Page 6 of 15
PE1.2 | Growth Assessment and Anthropometry — SDL Guide (Part 3)
Applied Growth Assessment: Clinical Scenarios and Programme Context
The skill of growth assessment is practised in two distinct contexts in India: the clinical (hospital/health-facility) setting and the community/programme setting. Both require the same technical accuracy but differ in the resources available, the population being screened, and the decision pathways that follow. The transition from measurement technique and chart interpretation to clinical action is where the skill acquires its full meaning. A correctly measured, correctly plotted, correctly classified nutritional assessment that is then communicated to a caregiver without a clear action plan—dietary targets, review timeline, referral threshold—delivers only a fraction of its potential value. The final-year MBBS student must therefore be able to do all three in sequence: measure accurately, interpret correctly using WHO/IMNCI criteria, and then translate the interpretation into a management decision that the caregiver can act on. Both programme and clinical contexts require this complete three-part competency, though the instruments, reference charts, and escalation pathways differ between them.
In the health-facility setting, growth assessment is integrated into:
- Routine well-child visits and immunisation contacts: measure weight (every contact), length/height (every contact for under-2, 3-monthly for 2–5 years), and HC (every contact for under-2). Plot on the child health card. If the child is crossing percentiles downward, initiate evaluation.
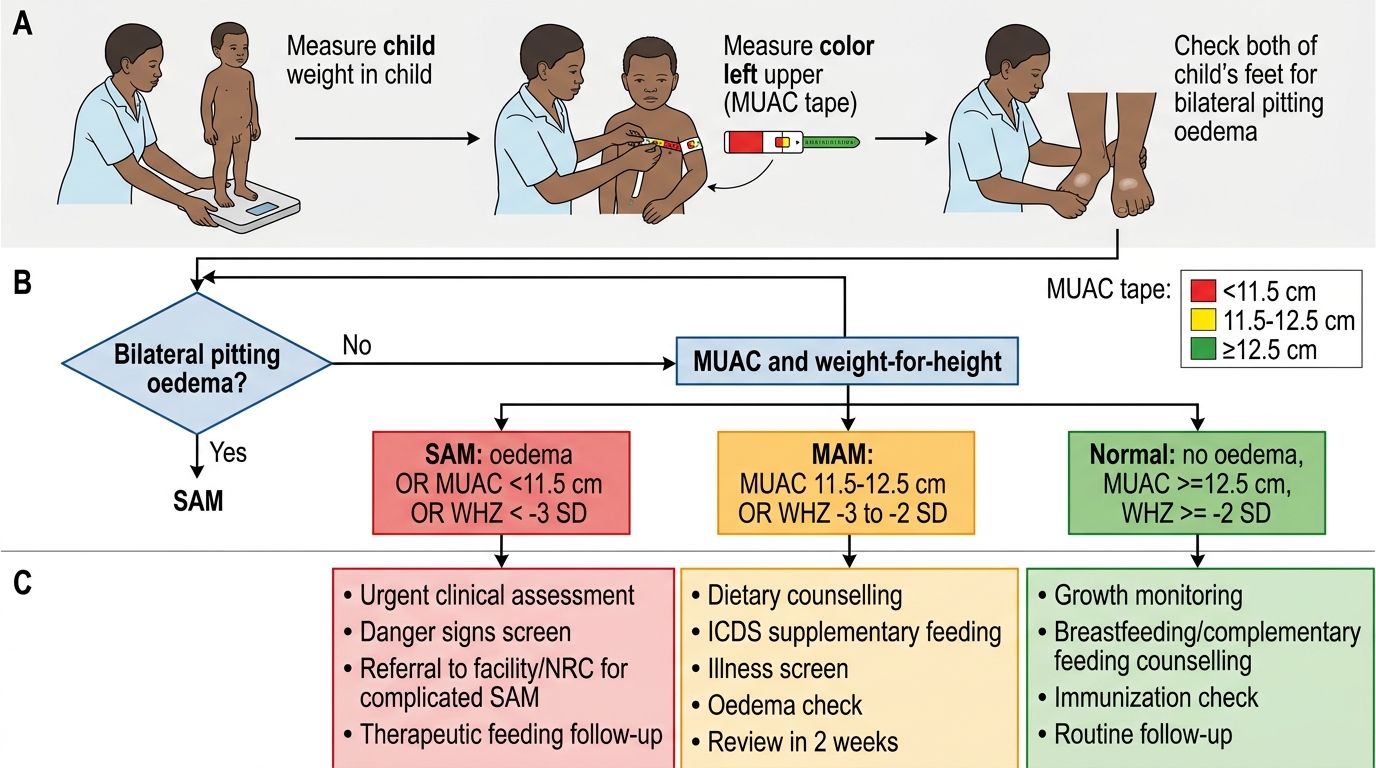
- Sick-child consultations (IMNCI): check for visible severe wasting, bilateral oedema, and MUAC. A child with any SAM criterion requires inpatient admission (or referral) and management with therapeutic feeding (F-75/F-100 ready-to-use therapeutic food per WHO/UNICEF guidelines).
- Inpatient nutrition management: serial daily weights (same time, same scale) are the primary monitoring tool during therapeutic feeding. A child gaining <5 g/kg/day during the rehabilitation phase is not responding adequately.
In the community setting (ICDS/Anganwadi programme):
- Monthly weighing of all children under 3 years using a Salter spring scale or digital scale at the Anganwadi centre.
- Colour-coded growth chart (red/yellow/green) on the child health card communicates nutritional status to the mother without requiring her to interpret SD scores.
- MUAC screening by ASHA workers during home visits identifies SAM cases for referral to NRC (Nutritional Rehabilitation Centre) or PHC.
Counselling parents is an integral part of growth assessment. After plotting and interpreting a measurement, the clinician should:
1. Show the parent where the child's point is on the chart and what it means in plain language.
2. Explain the direction of the curve (trajectory) — whether it is following a centile or drifting down.
3. Give specific, actionable dietary counselling (not 'feed more' but 'give an extra meal of X at time Y, continue breastfeeding').
4. Set a specific review date with a clear expected weight gain as a target.
Applying this module's skills to the opening clinical scenario: the 2-year-old boy with weight 7.8 kg, length 80 cm, MUAC 11.0 cm, no oedema. MUAC <11.5 cm = SAM. Plot weight-for-length on the WHO chart: expected weight for 80 cm length is approximately 10.5–11 kg; 7.8 kg is approximately −3.5 SD below the median. Confirmed SAM. This child requires inpatient or NRC-based therapeutic feeding, not outpatient management.
IMNCI Growth Assessment and Nutrition Classification
Self-Assessment: Growth Assessment and Anthropometry
Work through these scenarios before your next outpatient paediatrics posting.
Scenario 1: An Anganwadi worker records a child's MUAC as 12.0 cm at a monthly weighing. The mother says the child was 12.8 cm last month. How do you classify nutritional status now, and what is your next step?
(MUAC 12.0 cm = MAM range [11.5–12.5 cm]. Downward trend from 12.8 to 12.0 cm in one month is concerning. Classification = MAM. Action: refer for dietary counselling and supplementary feeding through ICDS, review in 2 weeks, screen for illness, check for oedema.)
Scenario 2: A 4-year-old girl has weight-for-height of −1.8 SD, height-for-age of −2.6 SD, and MUAC of 13.5 cm. How do you describe her nutritional status?
(She is stunted [height-for-age <−2 SD] but not acutely malnourished [weight-for-height and MUAC both normal]. This pattern suggests past chronic malnutrition with current adequate nutritional status. Management focuses on dietary adequacy, micronutrient supplementation, deworming, and addressing chronic infection risk—not therapeutic feeding.)
Scenario 3: You are measuring a 22-month-old for the first time. List the five steps you will take and the measurements you will obtain.
(1) Weigh using infant scale with tare, record to 0.1 kg. (2) Measure recumbent length with infantometer [under 2 years], two-measurer technique, record to 0.1 cm. (3) Measure head circumference with non-stretchable tape over maximum occipital circumference, record to 0.1 cm. (4) Measure MUAC at left arm mid-point. (5) Plot weight-for-age, length-for-age, weight-for-length, and HC-for-age on WHO 2006 charts. Interpret each index.)