Page 16 of 26
PE18.{7,13} | Immunization Counseling and Consent — SDL Guide (Part 2)
Addressing Vaccine Hesitancy and Refusal
Vaccine hesitancy requires differentiated responses depending on its root cause. Generic reassurance ('vaccines are safe') without addressing the specific concern is ineffective and can increase distrust. The first step is to identify the nature of the hesitancy by listening without interrupting, then to address the specific concern with evidence and empathy.
Common concerns and evidence-based responses:
'My child gets too many vaccines at once — it overloads the immune system.'
Response: 'Your baby's immune system faces thousands of antigens every day from bacteria and viruses in the environment. The vaccines given today contain a tiny number of antigens — far fewer than those in everyday air, food, and contact. Multiple studies have shown no harm from giving several vaccines at the same visit, and this is actually safer than multiple visits because it protects the baby earlier and reduces pain from repeated clinic trips.'
'The polio drops will give my baby polio.'
Response: 'The OPV drops contain a weakened version of the poliovirus that cannot cause full polio in a healthy baby. In very rare cases [1 per 2.7 million doses], it could theoretically affect a baby with a severe immune problem — which is why we have switched to the injectable fractional IPV alongside the drops. But for a healthy baby, the drops are safe and provide excellent protection against the real poliovirus.'
'Vaccines contain pork/non-halal/non-kosher ingredients — it is against our religion.'
Response: This requires careful, respectful engagement. In practice, trace gelatin (porcine-derived) is used as a stabiliser in some lyophilised vaccines (MMR in some formulations). The Islamic jurisprudence position (fatwa from Al-Azhar and other authorities) generally permits use of vaccines where the gelatin has been transformed (istihalah) and where the greater harm of the disease outweighs the concern. The provider should acknowledge the concern, refer to available religious guidance if requested, and if the parent still objects, document carefully and schedule a follow-up. Do NOT trivialise religious concerns.
'A neighbour said their baby became deaf after MMR.'
Response: 'I understand why that story is frightening. The MR/MMR vaccine has been given to billions of children worldwide and is one of the most studied vaccines in history. There is no evidence it causes deafness. The vaccine does cause a mild fever and rash in some children at 7–12 days — this is expected and harmless. True nerve deafness from measles disease itself, on the other hand, is a well-documented complication of natural measles infection.'
When a parent refuses after complete information:
Document the refusal in the immunization record: note the date, that full information was provided, that risks of non-vaccination were explained, and that the parent declined. Schedule a follow-up. Never threaten, coerce, or penalise the family. Never vaccinate a child against the explicit refusal of a legally responsible parent — doing so constitutes battery regardless of your belief that it is in the child's best interest.
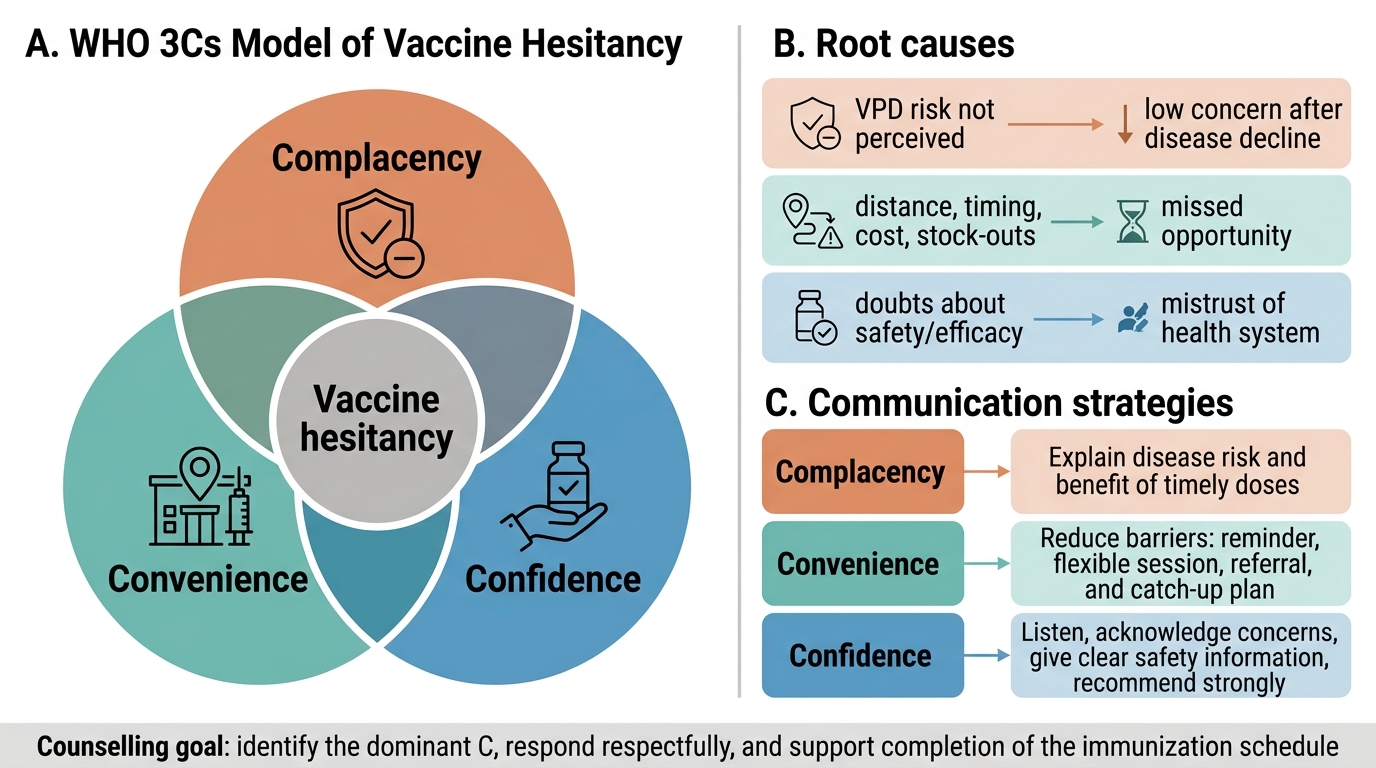
WHO 3Cs Model of Vaccine Hesitancy
Applied Communication Practice
This section applies the counselling skills from the preceding blocks to the post-vaccination interaction — the communication that happens after the vaccine has been given. This is equally important to pre-vaccination counselling, because parents' experience of the immediate post-vaccination period heavily influences their willingness to return for subsequent doses.
The post-vaccination interaction has four components:
1. Observation and monitoring:
All vaccinated children should remain at the immunization site for 15–30 minutes after each vaccination, regardless of which vaccine was given. This observation window is the time during which anaphylaxis — the only truly acute life-threatening AEFI — is most likely to occur (onset typically within 15 minutes). The immunization site must have adrenaline (epinephrine 1:1000) available; the provider must know the dose (0.01 mg/kg IM, anterolateral thigh; maximum 0.5 mg per dose) and the technique. During the observation period, parents should be counselled not to leave and should know to alert staff immediately if the child shows any signs of breathing difficulty, collapse, or skin changes.
2. Standardised post-vaccination counselling script (PVCS):
Before the family leaves, provide a brief summary:
• What reactions are expected and when (DPT: local pain/swelling/fever within 24–48 hours; BCG: local lump/ulcer at 2–4 weeks; MR: fever/rash at 7–12 days)
• What to do at home: paracetamol 15 mg/kg/dose for fever/pain; cool compress for injection site swelling; continue breastfeeding
• Red-flag signs requiring immediate return: breathing difficulty, extreme pallor, limpness, persistent high fever >39°C lasting >3 days, convulsions, any unexpected severe reaction
• Next appointment: write the date and vaccines due in the immunization card
3. Documentation of vaccination and counselling:
Record in the immunization card: vaccine name, date, batch number, site, and the health worker's initials. Document in the clinic record that counselling was provided and the parent demonstrated understanding (verbal acknowledgement or ask-back technique: 'Can you tell me what reactions to watch for at home?').
4. Managing AEFI at the session:
If an AEFI occurs during the observation period, respond immediately: for anaphylaxis, administer adrenaline IM without delay, call for emergency assistance, monitor and document. All AEFI must be reported to the block/district surveillance officer using the standard AEFI reporting form (Government of India). Document the AEFI in the immunization card with a note for the next health worker managing the child. Do NOT administer the same vaccine in subsequent doses if the child experienced anaphylaxis to it — refer to a specialist centre for further assessment.
SELF-CHECK
A mother asks: 'After the last pentavalent injection, my baby had a fever of 38.2°C for 2 days and cried a lot. This time I don't want the next dose — I'm scared.' What is the most appropriate counselling response?
A. Agree to skip today's dose since the child had a reaction previously
B. Tell her the previous reaction was an AEFI and the vaccine must be stopped permanently
C. Acknowledge her concern, explain that mild fever and irritability are expected post-DPT reactions (not a true contraindication), advise paracetamol after this dose, and proceed with vaccination
D. Give only the HepB and Hib components of pentavalent and omit the DPT component
Reveal Answer
Answer: C. Acknowledge her concern, explain that mild fever and irritability are expected post-DPT reactions (not a true contraindication), advise paracetamol after this dose, and proceed with vaccination
Mild fever and irritability after DPT/pentavalent are common, expected local and systemic reactions — they are NOT contraindications to further doses. A contraindication to the pertussis component of DPT is encephalopathy within 7 days of a prior dose, or anaphylaxis. Mild fever does not qualify. The correct response is to acknowledge the mother's concern empathetically (validating her worry shows respect), explain that these reactions are expected and self-limiting, advise prophylactic paracetamol (15 mg/kg) after this dose to reduce fever, and proceed with the scheduled vaccine. Skipping or permanently stopping is incorrect clinical practice. Splitting pentavalent into components is not operationally or clinically indicated for this reason.
Self-Assessment
The following scenarios test your ability to integrate counselling knowledge, consent principles, and AEFI management into realistic clinical communication. Each scenario represents a real situation you will encounter in your final-year posting at a PHC immunization session, paediatric OPD, or community health camp. Effective response to these cases requires not just knowledge of the correct answer but the ability to communicate it in a way that maintains parental trust and results in the child being protected — the ultimate clinical outcome measure for immunization counselling. These are also representative of the communication-and-ethics questions that appear in clinical oral examinations and structured OSCEs: the examiner is not just assessing what you know, but whether you can apply it under the pressure of a real or simulated consultation.
- A father of a 9-month-old child asks: 'My child received the MR vaccine 10 days ago and now has a fever and rash. Did the vaccine cause this? Should I go to casualty?' How do you respond — what would you tell him, and what clinical assessment would you do?
- You are at an immunization session and about to give pentavalent to a 6-week-old infant. The mother says nothing and does not sign any form. Is this vaccination legally permissible? What is the ethical obligation of the health worker before proceeding?
- A mother consistently refuses BCG for her newborn, citing religious beliefs. The baby is now 6 weeks old. How would you approach this consultation? What would you say, what would you document, and what would you do if she continues to refuse?
- After receiving fIPV at 14 weeks, a baby develops difficulty breathing and urticaria within 10 minutes of vaccination. The health worker suspects anaphylaxis. What is the immediate management, including the drug, dose, route, and monitoring? What documentation and reporting is required?
- A grandfather brings his 3-year-old grandson for immunization. The parents are abroad. He states the parents have given him permission verbally. Can he provide consent for the child's vaccination? What is the ethical/legal framework applicable here?