Page 22 of 53
PE19.8 | Low Birth Weight — SDL Guide (Part 2)
Complications of LBW: Acute and Long-term
LBW neonates face a predictable cascade of complications that correlates with the degree of prematurity and growth restriction. Understanding which complications occur in which group (preterm vs SGA) and their pathophysiological basis enables anticipatory management — addressing problems before they become crises. The cardinal principles are: (1) complications are predictable from the pathophysiology; (2) early recognition before symptoms become severe dramatically improves outcomes; and (3) certain complications are specific to prematurity (RDS, IVH, NEC, ROP), others to growth restriction (hypoglycaemia from depleted liver glycogen), and some affect all LBW infants (hypothermia, sepsis, feeding difficulties, jaundice). Knowing which group is at risk for which complication converts this seemingly long list into a clinically actionable and manageable framework.
Immediate complications (first hours to days):
- Hypothermia: occurs in both preterm and SGA due to thin skin, poor subcutaneous insulation, and large surface-area-to-volume ratio. Preterm infants are additionally unable to shiver or increase brown-fat thermogenesis adequately. Core temperature <36.5°C defines hypothermia; moderate hypothermia (<35.5°C) causes metabolic acidosis, hypoglycaemia, pulmonary hypertension, and apnoea.
- Hypoglycaemia: occurs within first 1–3 hours, especially in SGA infants (depleted liver glycogen) and preterm infants (high metabolic demands, small glycogen stores). Blood glucose <45 mg/dL (2.5 mmol/L) requires treatment. Severe or unrecognised neonatal hypoglycaemia causes permanent brain injury.
- Respiratory Distress Syndrome (RDS) (primarily preterm <34 weeks): surfactant deficiency → atelectasis → respiratory distress (tachypnoea, grunting, subcostal retractions, cyanosis). Treated with surfactant replacement therapy (intratracheal) and CPAP/mechanical ventilation.
- Jaundice: LBW neonates (especially preterm) have immature hepatic conjugation → physiological jaundice appears earlier, peaks higher, and persists longer than in term neonates. Cephalhaematoma (from birth injury) worsens jaundice. Monitor serum bilirubin and initiate phototherapy at lower thresholds in preterm/LBW infants.
- Sepsis: immature immune defences (reduced immunoglobulins, complement, neutrophil function), multiple procedures, central lines → early-onset (GBS, E. coli) and late-onset (nosocomial — Staphylococcus, Klebsiella) sepsis.
- Feeding difficulties: poor suck-swallow-breathe coordination (preterm); unable to coordinate oral feeds until ~34 weeks gestation; requires nasogastric or orogastric feeds with expressed breast milk.
Specific complications of prematurity:
- Intraventricular haemorrhage (IVH): bleeding into the germinal matrix and lateral ventricles; classified Grades I–IV (Papile); Grade III–IV associated with hydrocephalus and neurodevelopmental disability.
- Necrotising Enterocolitis (NEC): intestinal ischaemia-necrosis in preterm gut; presents at 2–3 weeks with abdominal distension, blood in stools, deterioration; managed medically (bowel rest, antibiotics, TPN) or surgically.
- Retinopathy of Prematurity (ROP): unregulated VEGF-driven abnormal retinal vascularisation, especially with unmonitored oxygen therapy in <32 weeks; screened by ophthalmologist at 4–6 weeks.
- Apnoea of prematurity: respiratory pause >20 seconds or any pause with bradycardia/desaturation; treated with methylxanthines (caffeine citrate — first line, safe, effective).
- Patent Ductus Arteriosus (PDA): failure of ductal closure due to prostaglandin excess and reduced oxygen sensitivity in preterm; causes left-to-right shunt → pulmonary oedema; treated with ibuprofen or indomethacin (COX inhibitors) or surgical ligation.
Long-term sequelae:
- Neurodevelopmental disability: cerebral palsy (especially after IVH Grade III–IV), intellectual disability, autism spectrum disorder — risk increasing with decreasing gestational age.
- Stunting and wasting: IUGR infants who do not achieve catch-up growth by 2 years have increased risk of permanent short stature.
- Barker hypothesis / Developmental Origins of Health and Disease (DOHaD): intrauterine undernutrition programmes the fetus metabolically for a nutrient-poor environment; post-natal exposure to adequate or excess nutrition → metabolic mismatch → increased risk of adult-onset hypertension, insulin resistance, type 2 diabetes, and coronary artery disease. This concept underpins the importance of LBW as a public health, not just neonatal, issue.
SELF-CHECK
A 30-week preterm infant develops abdominal distension, bloody stools, and haemodynamic instability at 2 weeks of age. Plain X-ray shows pneumatosis intestinalis (gas in bowel wall). What is the most likely diagnosis?
A. Hirschsprung disease
B. Neonatal necrotising enterocolitis (NEC)
C. Intussusception
D. Meconium ileus
Reveal Answer
Answer: B. Neonatal necrotising enterocolitis (NEC)
Necrotising Enterocolitis (NEC) classically affects preterm infants, typically presenting at 2–3 weeks of age with abdominal distension, blood in stools (haematochezia), haemodynamic instability, and metabolic deterioration. Pneumatosis intestinalis (gas in the bowel wall — a pathognomonic X-ray finding) confirms the diagnosis. NEC is caused by immature intestinal mucosal barrier + altered colonisation + bowel ischaemia. Hirschsprung disease presents in term infants with delayed meconium passage and does not show pneumatosis. Intussusception is rare in neonates and presents with colicky pain. Meconium ileus is associated with cystic fibrosis and presents in the first day.
Diagnosis and Investigation of LBW
The diagnostic assessment of an LBW neonate begins at birth with a structured clinical evaluation, then progresses to targeted investigations based on the initial clinical findings. The goals are: (1) determine gestational age and plot growth parameters to classify the infant as preterm, SGA, AGA, or LGA; (2) identify imminent complications — particularly hypoglycaemia, hypothermia, and respiratory distress in the first hour; (3) investigate for underlying causes of IUGR when appropriate (TORCH screen, chromosomal karyotype). The investigation strategy is sequenced by urgency: bedside point-of-care tests (blood glucose, temperature, pulse oximetry) must precede all other investigations because they identify the complications that can cause permanent harm within the first few hours. Formal imaging and aetiology workup are planned in parallel once the infant is stabilised.
Gestational age assessment:
- Clinical method: Ballard Score (modified) — assessed within 12 hours of birth; combines 6 neuromuscular + 6 physical criteria, each scored 0–5; maximum 50 corresponds to ≥44 weeks. Useful when antenatal USG is unavailable or unreliable.
- Antenatal method (most accurate): First-trimester ultrasound crown-rump length (CRL) is the gold standard for gestational age assignment.
Growth plotting:
- Plot birth weight, length, and head circumference on the Fenton growth chart (appropriate for preterm neonates) or WHO growth standards to determine percentile for gestational age.
- SGA = below 10th percentile; AGA (appropriate for gestational age) = 10th–90th percentile; LGA = above 90th percentile.
Routine monitoring for complications:
- Blood glucose: monitor at 1 hour, 3 hours, 6 hours, then 6-hourly for first 24 hours (more frequently if symptomatic); threshold <45 mg/dL (2.5 mmol/L) = treat
- Temperature: continuous or 1-2 hourly axillary temperature; maintain 36.5–37.5°C
- Haematocrit/Hb: rule out polycythaemia (Hct >65% — SGA infants at risk) and anaemia
- Sepsis screen (if clinically indicated): CBC, CRP, blood culture, LP if meningitis suspected
- Chest X-ray: for respiratory distress — bilateral granular/ground-glass opacification (RDS) vs streaky infiltrates (wet lung/TTN) vs lobar consolidation (pneumonia)
- Cranial USG: screen for IVH in all <32-week preterms at 3–7 days, repeat at 1 month
- ROP screening: all neonates <32 weeks or birth weight <1500 g; ophthalmology review at 4–6 weeks
Investigation for cause of IUGR:
- Maternal serology: TORCH panel (IgM/IgG) if symmetric IUGR with hepatosplenomegaly or brain calcifications
- Chromosomal karyotype: if dysmorphic features suggest chromosomal cause
- Doppler velocimetry of umbilical artery (antenatal): absent or reversed end-diastolic flow predicts severe placental insufficiency
Management of LBW: Stabilisation, Feeding, and KMC
Management of the LBW neonate covers an immediate stabilisation phase, a feeding and growth phase, and a discharge and follow-up phase. The principles are to provide what the maternal-intrauterine environment would have provided: warmth, nutrition, protection from infection, and neurodevelopmental stimulation — as simply and as close to the mother as possible.
Immediate stabilisation (delivery room and first hour):
Warm the infant immediately (warm resuscitation table, pre-warmed towels); position head-neutral; assess for need for oxygen/PPV (if RDS or apnoea). Administer Vitamin K1 0.5 mg IM (<1.5 kg) or 1 mg IM (≥1.5 kg). Administer BCG + OPV-0 + Hep-B if clinically stable.
Thermal care:
For preterm <34 weeks or weight <1800 g without KMC: incubator or radiant warmer (set to 35–36°C for very preterm). For stable LBW ≥1800 g (or lower once stable off oxygen): initiate KMC.
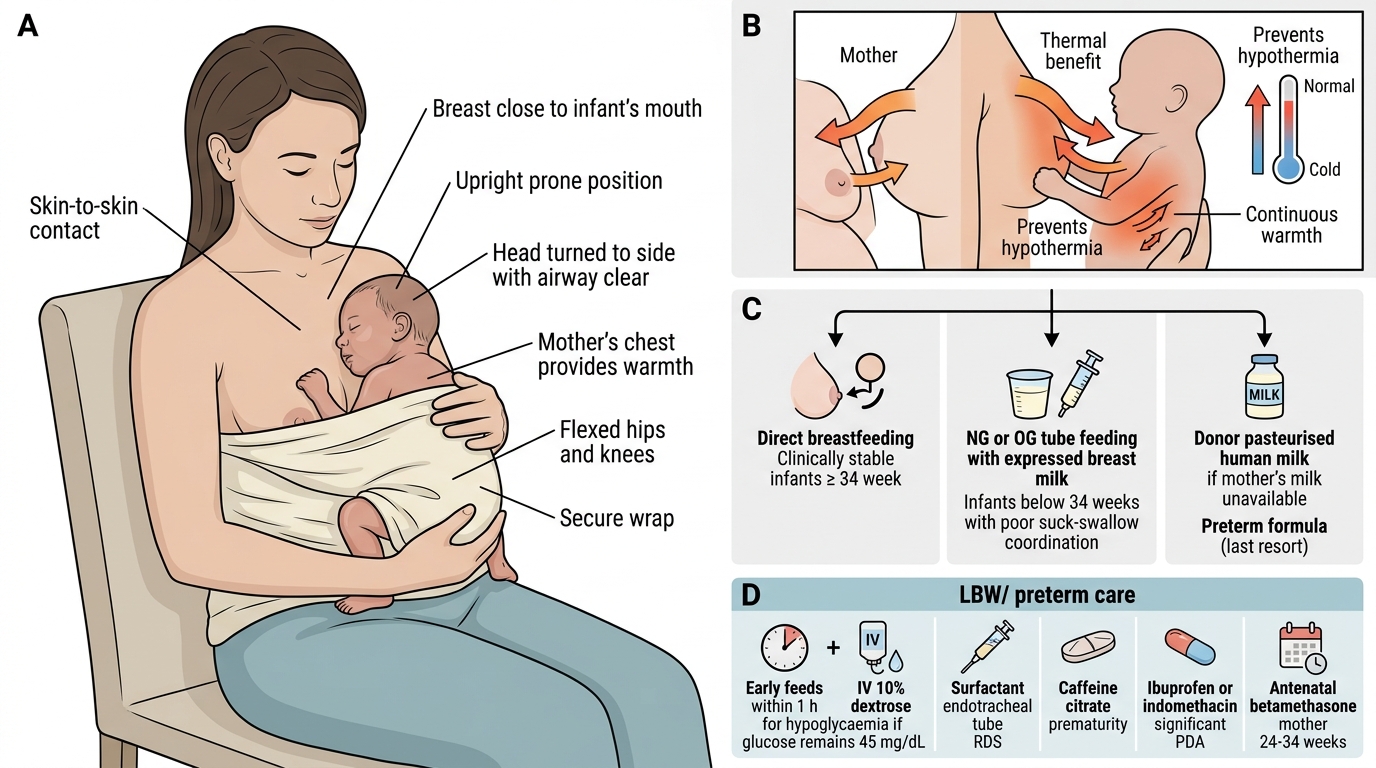
Kangaroo Mother Care (KMC):
KMC is a method of care for stable LBW neonates based on three components: (1) continuous skin-to-skin contact between the mother (or father/caregiver) and the infant in the upright prone position on the chest; (2) exclusive breastfeeding or expressed breast milk; (3) early hospital discharge with follow-up. KMC provides warmth (mother's chest temperature regulates infant's temperature), promotes breastfeeding, reduces sepsis, reduces apnoea, improves weight gain, and reduces parental anxiety. WHO evidence from multicountry trials shows KMC reduces mortality in stable LBW infants born <2000 g. In India, KMC is the standard of care for stable LBW neonates and is promoted under the Facility-Based Newborn Care (FBNC) programme. Contraindications to KMC: infant requiring mechanical ventilation, ongoing intravenous medications (but infant can be on CPAP with KMC).
Kangaroo Mother Care and Feeding Support for LBW Infant
Feeding strategy:
- Expressed breast milk (EBM) is the gold standard for all LBW infants — reduces NEC, improves gut colonisation, provides immune factors, improves neurodevelopmental outcomes.
- Feeding method: if gestational age ≥34 weeks and clinically stable → direct breastfeeding. If <34 weeks or poor suck-swallow → nasogastric (NG) or orogastric (OG) tube feeding with EBM.
- Volumes: start at 60–80 mL/kg/day (enteral) on day 1, increase by 20 mL/kg/day to reach 150–180 mL/kg/day by day 5–7.
- If breast milk unavailable: donor pasteurised human milk (preferred); preterm formula as last resort.
- Hypoglycaemia management: early initiation of feeds (within 1 hour); IV 10% dextrose if oral feeds insufficient or blood glucose <45 mg/dL despite 2 feeds.
Medications for preterm complications:
- Surfactant replacement: intratracheal, for RDS — dramatically reduces mortality; INSURE technique (intubate-surfactant-extubate to CPAP) preferred
- Caffeine citrate (loading 20 mg/kg then 5 mg/kg/day): for apnoea of prematurity — reduces apnoea episodes, extubation failure, and BPD; safe long-term neurodevelopmental profile
- Ibuprofen or indomethacin: for haemodynamically significant PDA
- Antenatal corticosteroids (given to mother 24–34 weeks): betamethasone 12 mg IM × 2 doses, 24 hours apart — reduces RDS severity, IVH, NEC; given to mother before preterm delivery
Discharge criteria for LBW:
- Weight ≥1800 g (or higher if clinically indicated)
- Sustaining body temperature in room temperature for 24 hours
- Established oral/breastfeeds — gaining ≥15–20 g/kg/day
- No apnoea for 7 days off caffeine
- Mother trained and confident in KMC and feeding
- Follow-up for ROP, hearing, neurodevelopment arranged
Prevention of LBW (public health):
- Antenatal care including iron-folic acid, calcium supplementation, balanced energy-protein supplementation
- Treatment of hypertension and infections in pregnancy
- Spacing of pregnancies (>18 months)
- Avoidance of tobacco and alcohol
- Identification and management of anaemia
SELF-CHECK
Which of the following correctly describes Kangaroo Mother Care (KMC) and its evidence base?
A. KMC is a supplement to incubator care used only for infants weighing <1000 g
B. KMC involves intermittent (2–3 hours/day) skin-to-skin contact and formula feeding
C. KMC is continuous skin-to-skin contact + exclusive breastfeeding for stable LBW neonates, shown to reduce mortality in WHO trials
D. KMC is contraindicated if the mother has received antibiotics for postpartum infection
Reveal Answer
Answer: C. KMC is continuous skin-to-skin contact + exclusive breastfeeding for stable LBW neonates, shown to reduce mortality in WHO trials
KMC has three components: (1) continuous (not intermittent) skin-to-skin contact between the infant and mother/caregiver in the upright prone position, (2) exclusive breastfeeding or expressed breast milk, and (3) early discharge with ambulatory follow-up. WHO multicountry evidence demonstrates mortality reduction in stable LBW infants born <2000 g. It is a replacement for incubator care in stable LBW neonates, not a supplement. It applies to stable LBW neonates (not only <1000 g). Maternal antibiotic use is not a contraindication — breast milk continues to be recommended.
Self-Assessment: LBW Clinical Reasoning
Work through these cases using the LBW framework: classify the infant, identify the predominant mechanism of low weight, anticipate the complications, and outline the management approach. Each case tests a different clinical competency domain from this module. Before reading the structured responses, write out your own classification and reasoning — this self-testing process is the most effective way to consolidate diagnostic frameworks. The ability to arrive at the correct classification and first management step from clinical description alone is what will be tested in your examinations and, more importantly, in your clinical practice.
Case 1 — Preterm vs SGA distinction: At 36 weeks, a baby boy is born weighing 1750 g to a 28-year-old primigravida with severe pre-eclampsia (BP 170/110). On examination, the infant has loose skin with a relatively large head, thin cord, and is alert and hungry.
- Classification: Term-equivalent SGA (36 weeks = late preterm, but weight <10th percentile for 36 weeks → SGA); mechanism is IUGR from placental insufficiency due to pre-eclampsia
- Predominant pattern: asymmetric IUGR (brain-sparing) — Ballard gestation ~36 weeks but weight discordant
- Immediate danger: hypoglycaemia (depleted liver glycogen from brain-sparing IUGR) — check blood glucose at 1, 3, 6 hours
- Management: early feeds (EBM or formula), KMC, monitor temperature, monitor jaundice
Case 2 — VLBW complication cascade: A 28-week, 900 g infant (ELBW) is admitted to NICU. Over the next 2 weeks: day 1 — RDS requiring surfactant + CPAP; day 3 — IVH Grade II on cranial USG; day 14 — abdominal distension and bloody stools.
- Identify complications in sequence: RDS (surfactant deficiency) → IVH (germinal matrix haemorrhage) → NEC (preterm gut immaturity)
- Management cascade: surfactant for RDS; NICU monitoring for IVH (serial USG, avoid cerebral blood flow fluctuations); NEC = bowel rest + IV antibiotics + surgical review
- Key long-term concern: Grade II IVH has guarded neurodevelopmental prognosis; NEC may require bowel resection → short bowel syndrome
Case 3 — KMC counselling: A 34-week, 1600 g infant girl has been off oxygen for 24 hours and is being fed by nasogastric tube with expressed breast milk. The mother wants to know when she can 'hold her baby normally.'
- KMC indication: infant is now stable (off oxygen), on enteral feeds → criteria for KMC met
- Counsel the mother: explain skin-to-skin technique (upright prone on chest, covered), the warmth benefit (mother's skin temperature maintains infant's temperature), how to continue NG feeds during KMC, importance of exclusive breastfeeding, and transition to direct breastfeeding as suck-swallow matures (~34+ weeks)
- Discharge planning: once weight ≥1800 g + temperature maintained in room air + established oral feeds, initiate home KMC with follow-up