Page 2 of 21
EN4.27 | Nasal Polyps — SDL Guide (Part 2)
Diagnosis and Differential Diagnosis
The diagnosis of nasal polyps is primarily clinical, confirmed by anterior rhinoscopy and nasal endoscopy. The key diagnostic challenge is to distinguish bilateral ethmoidal polyps from the antrochoanal polyp, and both from other nasal masses that may mimic polyps.
Provided image
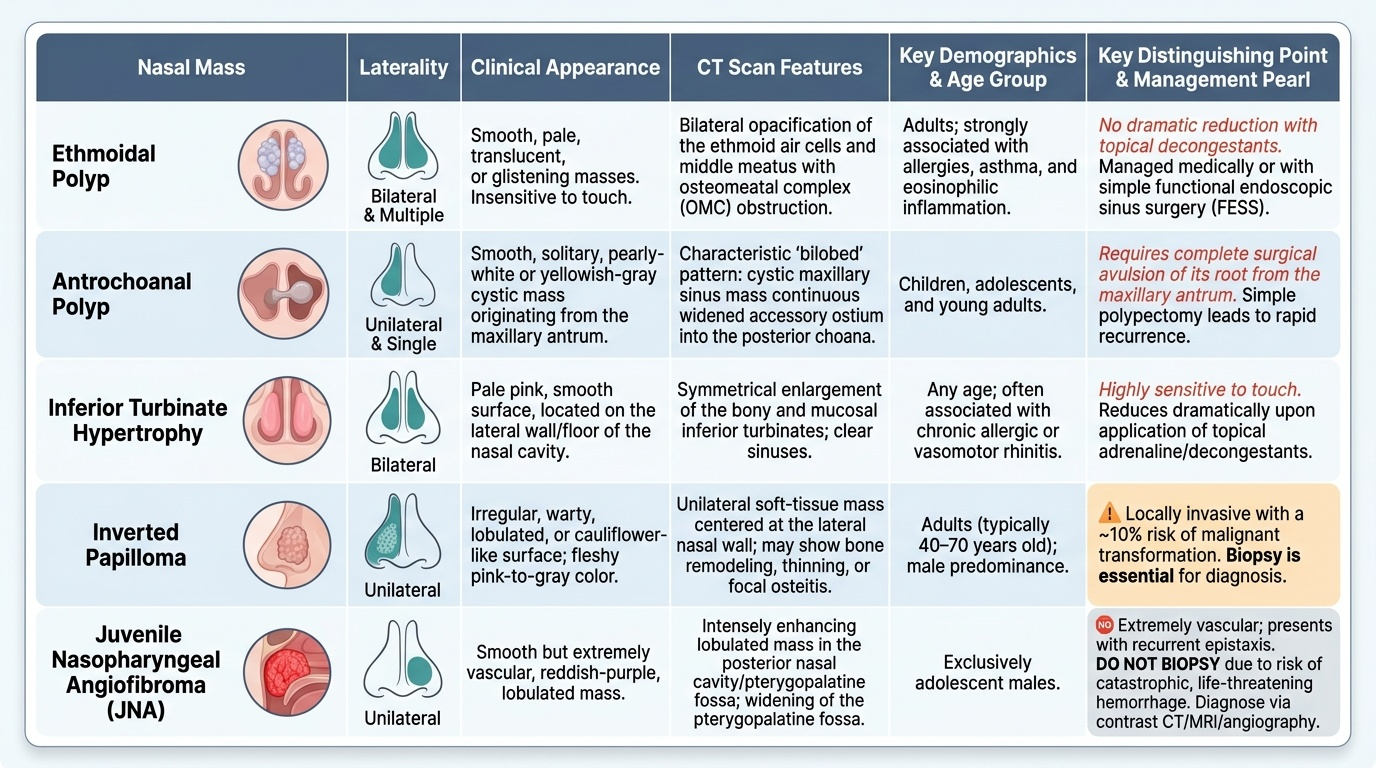
Ethmoidal polyps vs antrochoanal polyp — the most important distinction:
The EN known-trap for nasal polyps bears emphasis: ethmoidal polyps are bilateral and multiple (arising from the ethmoid mucosa bilaterally, strongly associated with allergy and eosinophilic inflammation, common in adults); antrochoanal polyp is unilateral and single (arising from the maxillary antrum, extending through the accessory ostium to the choana, commoner in children and young adults). Confusion between these two has direct management consequences — an antrochoanal polyp requires avulsion of its root from the maxillary antrum at surgery (inadequate removal causes rapid recurrence), not just a simple polypectomy.
On CT, the antrochoanal polyp shows a characteristic bilobed pattern — a cystic mass within the maxillary sinus continuous through the ostium with a posterior choanal component. Ethmoidal polyps produce bilateral ethmoid and middle meatus opacification with OMC obstruction.
Differential diagnosis of nasal masses:
- Hypertrophied inferior turbinate: pale pink, smooth, located in the floor of the nasal cavity along the lateral wall; bilateral; reduces on decongestion with topical adrenaline (polyps do not reduce as dramatically). Key distinction: turbinate hypertrophy is sensitive to touch.
- Inverted (Schneiderian) papilloma: unilateral, arises from the lateral nasal wall, has a warty or irregular surface, is locally invasive with malignant transformation potential (~10%). Biopsy is essential for any unilateral irregular mass.
- Juvenile nasopharyngeal angiofibroma (JNA): adolescent males, unilateral, extremely vascular. Presents with recurrent epistaxis and nasal obstruction. Do not biopsy — catastrophic haemorrhage. Diagnose on contrast CT/MRI and angiography.
- Meningoencephalocele: soft, pulsatile, compressible mass, often in the roof of the nasal cavity. Associated with CSF rhinorrhoea. Never probe or biopsy blindly — risk of meningitis and CSF fistula. CT and MRI of skull base required.
- Carcinoma / lymphoma: unilateral, irregular, fleshy, bleeds on touch, may be associated with facial pain, cranial nerve involvement, or cervical lymphadenopathy. Biopsy essential.
SELF-CHECK
A 14-year-old boy is brought to the ENT clinic with a 6-month history of right-sided nasal blockage and three episodes of severe right-sided epistaxis requiring nasal packing. On anterior rhinoscopy a fleshy, greyish-pink mass is seen on the right side. CT scan shows a highly vascular mass filling the right nasal cavity and extending to the nasopharynx. The most appropriate next step is:
A. Perform an immediate office biopsy to confirm the diagnosis histologically
B. Arrange contrast CT and MRI for detailed imaging, then plan surgical excision — do NOT biopsy
C. Start high-dose topical corticosteroids and review in 6 weeks
D. Perform functional endoscopic sinus surgery (FESS) under general anaesthesia
Reveal Answer
Answer: B. Arrange contrast CT and MRI for detailed imaging, then plan surgical excision — do NOT biopsy
This presentation — adolescent male, unilateral vascular nasal mass, recurrent severe epistaxis — is juvenile nasopharyngeal angiofibroma (JNA) until proven otherwise. JNA is an extremely vascular benign tumour of adolescent males. Biopsy is absolutely contraindicated because it may provoke catastrophic haemorrhage that cannot be controlled in an outpatient or office setting. Diagnosis is made on contrast CT (which shows characteristic 'Holman-Miller sign' — anterior bowing of the posterior wall of the maxillary sinus) and MRI. Pre-operative embolisation of the feeding vessels (usually the internal maxillary artery, a branch of the external carotid) is performed 24–48 hours before surgical excision to reduce intraoperative bleeding. Topical steroids have no role; FESS is not the correct procedure for JNA.
CLINICAL PEARL
The three features that should STOP you from labelling a nasal mass as a simple polyp and prompt urgent rethinking are: (1) UNILATERAL — a single unilateral nasal mass is a malignancy or serious pathology until proven otherwise; the differential includes JNA, inverted papilloma, and carcinoma. (2) BLEEDS ON TOUCH — benign nasal polyps do not bleed when gently probed; a bleeding nasal mass suggests JNA, a malignant tumour, or a haemangioma. (3) ADOLESCENT MALE with recurrent epistaxis — the classic JNA triad. Never biopsy a suspected JNA in the clinic.
Principles of Management
Management of nasal polyps is stepwise, beginning with medical therapy and escalating to surgery for medically refractory disease. The goal of treatment is symptom control, improvement in quality of life (particularly smell and nasal patency), and prevention of recurrence. Because the underlying inflammatory process is chronic and incompletely understood, recurrence is expected — the patient must understand this from the outset.
Medical management:
Topical nasal corticosteroids are the cornerstone of medical management and the first-line treatment for all grades of nasal polyps. Fluticasone furoate, mometasone furoate, budesonide, and triamcinolone nasal sprays applied as drops or sprays reduce eosinophilic mucosal inflammation, shrink polyp bulk, and slow recurrence post-surgery. Delivery technique matters: the patient should bend the head forward and downward ('head-down position') when instilling drops to maximise delivery to the middle meatus. Topical steroids are safe for long-term use at recommended doses; systemic absorption is minimal.
Systemic (oral) corticosteroids — a short course of prednisolone (0.5–1 mg/kg/day × 7–14 days, tapered) produces rapid and dramatic polyp shrinkage and smell improvement. It is used as a 'medical polypectomy' in patients with grade 3 polyps, to restore nasal patency before surgery, and to assess reversibility of disease. However, systemic steroids are unsuitable for long-term use because of well-known side effects (hyperglycaemia, osteoporosis, adrenal suppression).
Saline nasal douching (isotonic or hypertonic saline irrigation) improves mucociliary clearance, reduces crusting, and provides symptomatic relief. It is recommended as an adjunct to corticosteroid therapy.
Antihistamines are useful for the allergic rhinitis component but do not directly shrink polyps. Oral antihistamines and allergen avoidance are prescribed as part of managing the atopic background.
Leukotriene antagonists (montelukast): particularly useful in Samter's triad, where the leukotriene pathway is dominant. Aspirin desensitisation under specialist supervision is also an option in AERD.
Biologics (IL-4Rα inhibitors — dupilumab): Dupilumab (anti-IL-4Rα monoclonal antibody) blocks both IL-4 and IL-13 signalling and is now approved for severe uncontrolled CRSwNP in adults who have had inadequate response to corticosteroids. In the pivotal SINUS-24 and SINUS-52 trials, dupilumab significantly reduced polyp scores, improved nasal congestion, and restored sense of smell. Biologics are reserved for severe refractory cases because of high cost.
Surgical management:
Functional endoscopic sinus surgery (FESS) is the standard surgical procedure for nasal polyps that are refractory to medical treatment. Under general anaesthesia, the endoscopic technique removes polyp tissue, opens the OMC, enlarges the natural ostia of the maxillary, frontal, and ethmoid sinuses, and restores ventilation and drainage. FESS does not cure the underlying inflammatory disease — post-operative topical corticosteroids are mandatory to reduce recurrence. Complications of FESS include orbital haematoma (from medial wall breach of the orbit — the lamina papyracea), CSF leak (from inadvertent skull base breach at the cribriform plate or fovea ethmoidalis), and bleeding.
Simple polypectomy (avulsion with a nasal snare under local anaesthetic) has a high recurrence rate and is no longer the preferred technique except for isolated antrochoanal polyps in resource-limited settings. Antrochoanal polyp requires avulsion of the root from the maxillary antrum (either endoscopically via the antral ostium or via a Caldwell-Luc approach if endoscopic access is inadequate) — simple choanal avulsion without root removal inevitably recurs.
Summary of management approach:
| Stage | Intervention |
|---|---|
| Grade 1–2, first presentation | Topical corticosteroids × 3 months, saline douching, allergen control |
| Grade 3 or prior failure of topical therapy | Short course oral steroids + topical steroids; review at 6 weeks |
| Persistent symptoms / disease after 2 medical cycles | Refer for FESS + post-op topical steroids |
| Rapid/multiple recurrences, severe eosinophilic disease | Biologic therapy (dupilumab) consideration |
| Samter's triad | Montelukast, aspirin desensitisation, FESS if refractory |
Self-Assessment: Nasal Polyps
Use these structured questions to consolidate your learning before moving to the formal self-check questions at the end of this module. For each scenario, work through your reasoning before reading the explanation.
Question 1: A 10-year-old child presents with unilateral left nasal blockage of 1-year duration and a sensation of something in the throat. There is no history of allergies or asthma. Anterior rhinoscopy shows a smooth pale mass on the left side. Posterior rhinoscopy reveals a mass hanging into the nasopharynx. CT shows a cystic mass in the left maxillary antrum with an extension through the accessory ostium into the choana. What is the diagnosis, and what surgical approach would you plan?
Expected answer: Antrochoanal polyp (Killian's polyp). The unilateral location, young age, CT showing bilobed maxillary-choanal mass, and absence of atopy are all characteristic. Surgical treatment requires endoscopic removal including avulsion of the antral root (through the enlarged maxillary ostium endoscopically) — simple choanal removal leads to near-certain recurrence.
Question 2: A 45-year-old patient with known bilateral nasal polyps is scheduled for FESS. You counsel her about surgical risks. Which two anatomical boundaries, if breached, produce the most serious immediate complications of FESS?
Expected answer: (1) The lamina papyracea (medial wall of the orbit) — breach causes orbital haematoma or fat prolapse, with risk of blindness from optic nerve compression. (2) The cribriform plate / fovea ethmoidalis (skull base) — breach causes CSF leak and risk of meningitis. These define the 'danger triangle' of FESS and should be carefully identified on the pre-operative CT.
Question 3: Explain why complete anosmia in a patient with bilateral nasal polyps may NOT fully recover even after successful surgical clearance of the polyps.
Expected answer: While much of the smell loss in nasal polyps is conductive anosmia (physical obstruction of airflow to the olfactory cleft), prolonged inflammation also causes sensorineural damage to the olfactory neuroepithelium itself (olfactory receptor neurons are damaged and replaced slowly). Therefore, even after surgical clearance, olfactory recovery may be incomplete, particularly in patients who have had severe, long-standing disease. This is an important point to include when counselling patients pre-operatively.
SELF-CHECK
A patient with bilateral nasal polyps and a history of asthma presents for surgical planning. She reports that her asthma consistently worsens every time she takes paracetamol or ibuprofen. CT shows bilateral ethmoid opacification with a Lund-Mackay score of 18. After FESS, which medication is most important to prescribe long-term to reduce polyp recurrence?
A. Oral cetirizine (antihistamine) daily
B. Topical intranasal corticosteroid spray daily
C. Oral prednisolone 5 mg daily as maintenance
D. Amoxicillin-clavulanate for 3 months post-operatively
Reveal Answer
Answer: B. Topical intranasal corticosteroid spray daily
Post-operative topical intranasal corticosteroids are the cornerstone of long-term management after FESS for nasal polyps. They reduce mucosal eosinophilic inflammation at the site of polyp origin and are the most evidence-based intervention to reduce recurrence rates. Oral antihistamines help the allergic rhinitis component but do not reduce polyp recurrence. Long-term oral prednisolone is not appropriate for maintenance because of systemic side effects (osteoporosis, hyperglycaemia, adrenal suppression). Prophylactic antibiotics have no role in post-FESS polyp management. Note: the asthma + NSAID sensitivity pattern in this question is Samter's triad — in such patients, aspirin desensitisation and montelukast are additional options, but topical steroids remain the essential post-surgical treatment.