Page 15 of 53
PE19.6 | Birth Injuries — SDL Guide
Learning Objectives
- Classify birth injuries by anatomical category: soft-tissue, bony, neural, and visceral
- Distinguish caput succedaneum, cephalhaematoma, and subgaleal haemorrhage on the basis of anatomy, onset, and clinical behaviour
- Identify the postural characteristics and root levels of Erb palsy (C5–C6) and Klumpke palsy (C8–T1)
- Outline the management approach for common birth injuries including clavicle fracture and brachial plexus palsy
- Recognise alert features of subgaleal haemorrhage that warrant urgent intervention
INSTRUCTIONS
Birth injuries are a significant cause of early neonatal morbidity. A systematic, anatomy-driven understanding of these injuries is essential for any clinician who will manage newborns — from the delivery room assessment to discharge counselling. Getting the caput/cephalhaematoma/subgaleal distinction wrong can result in missing a life-threatening haemorrhage; misidentifying Erb palsy can delay physiotherapy and worsen outcomes. This module gives you the factual and clinical foundation to assess, diagnose, and initiate management.
References
- Ghai Essential Pediatrics, 9th ed., Ch 8 — Newborn Infant (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 113 — Birth Injury (textbook)
- IAP Standard Treatment Guidelines — Neonatal Birth Injuries (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the intern on duty in the postnatal ward. A primigravida delivered after prolonged labour and difficult forceps extraction. The baby cries at birth, APGAR is 8 at 1 minute, 9 at 5 minutes. During the routine newborn examination you notice: a soft, boggy swelling on the right parietal region that seems to extend across the midline. The senior resident on the phone says 'is it a caput or a haematoma?' — and you realise you need to know the answer immediately because the management implications are completely different.
WHY THIS MATTERS
Birth injuries occur in approximately 2–7 per 1,000 live births and represent a spectrum from trivial bruising to life-threatening haemorrhage. In resource-limited settings where difficult instrumental deliveries and prolonged labours are more common, recognising birth injuries promptly saves lives. More importantly, these injuries are clinically distinguishable — a student who masters the anatomy can make the correct diagnosis at the bedside without imaging. Furthermore, incorrect counselling (telling a worried mother her baby's swelling is 'normal' when it is actually an enlarging subgaleal haematoma) can be fatal.
RECALL
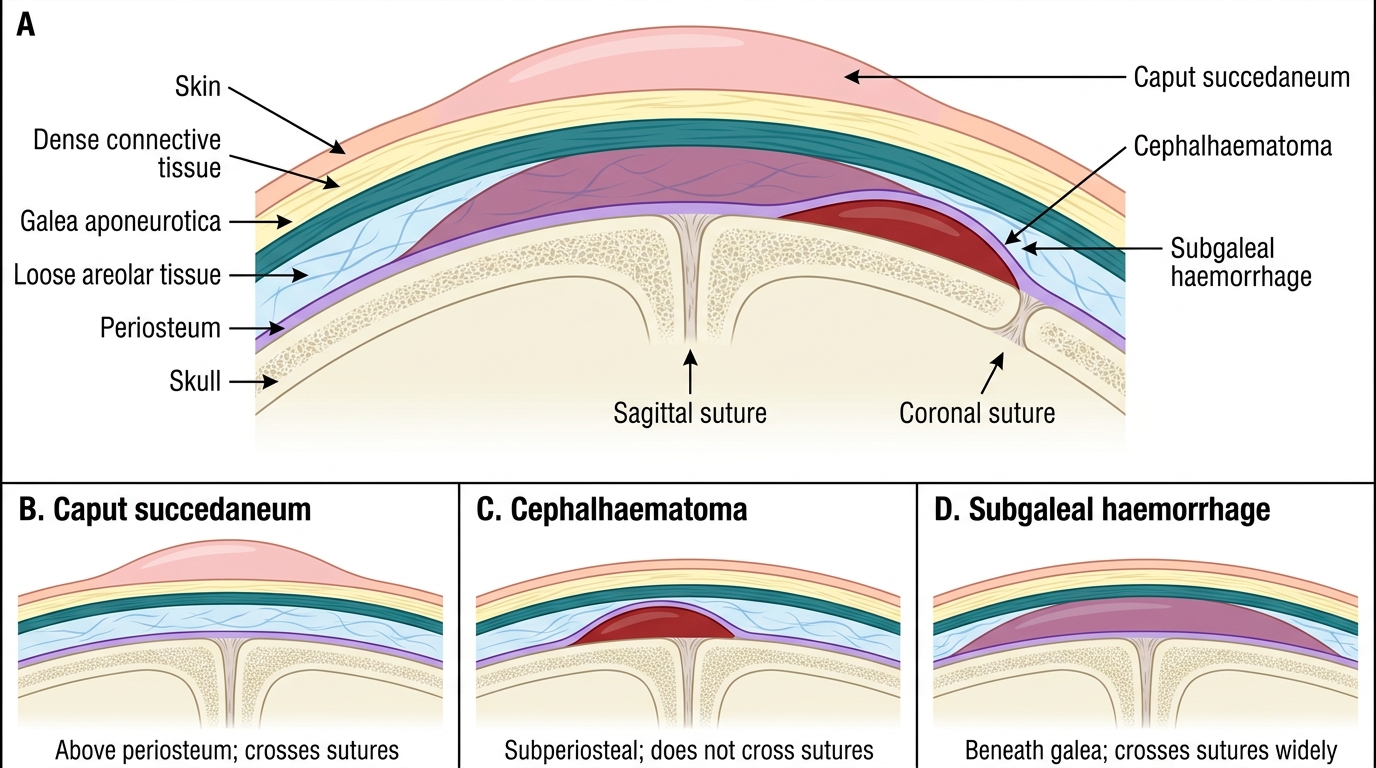
Before proceeding, recall the layered anatomy of the neonatal scalp from your anatomy course: the mnemonic SCALP — Skin → Connective tissue (dense subcutaneous) → Aponeurosis (galea aponeurotica) → Loose areolar tissue → Periosteum → bone. Each layer is relevant here. Recall also that individual skull bones are separated by suture lines (sagittal, coronal, lambdoid, metopic) and the fontanelles (anterior, posterior). From physiology, recall that a neonate's total blood volume is approximately 80–90 mL/kg, making even modest haemorrhage significant. From your paediatric arc foundation, recall that APGAR scores (0–2 each for heart rate, respiration, tone, reflex irritability, colour) assess the newborn at 1 and 5 minutes.
Clinical Presentation and Recognition of Birth Injuries
Birth injuries are physical injuries sustained by the neonate as a consequence of the mechanical forces of labour and delivery. They may be immediately obvious at birth or may evolve over hours to days. The astute clinician must perform a systematic neonatal examination looking specifically for signs that deviate from normal — not only to diagnose and treat, but to accurately document for medicolegal and parental communication purposes.
The classic presentation pattern depends on the injury type. Soft-tissue injuries manifest as visible swellings, bruising, or abrasions, most often over the presenting part. A scalp swelling following vertex delivery demands precise characterisation before a diagnosis is assigned. Nerve injuries typically present as asymmetric limb posture or movement — a baby who does not move one arm spontaneously, whose cry is asymmetric, or whose facial movements differ between sides requires brachial plexus or facial nerve assessment. Skeletal injuries often present as pseudo-paralysis (the infant avoids using a limb because it is painful) or may be discovered incidentally on examination. Visceral injuries are the most insidious — they often present with signs of internal haemorrhage (pallor, abdominal distension, cardiovascular instability) hours after delivery.
Risk factors for birth injury include: macrosomia (birth weight >4 kg), prolonged labour, instrumental delivery (forceps > vacuum), malpresentation (face, brow, breech), shoulder dystocia, and precipitate delivery. Identifying these antenatal and intrapartum risk factors prompts heightened post-delivery surveillance.
The systematic newborn examination should always include: assessment of symmetry of movement and tone in all four limbs, palpation of the clavicles (click or crepitus = fracture), inspection of scalp swellings (location, size, consistency, suture-crossing), assessment of facial symmetry during crying, and evaluation of the anterior fontanelle tension.
Soft-Tissue Birth Injuries: Caput, Cephalhaematoma, and Subgaleal Haemorrhage
These three scalp lesions are among the most commonly encountered birth injuries and are distinguished by their anatomical layer of origin — a distinction that has profound clinical implications. Understanding the anatomical basis is the key to correct diagnosis.
Caput succedaneum is an oedematous, diffuse soft-tissue swelling occurring in the subcutaneous layer, above the periosteum. It is caused by prolonged pressure on the presenting scalp against the cervix during a vertex presentation, or by vacuum-cup application. Because the subcutaneous layer is continuous across suture lines, caput crosses suture lines — this is the defining clinical feature. It is present at birth (not later), soft, pitting, and may have overlying petechiae or ecchymosis. It resolves spontaneously within 2–3 days without intervention and has no significant complications. No treatment is required.
Cephalhaematoma is a collection of blood in the subperiosteal space — between the periosteum and the outer surface of the skull bone. Because the periosteum is firmly adherent at suture edges, a cephalhaematoma is strictly limited by suture lines and cannot cross them. It is typically unilateral (right parietal most common), appears hours after birth (not immediately, because subperiosteal bleeding is slow), and is fluctuant and non-pitting. It may calcify if untreated and typically resolves over 6–8 weeks. Important complications include: neonatal hyperbilirubinaemia (as the haematoma reabsorbs, haem is degraded to bilirubin), and rarely associated linear skull fracture (in 5–20% of cases — do not aspirate routinely as this increases infection risk).
Subgaleal haemorrhage (subaponeurotic haemorrhage) is the most dangerous of the three. Blood collects in the loose areolar tissue beneath the galea aponeurotica, a potential space that extends from the orbital ridges anteriorly to the nuchal ridges posteriorly, and between the ears bilaterally. Because this space is entirely continuous, it crosses sutures widely and the entire scalp (and even behind the ears) may become a fluctuant boggy swelling. The critical danger is that this space can accommodate up to 260 mL — essentially the entire blood volume of a term neonate. Subgaleal haemorrhage most commonly follows vacuum delivery (3–4× increased risk vs forceps or spontaneous). The hallmark is a swelling that enlarges progressively after birth and may shift with repositioning (like a fluid wave). Alert signs include: pallor, tachycardia, bulging fontanelle, decreasing haematocrit. Management is urgent supportive care — blood transfusion, fluid resuscitation, phototherapy for jaundice. Mortality is approximately 12–14% in severe cases.
IMPORTED MEMORY CHECK — Three definitive distinguishing facts:
1. Caput: crosses sutures, present at birth, resolves in days.
2. Cephalhaematoma: does NOT cross sutures, appears hours later, resolves in weeks.
3. Subgaleal: crosses sutures widely, enlarges after birth, may be life-threatening.
Neonatal Scalp Swellings by Anatomical Plane
SELF-CHECK
A 2-day-old infant delivered by vacuum extraction has a soft, fluctuant swelling over the left parietal region that does NOT cross the sagittal suture. It was not present immediately after birth but was noticed at 6 hours of age. What is the most likely diagnosis?
A. Caput succedaneum
B. Cephalhaematoma
C. Subgaleal haemorrhage
D. Epidural haematoma
Reveal Answer
Answer: B. Cephalhaematoma
This is a cephalhaematoma: subperiosteal collection that does NOT cross suture lines (because periosteum is adherent at sutures), appears hours after birth (not immediately), and is fluctuant. Caput is present at birth and crosses sutures. Subgaleal haemorrhage crosses sutures widely and can be life-threatening. Epidural haematoma is intracranial and not a scalp swelling.
Nerve Injuries: Brachial Plexus Palsy and Facial Nerve Palsy
Birth-related nerve injuries are caused by traction, compression, or stretching of peripheral nerves during delivery. The brachial plexus and facial nerve are the most commonly affected.
Brachial plexus birth palsy (BPBP) results from excessive lateral traction on the neck during delivery, most commonly associated with shoulder dystocia or difficult traction in a vertex delivery, or traction on the trunk in a breech delivery. The brachial plexus (roots C5–T1) can be injured by stretching, avulsion, or rupture, with varying severity.
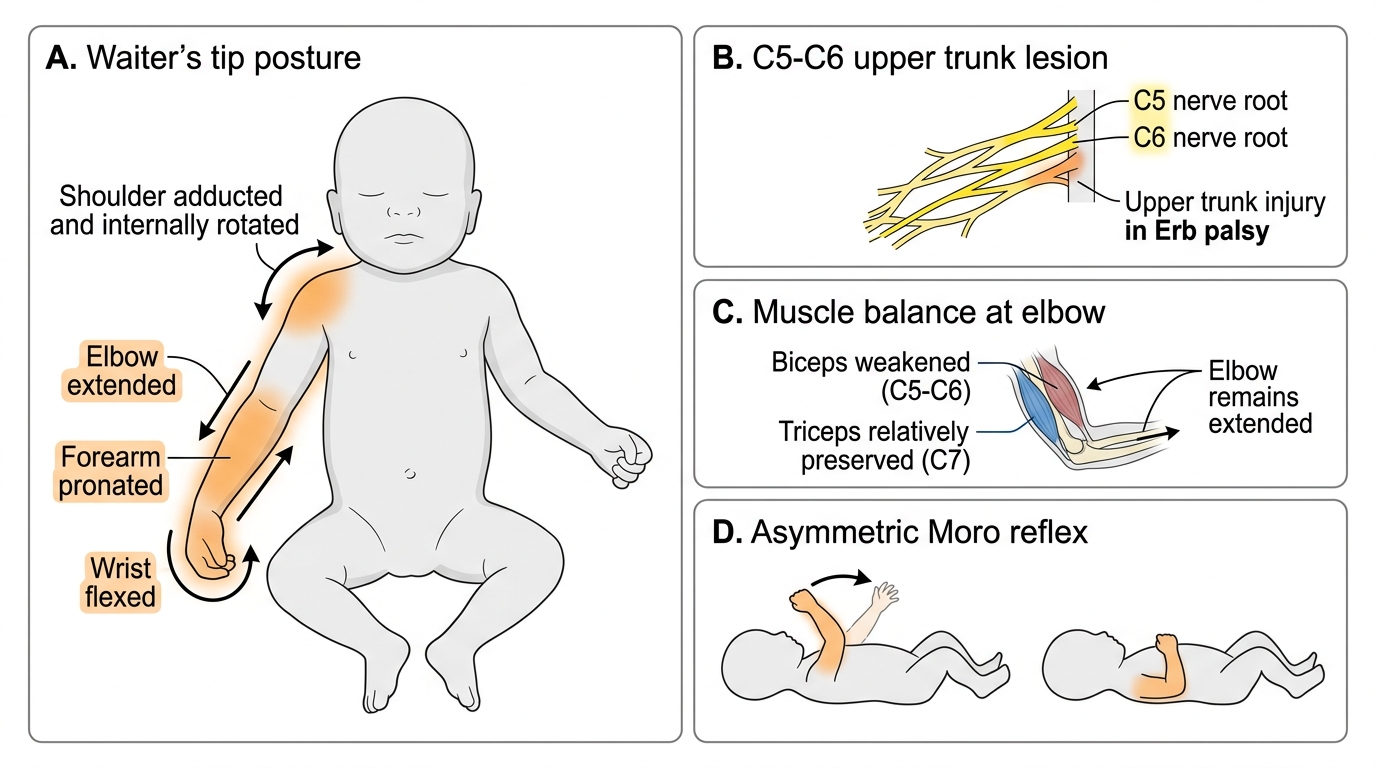
Erb palsy involves C5 and C6 roots (and sometimes C7). This is the most common pattern (~75% of BPBP). The mechanism is downward traction on the shoulder while the head is laterally flexed to the opposite side — as occurs in shoulder dystocia. The clinical appearance is characteristic and memorable: the infant holds the arm in 'waiter's tip' posture — the shoulder is adducted and internally rotated (deltoid and shoulder external rotators are paralysed), the elbow is extended (biceps, brachioradialis paralysed), the forearm is pronated (supinator paralysed), and the wrist is flexed (extensors from C7 reduced). The hand grasp is preserved if only C5–C6 are involved. Moro reflex is asymmetric — absent on the affected side.
Klumpke palsy involves C8 and T1 — the lower brachial plexus. This is far less common (~1%). It results from hyperabduction of the arm (e.g., traction on the arm in breech delivery). The clinical picture is a claw-hand deformity (intrinsic muscles of the hand paralysed, finger and wrist extensors preserved), with weakness of hand grip and finger flexion. When T1 is involved, Horner syndrome occurs on the ipsilateral side (ptosis, miosis, anhidrosis) because the sympathetic fibres to the eye travel via T1.
Total brachial plexus injury (C5–T1) produces a flaccid, anaesthetic, paralysed upper limb — this is the most severe form.
The natural history of Erb palsy is predominantly favourable: approximately 90% of cases recover spontaneously by 3–6 months with physiotherapy. Recovery is better when the injury is a neurapraxia (temporary conduction block without axonal disruption) rather than an axonotmesis or neurotmesis. Management consists of: splinting the arm across the abdomen initially (to protect the glenohumeral joint), gentle physiotherapy starting after a few weeks (passive range-of-motion exercises to prevent joint contracture), and parental counselling. Surgical intervention (nerve grafting) is considered if no recovery by 3–6 months.
Facial nerve palsy from birth injury is usually caused by compression of the facial nerve by forceps blades over the stylomastoid foramen, or by pressure from the sacral promontory in a prolonged labour. It presents as asymmetric facial movement during crying — the affected side does not move. The eye on the affected side may not close completely (lagophthalmos). Most cases are peripheral facial nerve palsy and resolve spontaneously within weeks. Eye protection (artificial tears, patching if poor closure) is important. The key distinction from central (upper motor neurone) facial palsy is that in peripheral palsy, the forehead and eye are also involved — in central palsy the forehead is spared.
Erb Palsy: Waiter's Tip Posture in a Neonate
CLINICAL PEARL
The 'waiter's tip' posture of Erb palsy (arm adducted, elbow extended, forearm pronated, wrist flexed) looks like a waiter holding their hand behind them to receive a tip — a vivid mnemonic. Critically, the biceps (C5-C6) is weakened while the triceps (C7) is relatively preserved, which is why the elbow stays extended. A useful bedside sign: the asymmetric Moro reflex. Lay the baby supine and allow the head to drop back slightly — the normal side abducts and extends in a 'startle', while the affected Erb arm barely moves. This test requires no equipment and can be done in the delivery room.