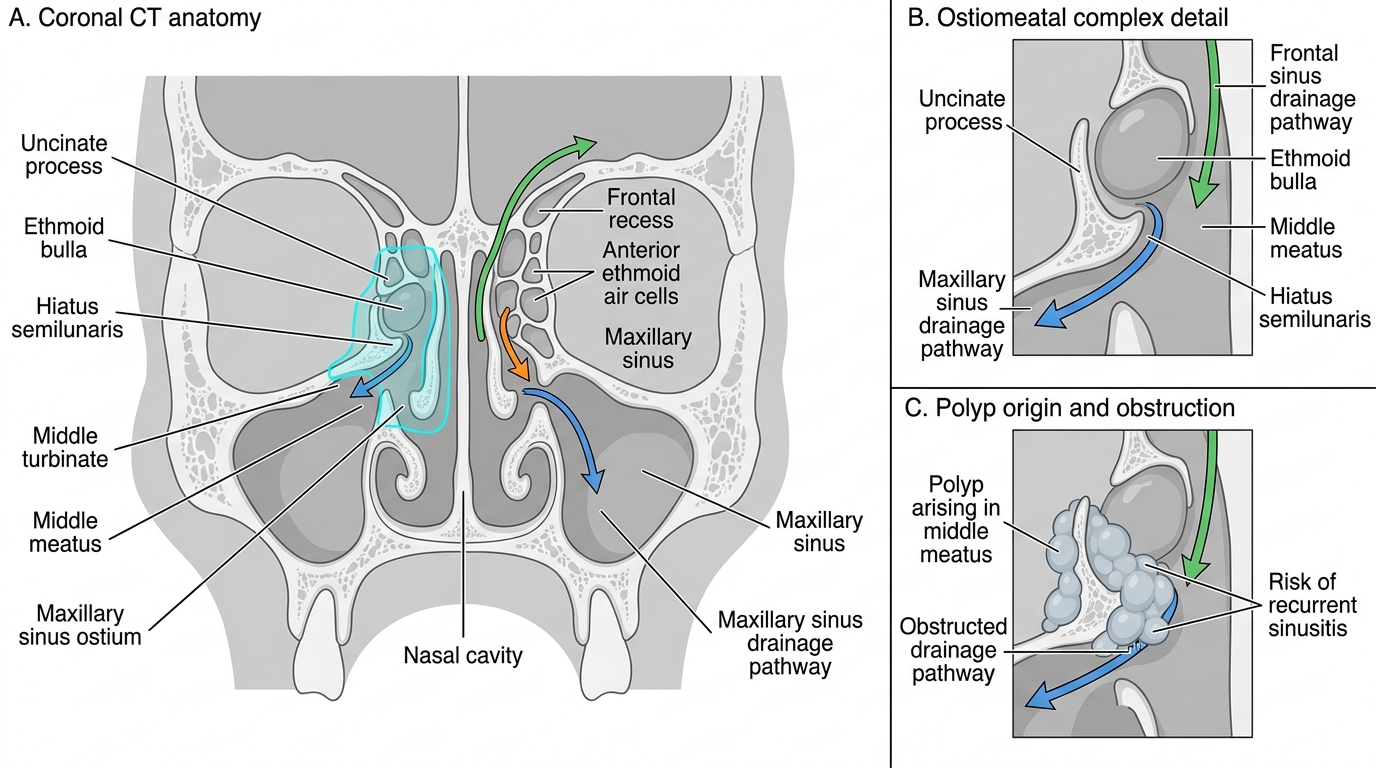
The ostiomeatal complex (OMC) is the key functional region of the lateral nasal wall. It is situated in the middle meatus, the space between the middle and inferior turbinates. Its components are the uncinate process (a thin bony projection from the lateral nasal wall), the hiatus semilunaris (a semilunar groove between the uncinate process and the ethmoid bulla), the ethmoid bulla (the largest anterior ethmoid air cell), and the infundibulum (the funnel-shaped passage through which the maxillary sinus ostium and anterior ethmoid cells drain). The frontal sinus drains via the frontal recess into the infundibulum or directly into the middle meatus. The OMC is narrow by design — normal mucus clearance depends on intact mucociliary function. Any mucosal swelling in this narrow corridor leads to ostial obstruction, sinus ventilation failure, and the cycle of chronic rhinosinusitis.
Pathophysiology of polyp formation: In the great majority of patients with bilateral ethmoidal polyps, the underlying mechanism is an eosinophil-dominant type 2 inflammatory cascade driven by epithelial barrier dysfunction. Aeroallergen or microbial exposure (including Staphylococcal superantigens) triggers release of epithelial-derived alarmins — IL-25, IL-33, and thymic stromal lymphopoietin (TSLP). These activate innate lymphoid cells type 2 (ILC2s) and Th2 lymphocytes to produce IL-4, IL-5, and IL-13. IL-5 drives eosinophil recruitment and degranulation in the lamina propria; IL-4 and IL-13 drive IgE production and goblet cell hyperplasia. The result is chronic mucosal oedema, impaired epithelial tight junctions, and excessive serous exudate — the histological substrate for polyp formation. Histologically, ethmoidal polyps show oedematous stroma with abundant eosinophils, a loosely arranged epithelium, and minimal glands — a distinctively different appearance from the antrochoanal polyp.
The Bernoulli effect in the narrow OMC contributes mechanically: high-velocity airflow through a narrowed passage creates negative pressure (Bernoulli's principle), drawing the hyper-oedematous mucosa outward to form pendant masses — the classic grape-like ethmoidal polyps that hang from the ethmoid roof and middle meatus.
Antrochoanal polyp (Killian's polyp) follows a different mechanism: a mucus retention cyst in the maxillary sinus gradually expands, protrudes through the accessory ostium (or the natural ostium enlarged by inflammation) into the nasal cavity, and extends posteriorly through the choana into the nasopharynx. It has a narrow pedicle (in contrast to the sessile base of some ethmoidal polyps) and a characteristic bilobed shape on CT — an intramaxillary component and a choanal component. Histologically it shows loose connective tissue stroma with few eosinophils — it is not a primary allergic lesion.
Ostiomeatal Complex and Middle Meatus Polyps
SELF-CHECK
A 28-year-old woman with a 3-year history of bilateral nasal blockage, anosmia, and recurrent sinusitis is found to have bilateral pale nasal polyps on anterior rhinoscopy. She also has mild asthma treated with an inhaled bronchodilator. She reports that her headaches and wheezing worsen markedly after taking ibuprofen. This presentation is most consistent with:
A. Cystic fibrosis — sweat chloride test should be performed
B. Samter's triad (aspirin-exacerbated respiratory disease) — nasal polyps, asthma, and NSAID/aspirin sensitivity
C. Antrochoanal polyp — CT required to confirm unilateral maxillary antrum origin
D. Kartagener syndrome — chest X-ray for situs inversus should be requested
Reveal Answer
Answer: B. Samter's triad (aspirin-exacerbated respiratory disease) — nasal polyps, asthma, and NSAID/aspirin sensitivity
The combination of bilateral nasal polyps, asthma, and worsening symptoms (both nasal and bronchospasm) triggered by NSAIDs/aspirin is the hallmark of Samter's triad (aspirin-exacerbated respiratory disease, AERD). The underlying mechanism is aspirin/NSAID inhibition of COX-1, which shunts arachidonic acid metabolism toward the 5-lipoxygenase pathway, producing excess leukotrienes (LTC4, LTD4) that cause bronchoconstriction and mucosal inflammation. Cystic fibrosis is a consideration in children with nasal polyps, not adults with asthma and NSAID sensitivity. Antrochoanal polyps are unilateral and unrelated to aspirin sensitivity.
ENT Examination and Investigations for Nasal Polyps
The ENT examination for nasal polyps follows a systematic sequence moving from external inspection to anterior rhinoscopy, posterior rhinoscopy, and endoscopic assessment. Investigations then confirm the extent of disease and guide surgical planning. The examination is not merely confirmatory — it determines the grade of disease, distinguishes features that should prompt a change in diagnosis, and provides the baseline against which treatment response is measured. A thorough and correctly performed anterior rhinoscopy, combined with a targeted history, is sufficient in most cases to make the clinical diagnosis; however, rigid nasal endoscopy and CT imaging are required before any surgical intervention to define disease extent and identify critical anatomical landmarks. The student should approach every nasal examination with both a diagnostic and a safety mindset — always asking whether a unilateral or bleeding mass could represent something more serious than a simple inflammatory polyp.
External inspection: Inspect for broadening of the nasal bridge (the 'frog face' deformity) — a rare but important sign of massive polyps expanding the nasal bones, most often seen in neglected or childhood cases. Nasal voice (hyponasality) may be noted in conversation.
Anterior rhinoscopy (using a Thudichum's speculum and good light):
- Ethmoidal polyps appear as pale, grey-white, translucent, smooth, grape-like masses in the middle meatus or filling the nasal cavity. They are insensitive to touch (probing them does not cause pain — a useful feature distinguishing them from turbinate mucosa, which is sensitive, and from meningoencephaloceles, which should NEVER be probed).
- They blanch with adrenaline application (unlike polyps versus meningoencephalocele, which also blanch, but this is not the key test).
- The mass is pedunculated and mobile. Antrochoanal polyp may be visible as a single mass on one side, appearing in the posterior choana on posterior rhinoscopy.
- Polyps grade: Grade 1 = confined to middle meatus; Grade 2 = extending beyond middle meatus but not obstructing the nasal airway; Grade 3 = completely obstructing nasal airway.
Posterior rhinoscopy (mirror examination): an antrochoanal polyp typically presents as a smooth mass in the choana or upper nasopharynx, seen on posterior rhinoscopy or flexible nasal endoscopy.
Nasal endoscopy (rigid 0° or 30° endoscope): provides direct visualisation of the middle meatus, OMC, sphenoethmoidal recess, and choana. It allows assessment of disease extent, documentation, and targeted biopsy where needed.
Investigations:
- CT scan of the paranasal sinuses (coronal sections without contrast) is the investigation of choice for surgical planning. It demonstrates the extent of polyposis, the degree of OMC obstruction, opacification of sinuses, and critical anatomical relationships (skull base, lamina papyracea, position of optic nerve). The Lund-Mackay score grades each sinus 0 (normal), 1 (partial opacification), or 2 (total opacification), with an additional 2 points for OMC obstruction; maximum score is 24. A score ≥12 indicates severe disease.
- Nasal endoscopy with biopsy is indicated when: the appearance is atypical (unilateral, irregular, fleshy, or bleeding mass), or when malignancy is suspected. Pale, smooth, bilateral polyps in the correct clinical context do not routinely require biopsy before initiating medical treatment.
- Allergy testing (skin prick test or serum specific IgE): identifies triggering allergens and guides allergen avoidance and immunotherapy.
- Aspirin sensitivity testing (oral challenge): rarely performed routinely; clinical history of NSAID exacerbation is usually sufficient.
- Sweat chloride test (in children): to exclude cystic fibrosis when polyps present in the paediatric age group.
- Mucociliary clearance tests (saccharin test or nasal ciliary biopsy): when Kartagener syndrome or primary ciliary dyskinesia is suspected.