Page 40 of 53
PE19.15 | Neonatal Hyperbilirubinemia — SDL Guide
Learning Objectives
- Distinguish physiological from pathological neonatal jaundice using timing and clinical criteria
- Explain the pathophysiology of unconjugated and conjugated hyperbilirubinaemia in newborns
- List the common causes of neonatal jaundice including haemolytic and non-haemolytic aetiologies
- Interpret the Bhutani nomogram and AAP/NNF guidelines to determine phototherapy and exchange transfusion thresholds
- Describe the complications of untreated severe hyperbilirubinaemia including kernicterus and BIND
INSTRUCTIONS
Neonatal jaundice is the most common condition requiring evaluation in the first week of life, affecting up to 60% of term and 80% of preterm newborns. While most cases are physiological and self-limiting, failure to recognise pathological hyperbilirubinaemia in time can result in kernicterus — a preventable cause of lifelong disability. As a paediatric clinician, you must be able to assess jaundice at the bedside, request the right investigations, and initiate phototherapy or escalate to exchange transfusion without delay. This module builds the framework for that clinical judgement.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 (Neonatal Jaundice) (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 123 (textbook)
- AAP Clinical Practice Guideline: Management of Hyperbilirubinemia in Newborn Infant ≥35 Weeks of Gestation (2022) (guideline)
- NNF India: Evidence-based Clinical Practice Guidelines on Neonatal Hyperbilirubinemia (2021) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Baby Rishi, a 28-hour-old term male born by normal vaginal delivery to a group-O mother, is brought to you because the ward nurse noticed yellowing of his skin starting from the face and spreading to the chest. The mother's blood group is O-positive; the baby is B-positive. There is no history of any family member needing blood transfusion at birth. Rishi's vital signs are stable, but on examination his sclerae are deeply icteric and Kramer zone 3 is reached. The nursing team wants to know whether to initiate phototherapy. You recall that jaundice in the first 24 hours of life is never physiological — and now you need to act on that knowledge.
WHY THIS MATTERS
Neonatal hyperbilirubinaemia is the leading cause of hospital readmission in the first week of life worldwide, and severe unconjugated hyperbilirubinaemia remains a preventable cause of cerebral palsy, sensorineural hearing loss, and intellectual disability through kernicterus. In India, the condition carries additional epidemiological weight because G6PD deficiency — a significant trigger for haemolytic jaundice — is prevalent in many communities, and preterm births are common. Understanding when to observe, when to treat with phototherapy, and when to escalate to exchange transfusion is a core competency for every primary-care physician, not just a neonatologist skill. The 2022 AAP guideline and NNF India guidelines now provide gestation- and hour-specific nomograms that replace older fixed thresholds, and you must be able to apply them.
RECALL
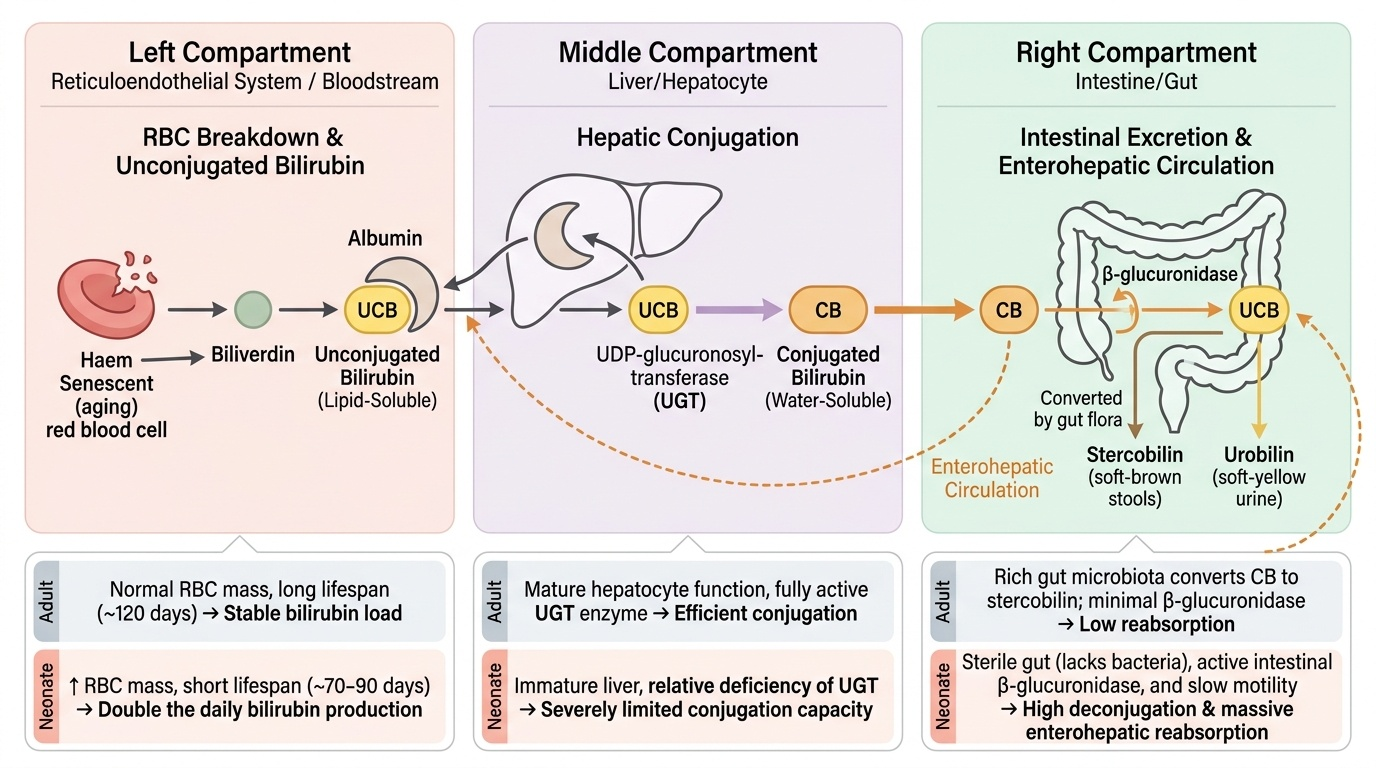
Before proceeding, recall the following from your basic science training. Bilirubin is derived from the breakdown of haem; the enzyme haem oxygenase converts haem to biliverdin, which is then reduced to unconjugated (indirect) bilirubin. Unconjugated bilirubin is lipid-soluble, bound to albumin in plasma, and transported to the liver where hepatic UDP-glucuronosyltransferase conjugates it with glucuronic acid to form water-soluble direct (conjugated) bilirubin, excreted in bile. In the fetal and neonatal period, this conjugating enzyme is relatively immature and bilirubin load is higher because fetal red blood cells (containing HbF) have a shorter lifespan (~70-90 days vs ~120 days in adults). These physiological constraints explain why virtually every newborn has some degree of hyperbilirubinaemia. Also recall that Rh-negative mothers sensitised to Rh antigen can produce IgG antibodies that cross the placenta and haemolyse fetal red cells — prevented by anti-D prophylaxis (Rhogam) given antenatally and post-delivery.
Clinical Presentation and Timing of Neonatal Jaundice
Neonatal jaundice manifests as yellow discolouration of the skin and sclerae and can be detected clinically using Kramer's zones, a system that correlates the cephalocaudal progression of jaundice with estimated serum bilirubin levels. In Kramer's classification, zone 1 (face and neck) corresponds to approximately 5–6 mg/dL, zone 2 (upper trunk to umbilicus) to 6–8 mg/dL, zone 3 (lower abdomen to thighs) to 8–10 mg/dL, zone 4 (arms, lower legs) to 10–12 mg/dL, and zone 5 (palms and soles) to greater than 15 mg/dL. Importantly, Kramer's method is a bedside guide and not a replacement for serum bilirubin measurement — clinical assessment can be unreestimate in darkly pigmented infants and under artificial lighting.
The most critical clinical distinction is between physiological and pathological jaundice, which is primarily determined by the timing of onset:
- Physiological jaundice: Appears on day 2 or 3 of life, peaks between day 3 and 5, and resolves by day 7 in term infants (day 14 in preterm). Total serum bilirubin (TSB) rarely exceeds 12–13 mg/dL in term infants on exclusive formula, or 15 mg/dL in those with breast-milk jaundice. The key characteristic is that it NEVER appears on day 1.
- Pathological jaundice: Defined by any of the following — (1) onset within the first 24 hours of life; (2) TSB rise >5 mg/dL per day; (3) TSB exceeding the high-risk zone on the Bhutani nomogram; (4) conjugated (direct) bilirubin >1 mg/dL or >20% of total; (5) persistence beyond 2 weeks in term or 3 weeks in preterm infants.
- Prolonged jaundice: Jaundice persisting beyond 2 weeks in term infants always requires evaluation of conjugated bilirubin fraction. A raised conjugated fraction (conjugated hyperbilirubinaemia) is always pathological and mandates urgent work-up to exclude biliary atresia, neonatal hepatitis, and metabolic disorders.
IMPORTANT CLINICAL RULE: Jaundice appearing within the first 24 hours of life is ALWAYS pathological and must be attributed to haemolysis (Rh or ABO incompatibility, G6PD deficiency, sepsis) until proven otherwise. Do not watch and wait.
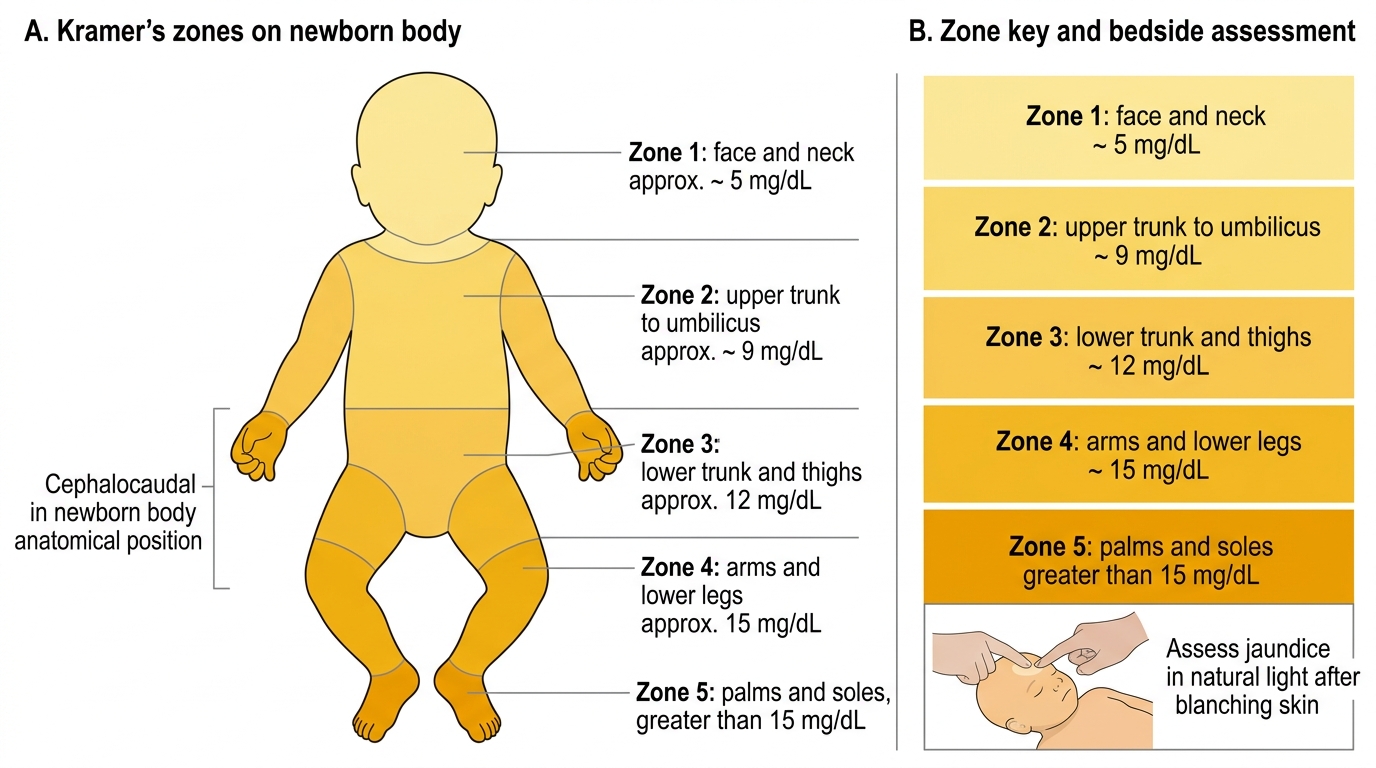
Kramer's Zones of Neonatal Jaundice
Pathophysiology, Aetiology and Classification
The neonatal period is physiologically predisposed to hyperbilirubinaemia for three interrelated reasons: (1) higher red blood cell mass and shorter neonatal RBC lifespan (~70–90 days vs 120 days in adults) produce a larger bilirubin load; (2) immature hepatic conjugation capacity due to relative deficiency of UDP-glucuronosyltransferase; and (3) active enterohepatic circulation — intestinal β-glucuronidases deconjugate bilirubin diglucuronide, which is then reabsorbed. Exclusive breastfeeding in the early days (before milk comes in) leads to reduced intestinal motility and increased reabsorption, contributing to the higher peak seen in breast-fed infants (breast-feeding jaundice = inadequate intake, distinct from breast-milk jaundice = inhibitory substances in mature breast milk peaking at 2 weeks).
Provided image
Aetiological classification is clinically useful by day of onset and bilirubin type:
Causes by timing:
• Day 1 (always pathological): Rh incompatibility, ABO incompatibility, G6PD deficiency with trigger, congenital infection (TORCH), red cell structural defects (hereditary spherocytosis).
• Days 2–3 (physiological or early pathological): physiological jaundice, polycythaemia, bruising (cephalohaematoma), swallowed maternal blood, early-onset sepsis.
• Prolonged (>2 weeks term): breast-milk jaundice, hypothyroidism, neonatal hepatitis, biliary atresia, Crigler-Najjar syndrome, TORCH.
| Cause | Type | Day of onset | Key feature |
|---|---|---|---|
| Rh incompatibility | Haemolytic (unconjugated) | Day 1 | DAT +ve; hydrops possible |
| ABO incompatibility | Haemolytic (unconjugated) | Day 1–2 | Mother O, baby A/B; DAT weak +ve |
| G6PD deficiency | Haemolytic (unconjugated) | Day 1–3 | X-linked; trigger-dependent |
| Physiological | Unconjugated | Day 2–3 | Diagnosis of exclusion |
| Breast-milk jaundice | Unconjugated | Peaks 2 wk | Peaks, then resolves if fed formula |
| Biliary atresia | CONJUGATED | Prolonged | Pale stools, dark urine — URGENT |
| Neonatal hepatitis | Conjugated or mixed | Prolonged | Hepatosplenomegaly; LFT abnormal |
Kernicterus and BIND: When unconjugated bilirubin overwhelms albumin-binding capacity, free bilirubin crosses the blood-brain barrier and deposits in the basal ganglia, subthalamic nuclei, and cerebellum. The spectrum is called bilirubin-induced neurological dysfunction (BIND): BIND-1 = subtle (hypotonia, poor suck, high-pitched cry); BIND-2 = moderate (retrocollis, opisthotonus, fever, seizures); BIND-3 = severe (acute kernicterus); chronic kernicterus = athetoid cerebral palsy + sensorineural hearing loss + dental enamel dysplasia + upward gaze palsy.
SELF-CHECK
A 20-hour-old term neonate is noted to have jaundice involving the face and upper chest. Mother is O-positive, baby is A-positive. Which of the following is the MOST likely cause?
A. Physiological jaundice
B. ABO incompatibility
C. Breast-milk jaundice
D. Rh haemolytic disease
Reveal Answer
Answer: B. ABO incompatibility
Jaundice within the first 24 hours is ALWAYS pathological. The mother-O to baby-A combination is the hallmark of ABO incompatibility, the most common cause of pathological jaundice in the first day. Physiological jaundice never appears before 24 hours. Breast-milk jaundice peaks around 2 weeks. Rh disease requires an Rh-negative mother sensitised to Rh-positive fetal cells — this mother is Rh-positive, so Rh incompatibility is not applicable here.
Diagnosis and Investigation
The initial assessment of a jaundiced neonate requires both a clinical evaluation and targeted laboratory investigations to establish the severity of jaundice, identify the underlying cause, and determine treatment urgency. Clinical assessment using Kramer's zones provides a rapid bedside estimate, but serum total bilirubin (TSB) remains the gold standard for quantification. Transcutaneous bilirubin (TcB) measurement is a non-invasive, validated screening tool for TSB ≤15 mg/dL in term/near-term infants, but TSB must be checked before initiating phototherapy and whenever TcB is elevated.
Interpreting the Bhutani nomogram (AAP/NNF hour-specific nomogram): The nomogram plots TSB against hours of age (0–144 h) for infants ≥35 weeks and assigns four risk zones — low, low-intermediate, high-intermediate, and high. A pre-discharge bilirubin in the high zone predicts subsequent severe hyperbilirubinaemia with high sensitivity. Critically, phototherapy and exchange transfusion thresholds are NOT fixed numbers — they vary with gestational age (GA), hours of age, and additional risk factors (haemolysis, G6PD deficiency, asphyxia, hypoalbuminaemia, prior sibling who required phototherapy). The 2022 AAP guideline provides separate threshold curves for infants at GA ≥38 weeks without risk factors vs GA 35–37+6/7 weeks or any neonate with risk factors.
Investigations:
• TSB (total and direct/conjugated fraction) — direct bilirubin >1 mg/dL (or >20% of TSB) = always pathological
• Blood group and direct antiglobulin test (DAT / direct Coombs test) — identifies antibody-coated RBCs in haemolytic disease
• Peripheral blood smear — spherocytes (ABO/spherocytosis), fragmented cells, polychromasia
• G6PD enzyme assay or fluorescent spot test — standard of care in India given high prevalence; note: testing within 2 weeks of haemolytic episode may give falsely normal result (reticulocytes have higher G6PD)
• Serum albumin — needed to calculate bilirubin-albumin ratio (threshold for exchange transfusion if TSB:albumin >8 mg/g in low-risk term infant)
• Complete blood count — anaemia, reticulocytosis, elevated total bilirubin
• Sepsis screen (blood culture, CRP) if infection suspected
• Urine-reducing substances, thyroid function, TORCH titres — if prolonged jaundice with conjugated fraction raised
• Urgent hepatobiliary ultrasound if conjugated bilirubin raised — biliary atresia is a surgical emergency; Kasai portoenterostomy must be done before 60 days for best outcome
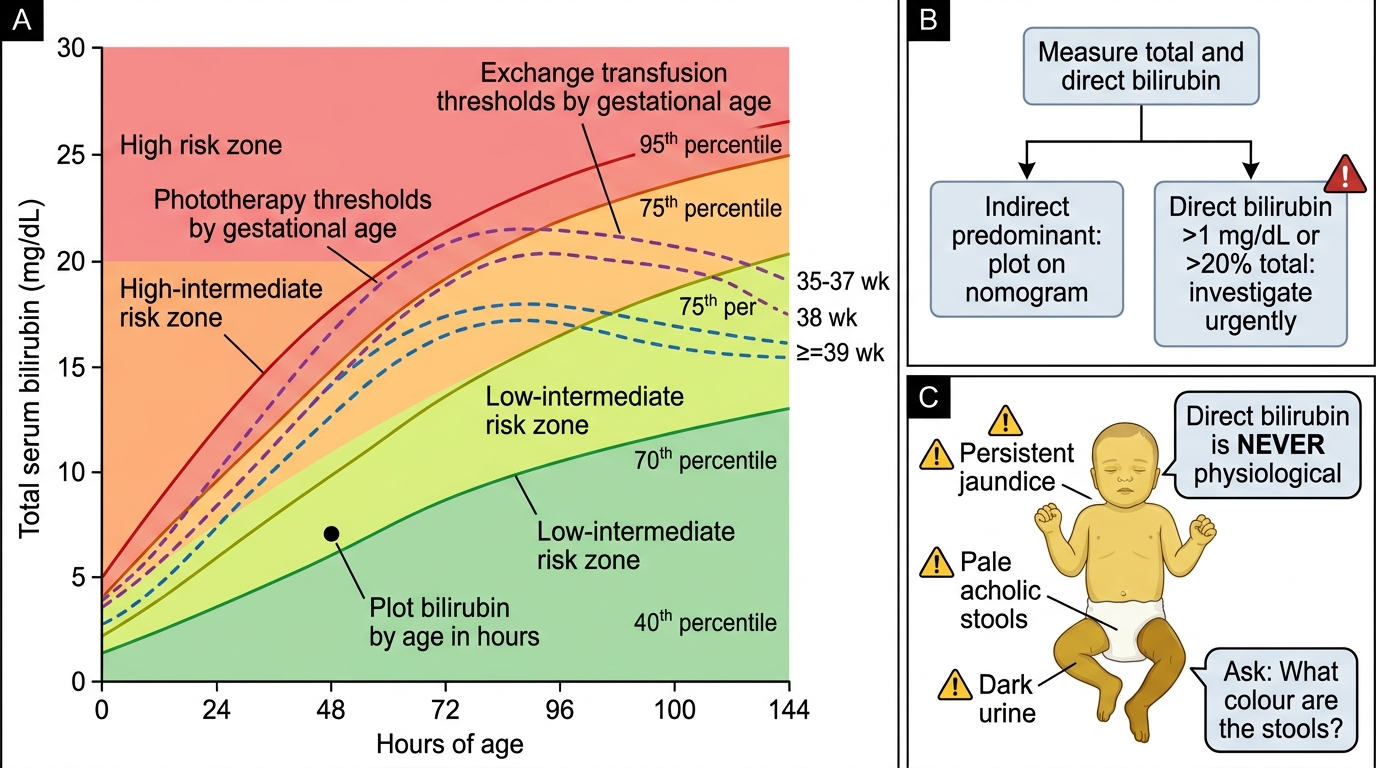
Bhutani Nomogram and Direct Bilirubin Red Flags
CLINICAL PEARL
Direct bilirubin is NEVER physiological. Any neonate with conjugated (direct) bilirubin >1 mg/dL (or >20% of total serum bilirubin) must be investigated promptly — this picture does not occur in physiological jaundice or simple haemolytic disease. Biliary atresia presents with persistent jaundice, pale stools (acholic), and dark urine; the disease is progressive and the window for the Kasai portoenterostomy is narrow (ideally <60 days of age). A missed diagnosis of biliary atresia is one of the most serious preventable errors in neonatal medicine. Teach yourself to ask: 'What colour are the stools?' at every postnatal visit for a jaundiced baby.