Page 16 of 53
PE19.6 | Birth Injuries — SDL Guide (Part 2)
Skeletal Birth Injuries: Clavicle, Long-Bone, and Skull Fractures
Skeletal injuries during birth result from traction and compressive forces applied to bones that, in a neonate, are more cartilaginous and compliant than at older ages. The most common is clavicle fracture, followed by long-bone fractures and skull fractures.
Clavicle fracture is the most common bone fractured during delivery and typically occurs during shoulder delivery in vertex presentation (especially in shoulder dystocia) or during arm extraction in breech delivery. The fracture is most often a greenstick fracture (incomplete) through the middle third of the clavicle. Clinical features: the baby may not move the arm on the affected side (pseudo-paralysis), there may be a palpable crepitus or step at the fracture site, the Moro reflex is asymmetric, and there may be tenderness. Importantly, many clavicle fractures are clinically silent and discovered only on routine examination or when callus formation is felt at 7–10 days. This is the reassuring lesion — prognosis is excellent with simple management: either no active treatment (for non-displaced fractures, allowing the mother to keep the arm comfortable) or pinning the sleeve of the garment to the body for 1–2 weeks.
Long-bone fractures — the humerus and femur can be fractured during breech delivery. They present as pseudo-paralysis, swelling, deformity, or pain on movement. X-ray confirms the diagnosis. Management involves splinting/immobilisation; healing in neonates is rapid (2–4 weeks).
Skull fractures — linear fractures are the most common, often associated with forceps application. Most are asymptomatic and require only observation. Depressed skull fractures (usually parietal, caused by firm pressure against the bony pelvis or forceps) present as a visible or palpable depression. If the fracture is associated with intracranial involvement or significant cosmetic deformity, neurosurgical consultation is required, but many depressed fractures in neonates elevate spontaneously.
Visceral injuries — although rare, liver, spleen, and adrenal haemorrhages can occur, particularly in macrosomic infants and difficult breech deliveries. These present as unexplained deterioration, pallor, abdominal distension, and haemodynamic instability in the first 48 hours. Adrenal haemorrhage may be bilateral and can lead to adrenal crisis. Imaging (abdominal USG) is diagnostic.
Diagnosis and Clinical Investigation of Birth Injuries
The diagnosis of most birth injuries is primarily clinical — a careful, systematic neonatal examination conducted within the first few hours of birth is the cornerstone. The clinical history (mode of delivery, risk factors, complications) directs the examination. Every newborn should undergo a structured head-to-toe assessment within 2–4 hours of delivery, with particular attention to the scalp, fontanelles, limb symmetry, clavicles, and primitive reflexes. The value of this systematic approach cannot be overstated: a missed cephalhaematoma may lead to unexpected jaundice at day 3–4; a missed subgaleal haemorrhage can be fatal within hours; an unrecognised clavicle fracture causes avoidable parental distress; and a delayed diagnosis of Erb palsy delays physiotherapy and may result in permanent contracture. The examination should always be documented carefully, noting size, location, and characteristics of any swelling, and the symmetry of all limb movements.
Provided image
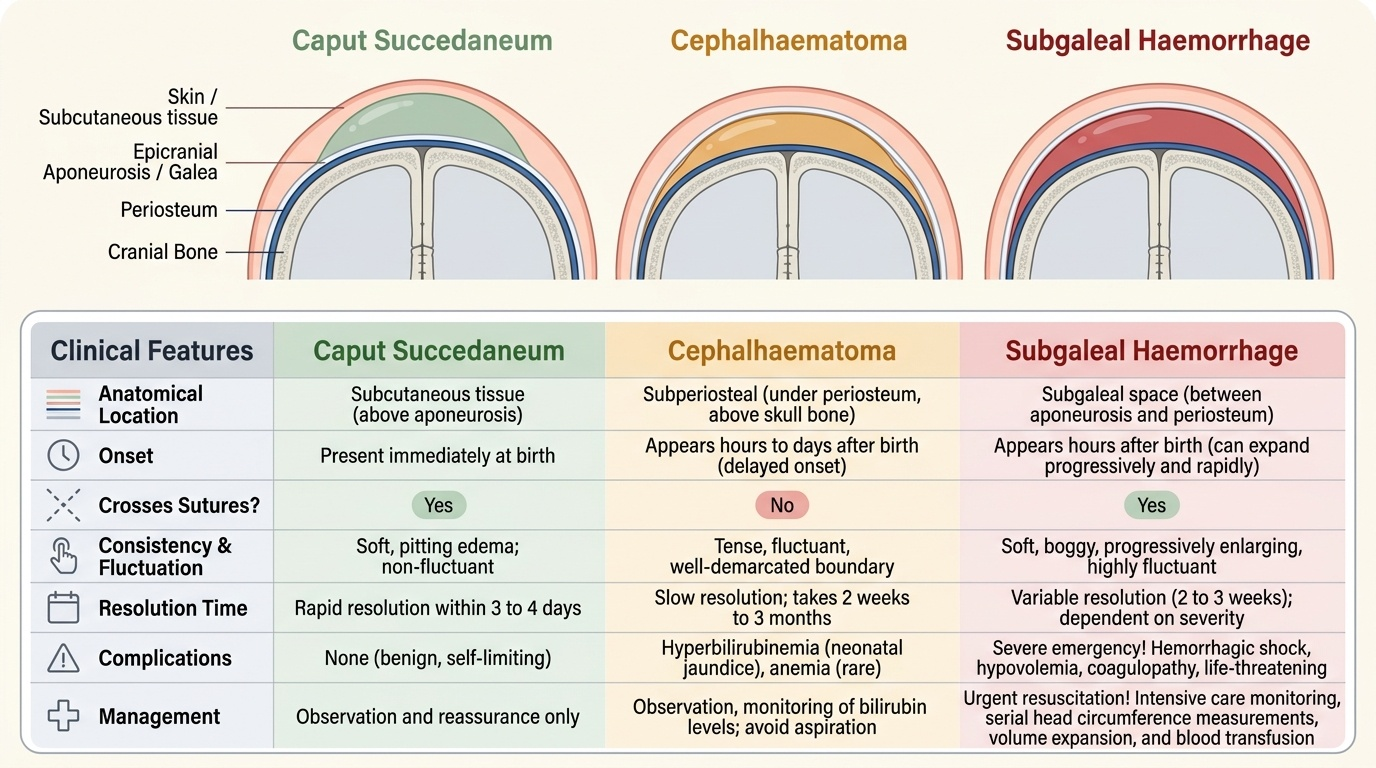
For scalp swellings, the key distinguishing features are assessed clinically. The examiner should palpate the entire scalp methodically, noting the distribution of any swelling relative to the underlying skull sutures — running a fingertip along the suture lines to determine whether the swelling stops at a suture (cephalhaematoma) or is continuous across it (caput or subgaleal). The consistency — pitting oedema versus fluctuant blood collection versus tense boggy swelling — and the temporal evolution (present at birth versus appearing hours later, or progressively enlarging) provide the most reliable clinical clues. A comparison of the three major scalp swellings is essential to master:
When a scalp swelling is present, assess: (1) does it cross suture lines — run a fingertip across the suspected suture; (2) was it present immediately after birth or did it appear later; (3) is it fluctuant (fluid) or oedematous (pitting); (4) is the baby pallor, tachycardic, or haemodynamically unstable. A worsening swelling that crosses sutures in a haemodynamically deteriorating baby is a subgaleal haemorrhage until proven otherwise.
Selecting the appropriate investigation requires clinical judgement. Most scalp swellings require no imaging. However, when there is haemodynamic instability, suspected intracranial involvement, or a fracture cannot be excluded clinically, targeted investigations are warranted. The principle is to use the least invasive investigation that answers the clinical question.
Imaging investigations:
- Skull X-ray: first line for suspected skull fracture (linear vs depressed). May show hairline fracture not palpable clinically.
- Cranial USG: non-invasive, performed bedside, evaluates intracranial haemorrhage (IVH, subdural, epidural) — complementary to clinical assessment.
- CT head: reserved for suspected intracranial injury, significant depressed fracture, or clinical deterioration.
- X-ray of limbs/clavicle: to confirm suspected fracture in pseudoparalysis.
- Abdominal USG: for suspected intra-abdominal haemorrhage (liver, spleen, adrenal).
- FBC, haematocrit, blood group and cross-match: in all cases of suspected significant haemorrhage (subgaleal, internal bleeding).
For nerve injuries: clinical examination with grading of active and passive movements, assessment of reflexes (Moro, grasp), and documentation of posture is usually sufficient for diagnosis and initial management. EMG/nerve conduction studies are used at 3–6 months to assess recovery and guide surgical decisions.
SELF-CHECK
An infant is delivered by difficult forceps after shoulder dystocia. At 4 hours of age, the parents notice the left side of the head 'keeps getting bigger.' On examination, there is a large soft boggy fluctuant swelling extending from above the left ear across the midline; the baby is pale and tachycardic. What is the immediate priority in management?
A. Request urgent skull X-ray to rule out fracture
B. Reassure parents that this is a normal caput succedaneum
C. Initiate urgent resuscitation with IV fluids and blood transfusion
D. Apply gentle pressure to the swelling to limit its extent
Reveal Answer
Answer: C. Initiate urgent resuscitation with IV fluids and blood transfusion
This presentation is a subgaleal haemorrhage — a swelling that crosses sutures, enlarges progressively, and is associated with haemodynamic instability (pallor, tachycardia). The subgaleal space can accommodate the entire neonatal blood volume (up to 260 mL), making this a life-threatening emergency. Immediate resuscitation with IV fluids and packed red cell transfusion is the priority. Skull X-ray is secondary. Applying pressure is ineffective and potentially harmful. Calling this a caput (present at birth, crosses sutures but small, haemodynamically stable) would be a fatal error.
Management of Specific Birth Injuries
Most birth injuries are managed conservatively with excellent prognosis. The specific management depends on the injury type and severity.
The general principle governing management of birth injuries is to match the intervention intensity to the severity of the injury. The great majority of birth injuries are self-limiting: they resolve with careful observation, parental reassurance, and, where needed, analgesia or positional care. Active intervention is reserved for injuries that threaten function (nerve palsy requiring physiotherapy), haemodynamic stability (subgaleal haemorrhage requiring resuscitation), or vital structures (eye in facial palsy). The following injury-specific approaches reflect current paediatric practice and IAP guidelines.
Caput succedaneum: Requires no treatment. Spontaneous resolution within 2–3 days. Parental reassurance is key.
Cephalhaematoma: Usually no active treatment needed. Avoid aspiration (risk of infection and introduction of bacteria into a closed subperiosteal space). Monitor for hyperbilirubinaemia (reabsorption of blood → jaundice; phototherapy may be needed). Calcification may occur but does not require intervention. Resolution by 6–8 weeks.
Subgaleal haemorrhage: This is the emergency. Key management steps:
1. Continuous monitoring of vital signs, head circumference (serial measurements).
2. IV fluid resuscitation (normal saline 10–20 mL/kg boluses for haemodynamic instability).
3. Blood transfusion (packed red cells) for anaemia or haemodynamic shock — aim haematocrit >35%.
4. Vitamin K administration (if not yet given at birth — haemorrhagic disease of the newborn can co-exist).
5. Phototherapy for hyperbilirubinaemia.
6. NICU admission for monitoring.
Clavicle fracture: For non-displaced fractures, no active immobilisation is required — gentle handling and dressing the baby normally is sufficient. For displaced or complete fractures, pin the sleeve to the body of the garment for 1–2 weeks. Excellent prognosis with complete healing. Instruct parents on gentle handling.
Brachial plexus palsy (Erb palsy):
- Initial: position the arm across the abdomen to protect the glenohumeral joint (not traditional wrist splint in waiter's tip — that position is the injury position).
- Begin passive physiotherapy at 2–3 weeks: gentle passive range-of-motion exercises, especially shoulder external rotation and supination, to prevent contracture.
- Parental counselling: ~90% recover by 3–6 months; encourage continued physiotherapy.
- If no recovery by 3–6 months: refer to paediatric neurosurgery/orthopaedics for consideration of nerve grafting or neurolysis.
Facial nerve palsy: Protect the eye (artificial tears every 2–4 hours, patch if lagophthalmos is significant). Most recover within weeks to months.
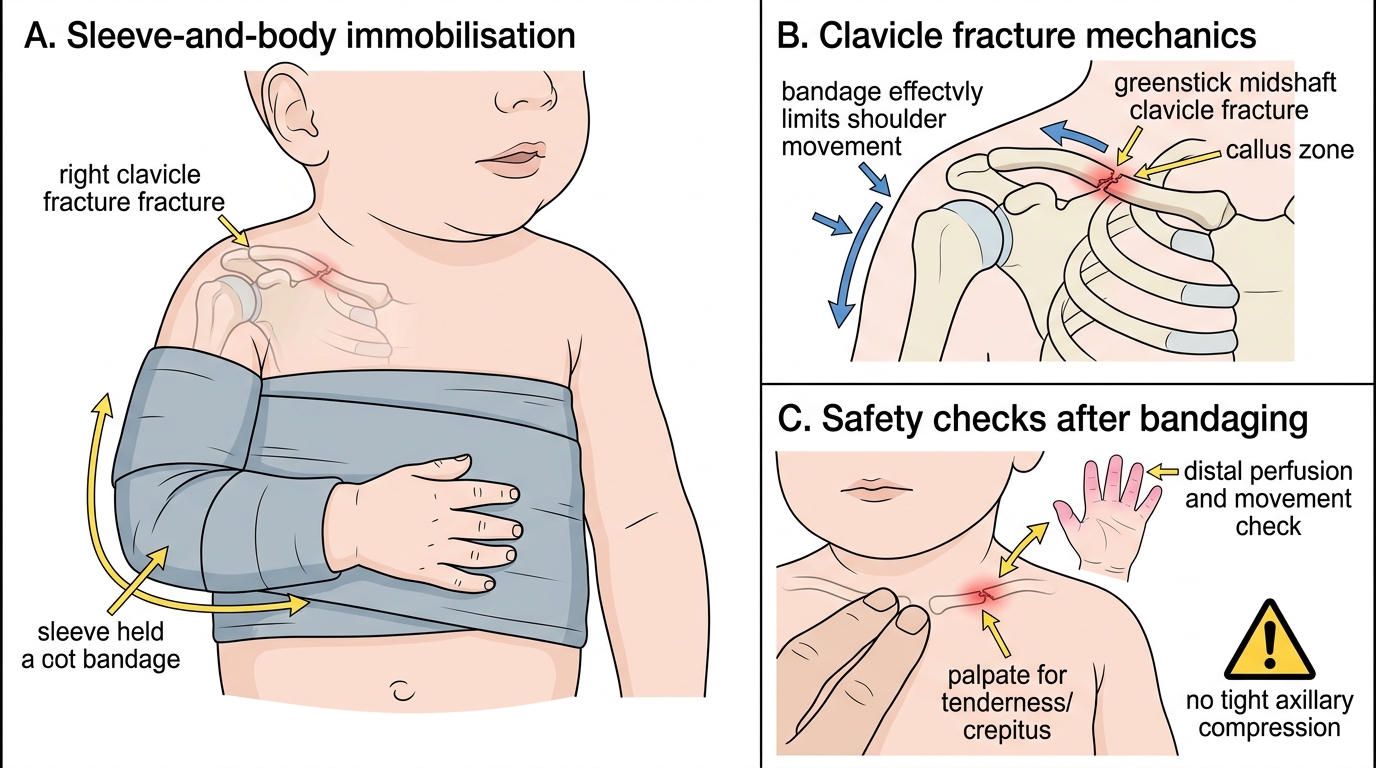
Sleeve-and-Body Bandage for Neonatal Clavicle Fracture
SELF-CHECK
In Erb palsy, which nerve roots are primarily involved, and what is the characteristic posture?
A. C5-C6; arm abducted, elbow flexed, forearm supinated — 'waiter giving a tip' posture
B. C5-C6; arm adducted, elbow extended, forearm pronated, wrist flexed — 'waiter's tip' posture
C. C8-T1; claw hand with Horner syndrome
D. C7; wrist drop with preserved hand grip
Reveal Answer
Answer: B. C5-C6; arm adducted, elbow extended, forearm pronated, wrist flexed — 'waiter's tip' posture
Erb palsy involves C5 and C6. The 'waiter's tip' posture (NOT 'waiter giving a tip') describes the arm in adduction and internal rotation at the shoulder (deltoid, external rotators paralysed), elbow extended (biceps/brachioradialis paralysed from C5-C6), forearm pronated (supinator from C6 lost), wrist flexed. The hand grasp is preserved (C8-T1 are intact). Option C describes Klumpke palsy (C8-T1). Option D describes radial nerve injury.
Self-Assessment: Putting It Together
Use the following integrative questions to check your understanding of the key clinical distinctions and management decisions in birth injuries. Apply the anatomy-first approach to each scenario.
The three cases below are structured to test your ability to apply the anatomy-first diagnostic framework to real clinical presentations. For each case, read the clinical scenario, identify the key distinguishing features in the history and examination, reach a diagnosis, and outline the initial management. These cases reflect the type of clinical decision-making you will encounter in the delivery suite and postnatal ward. Resist the temptation to look up the answers before working through the reasoning — the value of self-assessment lies in identifying your own knowledge gaps before an examination or clinical encounter does it for you.
Case 1: A 3.9 kg baby is born by spontaneous vaginal delivery with a prolonged second stage. The vertex was the presenting part. At birth, you note a soft, non-pitting swelling over the right parietal and temporal regions that clearly extends across the sagittal suture. The baby is active and well. This swelling was present immediately after birth and is not growing.
- What is the diagnosis? (caput succedaneum — crosses sutures, present at birth, non-pitting, infant well)
- What investigation does it require? (none)
- What should you tell the parents? (will resolve spontaneously in 2–3 days, normal after a head-down delivery)
Case 2: At the 6-hour check, you notice a baby delivered by forceps has an asymmetric Moro reflex — the left arm barely extends. On inspection, the left arm hangs with the shoulder adducted, elbow extended, and forearm pronated. The hand grip appears intact.
- What nerve roots are affected? (C5-C6 — Erb palsy)
- What is the immediate management? (position arm across abdomen; plan physiotherapy at 2–3 weeks; counsel parents on ~90% spontaneous recovery)
- When would you consider surgical referral? (no recovery by 3–6 months)
Case 3: A macrosomic baby (4.2 kg) is delivered by vacuum after prolonged labour. At 2 hours, the nurse calls you because 'the swelling on the head keeps getting bigger.' The baby is pale, heart rate is 180 bpm, the swelling extends bilaterally across the midline.
- What is the diagnosis? (subgaleal haemorrhage — expanding, crosses sutures, haemodynamically unstable)
- What is the immediate management? (IV fluids + blood transfusion + NICU + serial head circumference + FBC/cross-match)
- Why is this dangerous? (subgaleal space can accommodate entire neonatal blood volume ~260 mL)