Page 21 of 53
PE19.8 | Low Birth Weight — SDL Guide
Learning Objectives
- Define Low Birth Weight (LBW) and classify neonates as preterm, SGA, or both
- Describe the physical features that distinguish a preterm neonate from an SGA/IUGR neonate
- List the acute and long-term complications of LBW and their pathophysiological basis
- Outline the immediate management of a stable LBW neonate including Kangaroo Mother Care (KMC)
- Identify the major maternal, placental, and fetal causes of LBW relevant to the Indian context
INSTRUCTIONS
Low Birth Weight is the single most powerful predictor of neonatal mortality and morbidity in India. With approximately 18–20% of Indian births weighing <2500 g (NFHS-5), LBW is not a rare specialised condition — it is the everyday reality of neonatal wards across the country. Understanding whether an LBW infant is preterm or SGA/IUGR is not academic: these are different conditions with different pathophysiology, different complications, and different management priorities. Kangaroo Mother Care — a simple, free, evidence-based intervention — reduces mortality in LBW infants and every clinician in India should be able to counsel a mother on how to do it.
References
- Ghai Essential Pediatrics, 9th ed., Ch 8 — Newborn Infant and Ch 22 — The Premature Infant (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 116 — The High-Risk Infant (textbook)
- WHO Guidelines on Kangaroo Mother Care: A Care Practice That Protects, Promotes and Supports Breastfeeding (2003); IAP NNF Guidelines on LBW Management (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the duty intern in the neonatal ward. A midwife hands you two infants born within an hour of each other. Both weigh 1900 g. Infant A, born at 32 weeks by emergency caesarean for maternal pre-eclampsia, is pink, breathing fast, and has translucent skin with visible vessels. Infant B, born at 38 weeks to a malnourished mother who smoked throughout pregnancy, is alert and crying but has loose wrinkled skin, a relatively large head, and is stained with meconium. Both are LBW — but they are not the same patient. Understanding why these two infants are different, what makes each dangerous, and how to manage them is the central learning objective of this module.
WHY THIS MATTERS
India carries the world's largest burden of LBW neonates — an estimated 7–8 million annually. LBW is the single most powerful predictor of neonatal mortality: LBW neonates account for disproportionately high fractions of all neonatal deaths. The Barker hypothesis additionally links intrauterine growth restriction to adult-onset hypertension, coronary artery disease, and type 2 diabetes — making LBW a condition with lifelong consequence. Practical relevance for you as a clinician: every facility delivery in India involves neonatal weight measurement and a clinical decision about management. The ability to assess gestational age, plot weight on a growth chart, identify the at-risk infant, initiate KMC, and counsel on feeding will determine outcomes for thousands of patients in your career.
RECALL
From neonatal basics, recall that normal birth weight for a term Indian neonate is approximately 2.8–3.2 kg; the WHO threshold for LBW is <2500 g regardless of gestational age. Recall from your obstetrics arc that gestational age is counted from the first day of the last menstrual period and is normally 37–42 weeks; below 37 weeks is preterm. Recall from physiology that surfactant (dipalmitoylphosphatidylcholine) is produced by type II pneumocytes and lines alveoli to prevent collapse — it reaches adequate levels only after 34–35 weeks of gestation, explaining why extremely preterm infants develop Respiratory Distress Syndrome (RDS). From the NIS, recall that BCG, OPV-0, and Hepatitis B are given at birth even to LBW neonates if clinically stable. Recall from the Vitamin K module that LBW neonates (<1.5 kg) receive 0.5 mg IM Vitamin K at birth.
Clinical Presentation: Recognising the LBW Newborn
Clinical recognition of an LBW neonate and determination of whether the low weight reflects prematurity (preterm birth) or growth restriction (SGA/IUGR in a term or near-term infant) is the first and most important clinical step, because the two mechanisms produce different physical appearances, different complications, and different management priorities. Both can co-exist — a preterm infant can also be growth-restricted. The bedside examination within the first 2 hours provides sufficient information to distinguish these two groups in most cases, using a combination of gestational age assessment (Ballard Score) and careful inspection of the physical features that reflect either organ immaturity (preterm) or chronic fetal undernutrition (IUGR). Understanding these differences before opening any investigation is the hallmark of competent neonatal clinical care.
Provided image
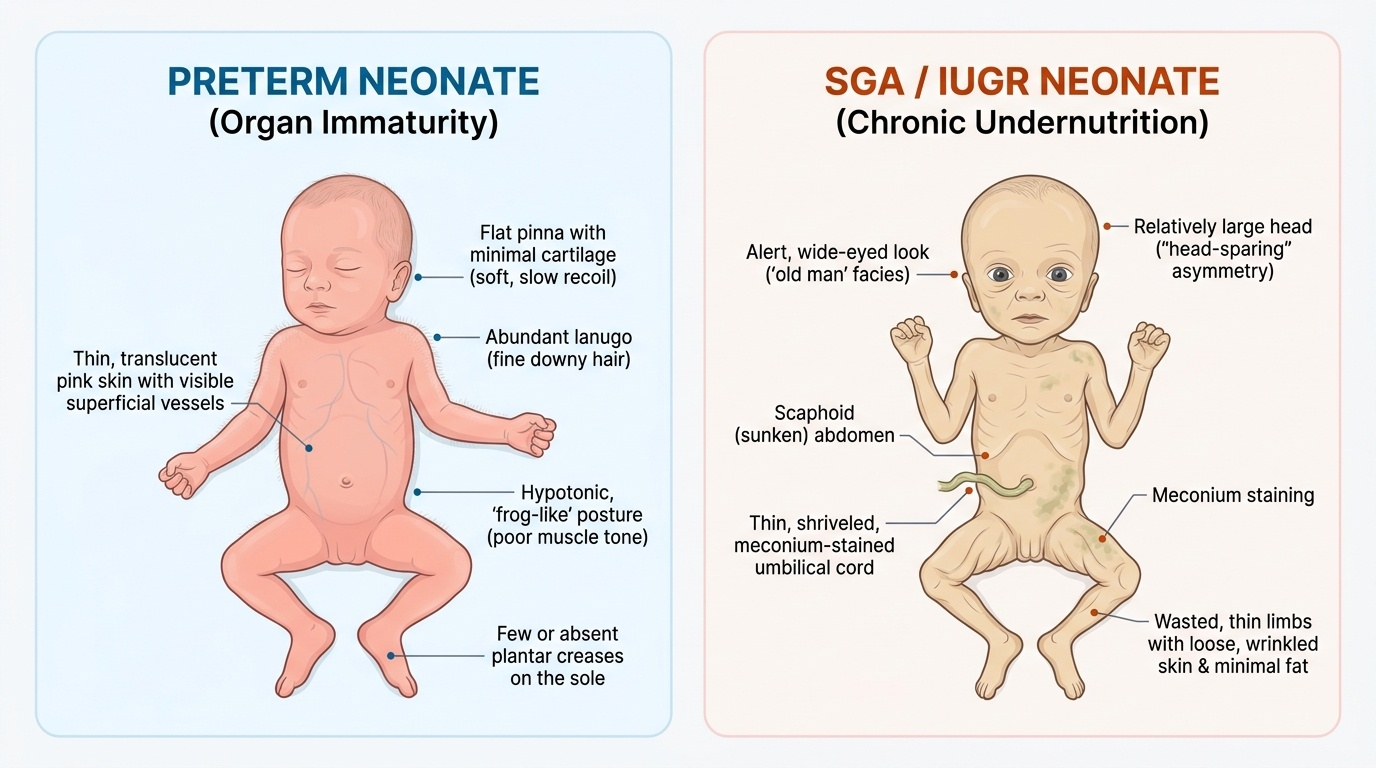
Physical features of a preterm neonate (born <37 weeks) reflect organ immaturity:
- Skin: translucent, thin, red/pink, with visible superficial blood vessels; abundant lanugo (fine downy hair over body)
- Ears: soft, flat pinna with little cartilage (early preterm) progressing to defined cartilage with elastic recoil (>32 weeks)
- Posture: hypotonic, frog-like posture (extension of all limbs due to immature muscle tone)
- Genitalia: undescended testes in males; labia majora do not fully cover labia minora in females
- Sole creases: few or absent at very early gestations; progressing to full-foot creasing at term
- Neurological tone: immature reflexes, weak grasp and suck, poor coordination of suck-swallow-breathe
Physical features of an SGA/IUGR neonate (birth weight <10th percentile, often near-term or term gestational age) reflect chronic undernutrition in utero:
- Skin: loose, dry, wrinkled, meconium-stained (chronic fetal distress), scaphoid abdomen
- Head: relatively large for body size (head-sparing in asymmetric IUGR) with wide fontanelles
- Limbs and buttocks: wasted, thin, minimal subcutaneous fat — 'old man' facies with alert expression
- Cord: thin, meconium-stained in severe cases
- Alertness: surprisingly alert and hungry (brain development relatively preserved in asymmetric IUGR)
Gestational age assessment: the Ballard Score (modified) is the standard clinical tool, evaluating 6 neuromuscular criteria (posture, square window angle, arm recoil, popliteal angle, scarf sign, heel-to-ear) and 6 physical criteria (skin, lanugo, plantar creases, breast, eye/ear, genitalia), each scored 0–5. Total score correlates with gestational age. This is distinct from APGAR (resuscitation score) and Silverman-Anderson (respiratory distress score) — do not confuse these three scoring systems.
Pathophysiology: Preterm Immaturity vs IUGR Mechanisms
The pathophysiology of LBW differs fundamentally between preterm birth and IUGR/SGA — a distinction that explains why these two groups face different clinical complications and require different management strategies. In preterm birth, the problem is organ immaturity: all physiological systems (pulmonary, neurological, gastrointestinal, haematological, immunological, metabolic, and thermal) are incompletely developed relative to the demands of extrauterine life. In IUGR/SGA, the problem is chronic undernutrition with preserved (and sometimes enhanced) maturation: the brain has been protected by preferential blood flow redistribution at the expense of the liver, gut, and musculoskeletal system, but the metabolic reserves are critically depleted. Distinguishing these mechanisms predicts the complications the clinician must anticipate.
Preterm immaturity means incomplete development of organ systems that are normally completed in the third trimester. The consequences are predictable from anatomy and physiology:
- Pulmonary immaturity: surfactant deficiency → alveolar collapse → Respiratory Distress Syndrome (RDS) — the leading cause of early neonatal death in preterm infants
- Brain vulnerability: the germinal matrix (a highly vascular region lining the lateral ventricles) is fragile and present only until ~32–34 weeks; fluctuations in cerebral blood flow cause intraventricular haemorrhage (IVH) — a major cause of neurodevelopmental disability
- Gut immaturity: immature intestinal mucosal barrier + microbial colonisation + formula feeding → necrotising enterocolitis (NEC) — potentially fatal gut necrosis
- Retinal vasculature incompleteness: at birth, retinal vascularisation is incomplete; post-birth oxygen therapy (unmonitored hyperoxia) can cause abnormal vascularisation → retinopathy of prematurity (ROP)
- Thermoregulation: reduced subcutaneous fat + large surface area: body volume ratio + immature thermogenesis → rapid hypothermia
- Metabolic: limited glycogen stores + high metabolic demands → hypoglycaemia within hours of birth
- Apnoea of prematurity: immature respiratory control (brainstem) → episodes of respiratory pause >20 seconds with bradycardia
IUGR pathophysiology — asymmetric vs symmetric IUGR:
The timing and nature of the growth-restricting insult determines the pattern:
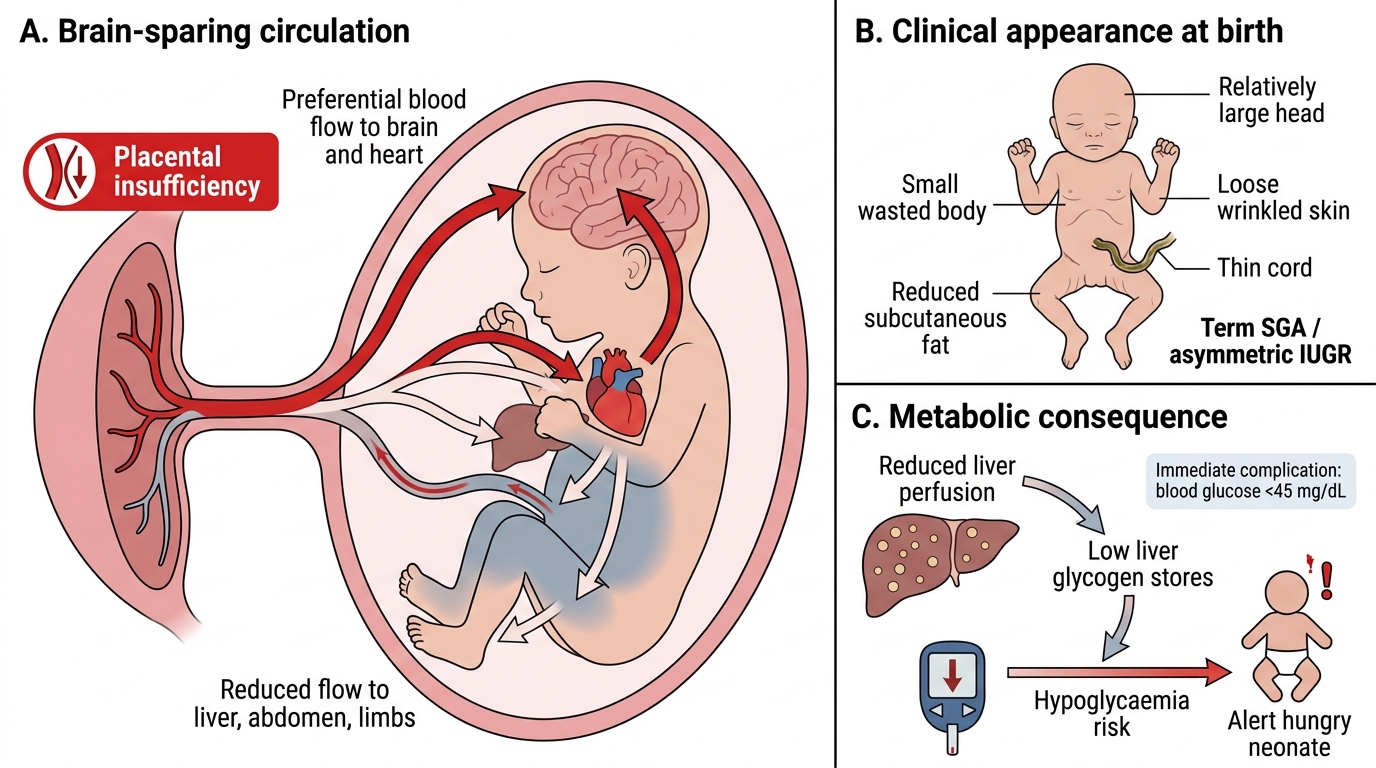
- Asymmetric IUGR (late-onset, placental insufficiency): reduction in uterine blood flow in the third trimester → fetus prioritises blood flow to brain and heart (brain-sparing) at the expense of liver, abdominal viscera, and limbs → head is relatively large, abdomen is small and scaphoid, liver glycogen stores are depleted → hypoglycaemia is the most immediate danger; ponderal index (PI = weight in g × 100 / length in cm³) is low (wasted).
- Symmetric IUGR (early-onset insult): chromosomal abnormalities, congenital TORCH infections (cytomegalovirus, rubella, toxoplasma), severe maternal malnutrition, radiation — affecting all organs proportionately from early in gestation → head AND body are small, PI is normal, prognosis is worse because brain development is also compromised.
IMPORTANT: asymmetric IUGR = brain-sparing = alert but hypoglycaemic; symmetric IUGR = all-reduced = possible chromosomal/infectious cause, poor neurodevelopmental prognosis.
Brain-Sparing in Asymmetric IUGR
SELF-CHECK
A 38-week neonate weighs 1800 g at birth. The infant is alert, has loose wrinkled skin with a relatively large head, thin meconium-stained cord, and is very hungry. How would you classify this infant, and what is the most immediate metabolic complication to anticipate?
A. Preterm infant with respiratory distress syndrome (RDS)
B. SGA/asymmetric IUGR term infant with risk of hypoglycaemia
C. SGA/symmetric IUGR infant with chromosomal abnormality
D. Normal-for-gestational-age preterm infant
Reveal Answer
Answer: B. SGA/asymmetric IUGR term infant with risk of hypoglycaemia
This is a term (38 weeks) infant with birth weight <2500 g and weight <10th percentile for gestational age = SGA. The clinical features (loose wrinkled skin, relatively large head, thin cord, alertness, extreme hunger) are classic for asymmetric IUGR — brain-sparing pattern where liver glycogen stores are depleted. The most immediate metabolic risk is hypoglycaemia (blood glucose <45 mg/dL). RDS is a preterm complication (surfactant deficiency). Symmetric IUGR presents with proportional reduction of all compartments. This infant is term, not preterm.
Aetiology of LBW: Fetal, Placental, and Maternal Causes
LBW has a complex, multifactorial aetiology that is best understood through a systematic categorisation into fetal, placental, and maternal factors. In clinical practice, identifying the likely cause determines both immediate management and counselling for recurrence prevention. In the Indian context, maternal nutritional and socioeconomic factors dominate the aetiology of IUGR, while preterm birth is driven by a combination of infections, uterine/cervical factors, and iatrogenic prematurity. A useful framework distinguishes whether the growth restriction originated from a problem with the fetus itself (chromosomal, infectious), the placenta (insufficiency, structural), or the mother (nutritional, hypertensive, toxic). Each category carries different implications for investigation of the affected newborn and for antenatal counselling in subsequent pregnancies. In clinical practice, the aetiology workup is guided by the pattern of growth restriction (symmetric vs asymmetric) and the presence of dysmorphic features or organomegaly.
Provided image
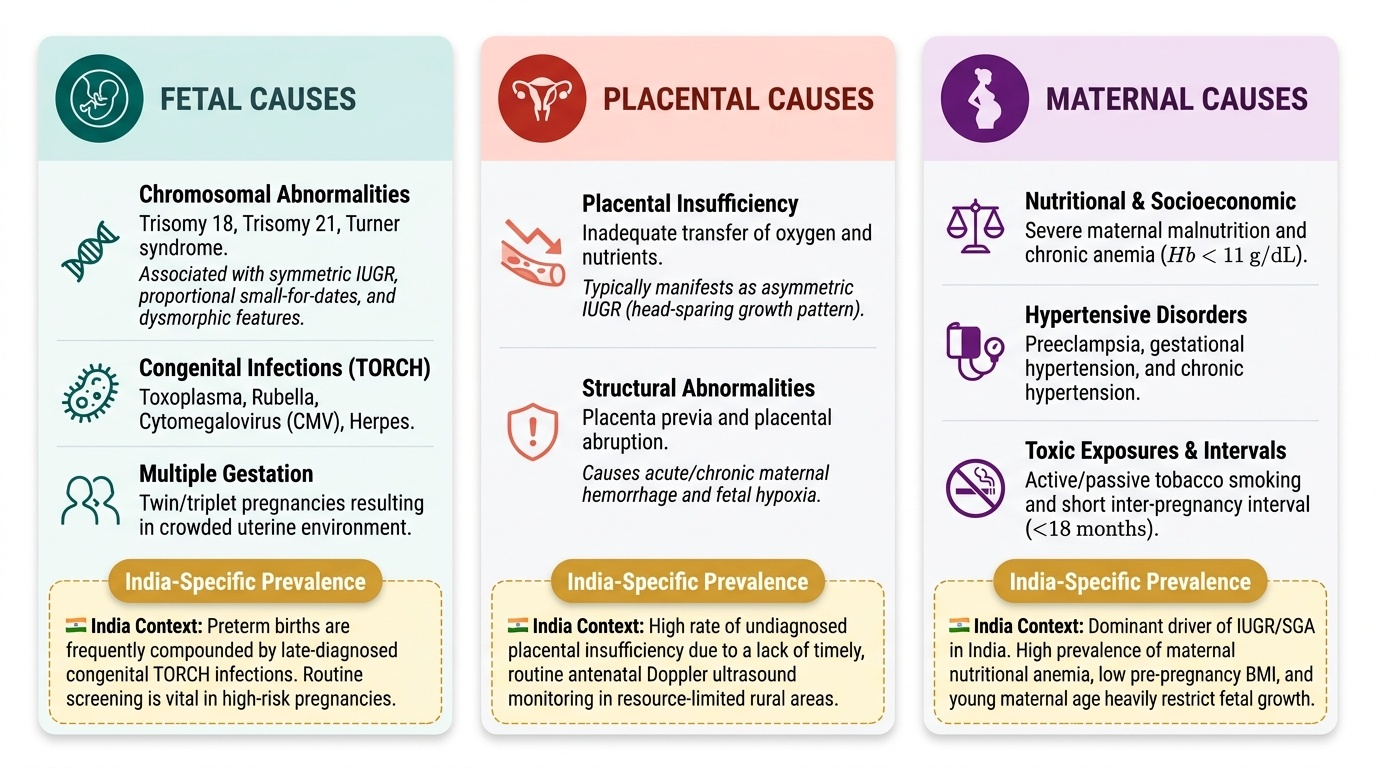
Fetal causes of IUGR/SGA:
- Chromosomal abnormalities: trisomy 18, trisomy 21, Turner syndrome — symmetric IUGR, proportional small-for-dates, associated dysmorphic features
- Congenital infections (TORCH): Toxoplasma, Rubella, Cytomegalovirus (CMV), Herpes — symmetric IUGR, hepatosplenomegaly, intracranial calcifications (CMV/Toxoplasma), cataracts (rubella)
- Multiple gestation: twins, triplets — twin-to-twin transfusion syndrome, shared placenta, uterine overcrowding
- Congenital malformations: cardiac defects, renal agenesis
Placental causes:
- Placental insufficiency (most common cause of asymmetric IUGR): hypertension, pre-eclampsia, thrombophilias, antiphospholipid syndrome → reduced uteroplacental blood flow → asymmetric brain-sparing pattern
- Placenta praevia, placental abruption: reduced effective placental area
- Circumvallate placenta, velamentous cord insertion: structural anomalies reducing placental efficiency
Maternal causes (dominant in India):
- Hypertensive disorders of pregnancy: pre-eclampsia and chronic hypertension are the most important modifiable risk factors for IUGR (both via placental insufficiency)
- Maternal anaemia (Hb <7 g/dL): oxygen carrying reduced → fetal hypoxia → IUGR; India has one of the highest rates of gestational anaemia globally
- Maternal malnutrition: low pre-pregnancy weight (BMI <18.5), inadequate gestational weight gain — very common in rural India
- Tobacco smoking and alcohol: direct fetal toxins causing vasoconstriction and teratogenicity
- Short inter-pregnancy interval (<18 months): maternal nutritional depletion
- Maternal age extremes: teenage pregnancies and older mothers (>35 years)
- Urogenital infections: bacterial vaginosis, Group B Streptococcus, UTIs → ascending infection → preterm labour
- Uterine structural abnormalities: uterine septum, fibroids, incompetent cervix → preterm delivery
Iatrogenic prematurity: elective caesarean or induction before 37 weeks for maternal/fetal indications (pre-eclampsia, placenta praevia) — contributes to late preterm LBW burden.
CLINICAL PEARL
In India, maternal anaemia is a major contributor to LBW — a connection that makes the routine prescription of iron-folic acid (IFA) tablets in antenatal care a LBW prevention intervention, not just a maternal health measure. The fetal consequences of severe maternal anaemia (Hb <7 g/dL) include reduced oxygen delivery to the fetoplacental unit and asymmetric IUGR via relative fetal hypoxia. The policy lesson: for every 10% reduction in prevalence of severe maternal anaemia, a measurable reduction in LBW rates has been observed in Indian cohort data. Teaching this causal chain — maternal IFA supplementation → correction of anaemia → improved fetoplacental oxygen delivery → improved birth weight — makes preventive interventions comprehensible rather than merely prescribed.