Page 15 of 26
PE18.{7,13} | Immunization Counseling and Consent — SDL Guide
Learning Objectives
- Educate and counsel a parent or caregiver about immunization — benefits, schedule, AEFI, and home care after vaccination
- Explain the concept of implied consent in immunization services and its legal and ethical basis
- Distinguish implied consent from express consent and state when each is appropriate
- Apply a structured counselling framework to address vaccine hesitancy using evidence-based, respectful communication
- Counsel a parent about expected post-vaccination reactions and the red-flag signs that require a return visit
INSTRUCTIONS
A technically perfect vaccine, given at exactly the right age, through the correct cold chain, is wasted if the parent refuses it or leaves without understanding what to do at home. The clinician's ability to communicate about immunization — to counsel effectively, to address hesitancy respectfully, and to secure consent appropriately — determines whether the vaccine programme translates to actual child protection. Competency PE18.7 (counselling) and PE18.13 (implied consent) are the communication and legal pillars of immunization practice.
References
- Ghai Essential Pediatrics, 9th edition, Chapter on Immunization (textbook)
- WHO SAGE Working Group on Vaccine Hesitancy: Report, October 2014 (guideline)
- IAP Advisory Committee on Vaccines and Immunization Practices (ACVIP) 2024 — Communication Guide (guideline)
- Park's Textbook of Preventive and Social Medicine — Ethics and Communication in Immunization (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 9 AM at the paediatric OPD. A father brings his 6-week-old baby boy for the first round of vaccines. Before the nurse can begin, he says: 'Doctor, I saw on WhatsApp that the vaccine has dangerous chemicals in it. My neighbour said her baby cried for 2 days after pentavalent — is that true? And my wife is worried the polio drops will give him polio. Can we just skip the shots and do the polio drops only?' You have 4 other patients waiting. How do you respond — efficiently, respectfully, and effectively — to address each concern while still proceeding with vaccination?
WHY THIS MATTERS
Vaccine hesitancy is a global public health crisis identified by the WHO as one of the top 10 threats to global health. In India, patchy immunization coverage — with significant gaps in urban slums, remote rural areas, and some communities with specific religious or cultural beliefs — is partly driven by parental hesitancy and poor counselling at point of care. The single most effective intervention for vaccine hesitancy is a strong, personalised recommendation from the healthcare provider, delivered with empathy and evidence. As a doctor, your conversation with a parent about vaccination is not peripheral to the technical act of immunization — it is as important as the vaccine itself.
RECALL
Recall from your NIS module: the benefits of each vaccine in the schedule, the common expected side effects (DPT fever, BCG ulcer, post-MR rash), the rare serious AEFI (anaphylaxis, febrile seizures), and the true versus false contraindications. These facts are the content of counselling — you cannot counsel effectively about a vaccine you do not know. Also recall from Community Medicine and Sociology: health-seeking behaviour is influenced by perceived susceptibility to disease, perceived severity, perceived benefits of the action, and perceived barriers — the Health Belief Model. Vaccine hesitancy maps directly onto this: parents who perceive low disease severity, low vaccine benefit, or high side-effect risk are hesitant.
Immunization Communication: Why Counselling Matters
Vaccine hesitancy is defined by the WHO SAGE Working Group (2014) as the delay in acceptance or refusal of vaccines despite availability of vaccination services. It is complex and context-specific, existing on a spectrum from mild uncertainty to outright refusal. Crucially, it is NOT synonymous with vaccine refusal — many hesitant parents are ambivalent, open to information, and can be persuaded by a credible, empathetic healthcare provider. Understanding this spectrum is clinically important: the approach to a mildly concerned parent differs fundamentally from the approach to an ideologically committed anti-vaccination parent. The spectrum also means that the same parent's hesitancy can change over time — a parent who refused at 6 weeks may accept at 10 weeks after a trusted family member or community health worker provides reassurance, or after their child survives a measles exposure in a partially vaccinated community. Recognising hesitancy as a dynamic, addressable state — rather than a fixed position — is the attitudinal foundation of effective immunization counselling.
The WHO 3Cs model identifies three root-cause determinants of vaccine hesitancy:
• Complacency: The parent does not perceive the vaccine-preventable disease as a real or serious threat ('polio is eradicated, why does my child need OPV?'; 'measles is not serious'). This is particularly common for diseases that vaccines have made rare — paradoxically, vaccination success creates complacency about the need to continue vaccinating.
• Convenience: Structural barriers — distance from immunization site, cost of transport, inconvenient timing, long waiting times, missed school or work, language barriers with health workers — prevent or delay vaccination even when the parent is willing.
• Confidence: Lack of trust in vaccine safety or efficacy, distrust of the healthcare system or pharmaceutical companies, religious or cultural objections, misinformation from social media or community networks ('MMR causes autism', 'vaccines contain pork', 'the government is conducting experiments').
Each 'C' requires a different response. Complacency is addressed by reinstating the perception of disease severity and community risk. Convenience is addressed by systemic changes (outreach, home visits, community mobilisation) and by addressing the individual family's barriers. Confidence is addressed by empathetic, evidence-based communication from a trusted provider.
The evidence is consistent: the provider's recommendation is the most influential single factor in vaccine uptake. Parents who receive a clear, confident, personalised recommendation from a doctor or nurse are significantly more likely to vaccinate than those who receive a generic poster or pamphlet. This makes every clinical encounter at the immunization session an opportunity to protect a child.
Governing Principles: Informed Consent and Implied Consent
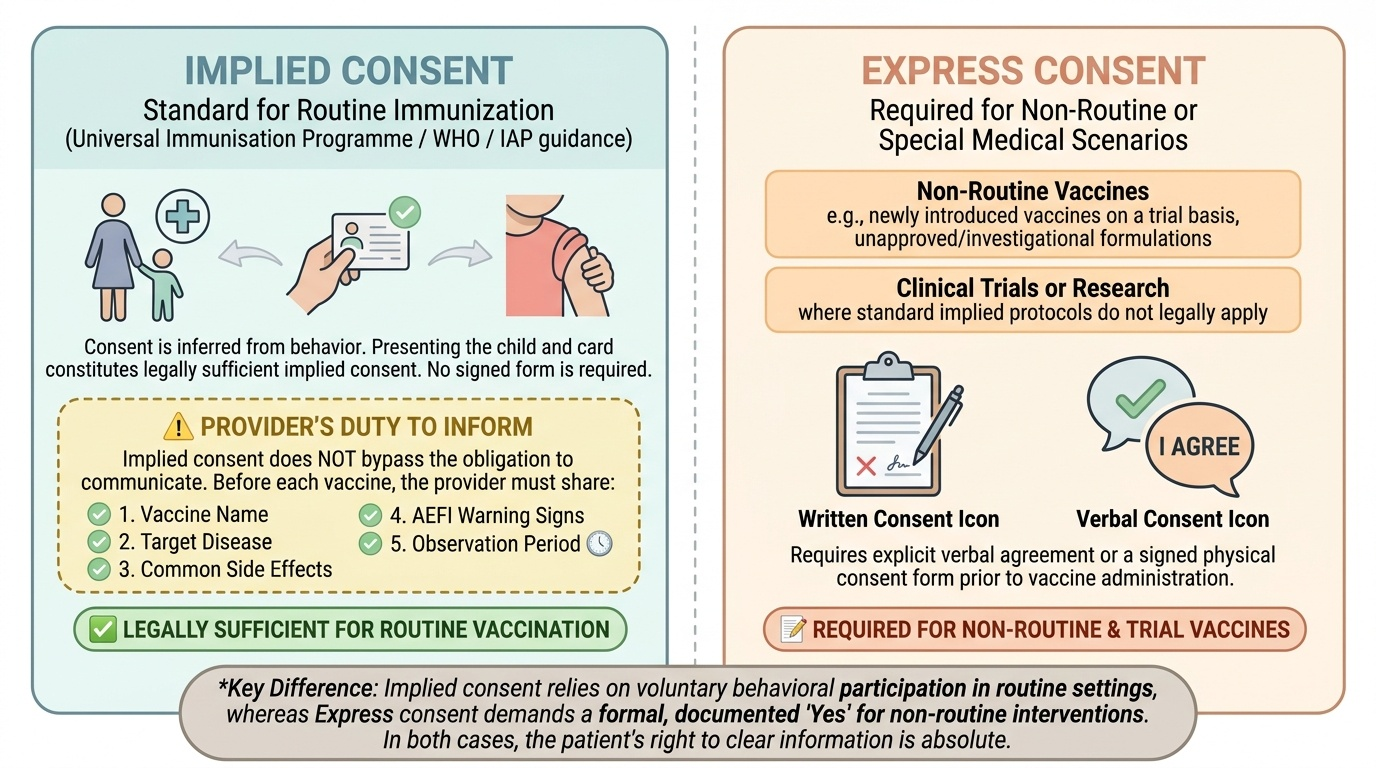
Consent for medical procedures, including vaccination, is grounded in the ethical principles of autonomy (the right of individuals to make informed decisions about their own or their child's health) and non-maleficence (the duty not to harm). In legal and ethical practice, consent for immunization typically operates under the principle of implied consent — but this does not mean the provider has no duty to inform.
Provided image
Implied consent is consent inferred from behaviour rather than explicitly stated. In the context of immunization, the parent who brings a child to a scheduled immunization clinic, presents the immunization card, and rolls up the child's sleeve is, by that behaviour, consenting to vaccination — the act of presenting the child in a context known to be a vaccine session constitutes implied consent. This is the legal standard for routine immunization under the Universal Immunisation Programme in India and is consistent with WHO and IAP guidance. Implied consent does NOT require a signed form or explicit verbal agreement for each vaccine in a routine session.
However, implied consent does not abrogate the duty to inform. The healthcare provider retains the professional and ethical obligation to inform the parent, before each vaccine is given, of: (1) which vaccine is being administered; (2) what disease(s) it protects against; (3) common expected side effects and how to manage them at home; (4) rare serious AEFI and the warning signs that require a return to the clinic; and (5) the recommended post-vaccination observation period (15–30 minutes at the site for anaphylaxis). Failure to provide this basic information does not make the vaccination illegal, but it constitutes a communication deficit that falls below professional standards.
Express consent — explicit verbal or written agreement — is required for: non-routine vaccines (e.g., a new vaccine being introduced on a trial basis, an unlicensed vaccine), vaccines given under research or clinical trial protocols, and vaccines requiring specific risk disclosure (e.g., yellow fever vaccine in an immunocompromised child). The immunization card serves as a written record of vaccination but is not a formal consent form for routine NIS vaccines.
Parental autonomy and refusal: A parent has the legal right in India to refuse vaccination for their child. This right must be respected. However, the provider has an obligation to ensure the refusal is informed — the parent must understand what disease the child is at risk of, that the disease can be serious or fatal, and that the vaccine is safe and effective. If, after full information, the parent still declines, the provider must: (a) document the refusal in the immunization record; (b) schedule a follow-up to revisit the decision; (c) NOT abandon or penalise the family for refusing. The child has no legal voice in India for routine vaccination decisions, but older adolescents' assent should be sought as a matter of professional ethics, even when parental consent is the legal standard.
SELF-CHECK
A mother presents her 6-month-old at a routine immunization session. Without being explicitly asked, she presents the immunization card and exposes the infant's thigh. The nurse proceeds to administer the vaccine. Which type of consent applies in this scenario?
A. No consent — the nurse should have asked verbally before proceeding
B. Implied consent — the mother's behaviour (presenting the child) constitutes consent
C. Express consent — a signed form is required for every vaccine under Indian law
D. Informed consent is not required for children — only for adult patients
Reveal Answer
Answer: B. Implied consent — the mother's behaviour (presenting the child) constitutes consent
This is the classic scenario for implied consent: the parent's behaviour — bringing the child to a vaccine session, presenting the immunization card, exposing the injection site — constitutes consent by implication. Express written consent is not required for routine NIS vaccines. However, the nurse still has a duty to inform the parent briefly about what is being given, expected reactions, and what to watch for at home — the implied consent standard does not eliminate the duty to inform. Option D is incorrect — consent (including by implication or via a parent/guardian for a child) is required for all medical procedures, including vaccination.
Counselling Technique: What to Tell Parents and How
Effective immunization counselling is brief, evidence-based, parent-centred, and action-oriented. It is not a lecture — it is a targeted conversation. Research on health communication shows that parents retain information best when it is: delivered by a trusted professional, personalised to their specific concern, framed positively (benefit-focused before risk-disclosure), and followed by a clear action recommendation.
Provided image
A structured approach to pre-vaccination counselling ensures completeness without consuming excessive consultation time. The following five elements should be communicated (or verified as understood) before each vaccine:
1. What is being given and why:
'Today, your baby is receiving the pentavalent vaccine — this one injection protects against five serious diseases: diphtheria, whooping cough (pertussis), tetanus, hepatitis B, and the most common cause of meningitis in babies [Hib]. Without this, even a small cut can cause tetanus — and whooping cough can be fatal in infants this young.'
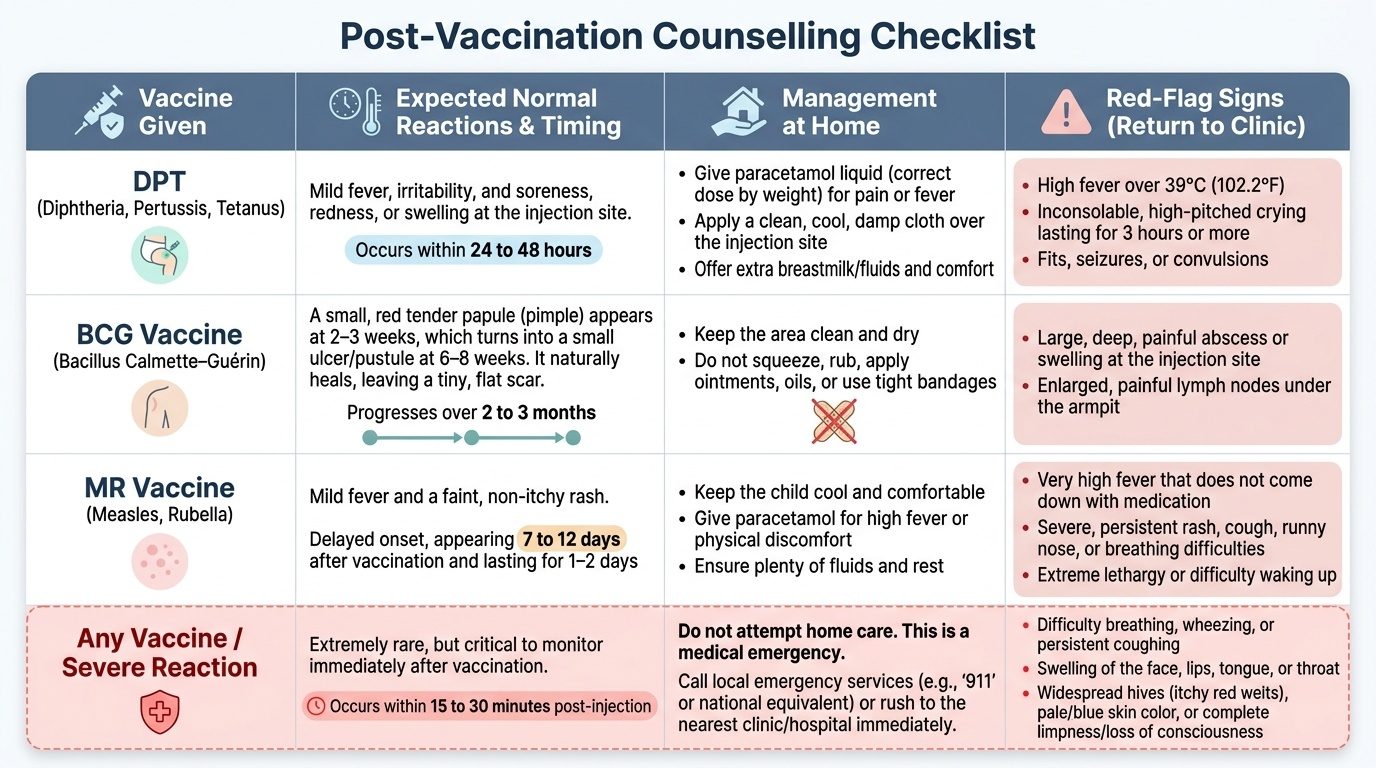
2. Common expected side effects — normalise and reassure:
'After the injection, your baby may have some pain, redness, and swelling at the injection site for 1–2 days — this is normal and shows the immune system is responding. Your baby may also have a mild fever (37.5–38.5°C) for 1–2 days. You can give paracetamol drops [15 mg/kg per dose, every 6 hours if needed, up to 4 doses in 24 hours] for pain and fever. Do NOT use aspirin.'
3. Specific vaccine reactions:
'For BCG, a small red lump will appear at the injection site after 2–4 weeks, turn into a small ulcer, and then heal to leave a small scar — this is completely expected and shows the vaccine has worked. Do not squeeze it or apply any ointment. For the MR vaccine, your baby may get a mild fever and rash at 7–12 days after the injection — this is not contagious and resolves on its own.'
4. Rare serious AEFI — red flags to return:
'Very rarely, a baby can have a serious reaction to a vaccine, called anaphylaxis — signs include difficulty breathing, severe swelling of the face or throat, skin turning pale and sweaty, or the baby becoming very limp within 15–30 minutes of the injection. If any of these signs occur, bring the baby back to the clinic immediately [or to any emergency department].'
5. Observation period and next steps:
'Please stay in the waiting area for 15–30 minutes after the injection. Your next vaccines are due at [age — give specific appointment]. Please bring the immunization card every time.'
CLINICAL PEARL
The MMR-autism myth — how to respond: The claim that the MMR vaccine causes autism originates from a 1998 study by Wakefield et al. in The Lancet that has since been fully retracted (2010) and the author struck off the medical register for fraud and ethical violations. Subsequent studies involving millions of children across multiple countries have found absolutely no association between MMR and autism. When a parent raises this concern, do not dismiss it — acknowledge it: 'I hear you — many parents have worried about this. Let me tell you what the evidence actually shows.' Then explain the retraction, the scale of subsequent studies, and the serious consequences of measles in unvaccinated children. Avoid becoming defensive or dismissive — the parent is genuinely concerned for their child's wellbeing, and that concern deserves respect even when the information driving it is wrong.