Page 41 of 53
PE19.15 | Neonatal Hyperbilirubinemia — SDL Guide (Part 2)
Management: Phototherapy and Exchange Transfusion
The management of neonatal hyperbilirubinaemia follows a stepwise approach based on TSB level, gestational age, hours of age, and risk factors. The two principal interventions are phototherapy and exchange transfusion, each with specific indications derived from the AAP/NNF hour-specific nomograms.
Provided image
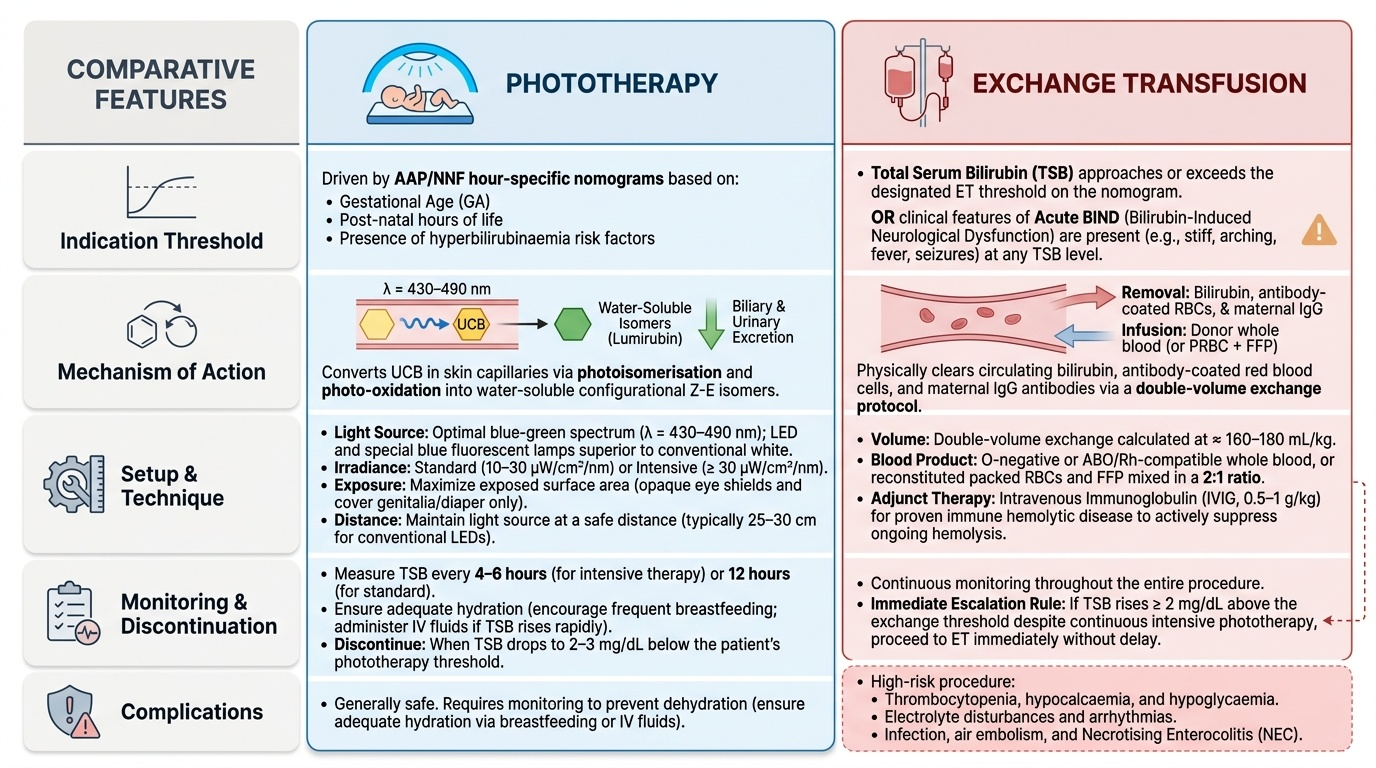
Phototherapy:
The mechanism involves photoisomerisation and photo-oxidation of unconjugated bilirubin in skin capillaries and superficial tissue, converting it to water-soluble isomers (lumirubin, configurational Z-E isomers) that are excreted in bile and urine without hepatic conjugation. Efficacy is determined by: (1) type of light — blue-green spectrum (430–490 nm) is optimal; LED and special blue fluorescent lamps are superior to conventional white; (2) irradiance — 10–30 µW/cm²/nm (intensive phototherapy ≥30 µW/cm²/nm for rapidly rising TSB); (3) surface area exposed — maximise by exposing all skin (patch eyes and genitalia only); (4) distance — maintain lamp distance per manufacturer recommendation (typically 25–30 cm for conventional LEDs).
Setup principles: (a) expose maximum skin surface; (b) patch both eyes with opaque shields to prevent retinal damage; (c) ensure adequate hydration (encourage breastfeeding; consider IV fluids if TSB rising fast); (d) monitor TSB every 4–6 hours during intensive phototherapy, or 12 hours for standard; (e) discontinue when TSB is 2–3 mg/dL below threshold.
Exchange transfusion (ET): Indicated when TSB approaches or exceeds the exchange transfusion threshold on the nomogram, or when clinical features of acute BIND are present (stiff, arching, fever, seizures) at any bilirubin level. The procedure uses double-volume exchange (~160–180 mL/kg) with O-negative or ABO/Rh-compatible whole blood (or reconstituted packed RBCs + fresh-frozen plasma in 2:1 ratio) to remove antibody-coated red cells, circulating antibody (IgG), and bilirubin. Complications include: thrombocytopenia, hypocalcaemia, hypoglycaemia, electrolyte disturbances, infection, NEC, air embolism, and arrhythmias. Monitor continuously. If TSB rises ≥2 mg/dL above exchange threshold despite intensive phototherapy → proceed to ET without delay.
Other measures: Pharmacological agents are second-line. Intravenous immunoglobulin (IVIG 0.5–1 g/kg) reduces haemolysis and may decrease need for ET in proven haemolytic disease (Rh/ABO) — given with intensive phototherapy. Phenobarbitone (enzyme inducer) is rarely used. Tin-mesoporphyrin (haem oxygenase inhibitor) reduces bilirubin production but is not widely available.
SELF-CHECK
A 3-day-old term neonate (38 weeks GA) has TSB of 18 mg/dL and is receiving standard phototherapy. Repeat TSB after 6 hours is 21 mg/dL. The exchange transfusion threshold on the AAP nomogram for this infant (no additional risk factors) at 72 hours is 22 mg/dL. What is the NEXT best step?
A. Continue standard phototherapy and repeat TSB in 12 hours
B. Upgrade to intensive phototherapy and add IVIG
C. Proceed to exchange transfusion immediately
D. Add phenobarbitone and continue current phototherapy
Reveal Answer
Answer: B. Upgrade to intensive phototherapy and add IVIG
The TSB rose by 3 mg/dL despite standard phototherapy in 6 hours, and at 21 mg/dL it is approaching (within 1 mg/dL of) the exchange transfusion threshold of 22 mg/dL. The correct step is to escalate to intensive phototherapy (irradiance ≥30 µW/cm²/nm, maximum surface area) and add IVIG if haemolytic cause is confirmed, then recheck TSB in 2–4 hours. Exchange transfusion is indicated if TSB meets or exceeds the nomogram threshold, or if intensive phototherapy fails to contain the rise. Do not wait 12 hours when TSB is near the exchange threshold.
SELF-CHECK
A 6-week-old term infant is referred for persistent jaundice. Examination shows hepatosplenomegaly, dark urine, and pale (acholic) stools. TSB is 8 mg/dL with conjugated bilirubin 4.2 mg/dL. What is the priority action?
A. Initiate phototherapy and monitor
B. Start phenobarbitone to improve conjugation
C. Urgent hepatobiliary ultrasound and surgical referral for possible biliary atresia
D. Reassure and review in 2 weeks
Reveal Answer
Answer: C. Urgent hepatobiliary ultrasound and surgical referral for possible biliary atresia
Conjugated bilirubin >1 mg/dL (here 4.2 mg/dL = >20% of TSB) is NEVER physiological. The combination of pale stools, dark urine, hepatosplenomegaly, and prolonged jaundice is the classic presentation of biliary atresia. Phototherapy and phenobarbitone do NOT treat cholestatic jaundice. The Kasai portoenterostomy (surgical bypass of the obliterated biliary tree) has the best outcomes if performed before 60 days of age — delay is catastrophic. Urgent imaging and surgical referral are the priority.
Self-Assessment: Neonatal Hyperbilirubinemia
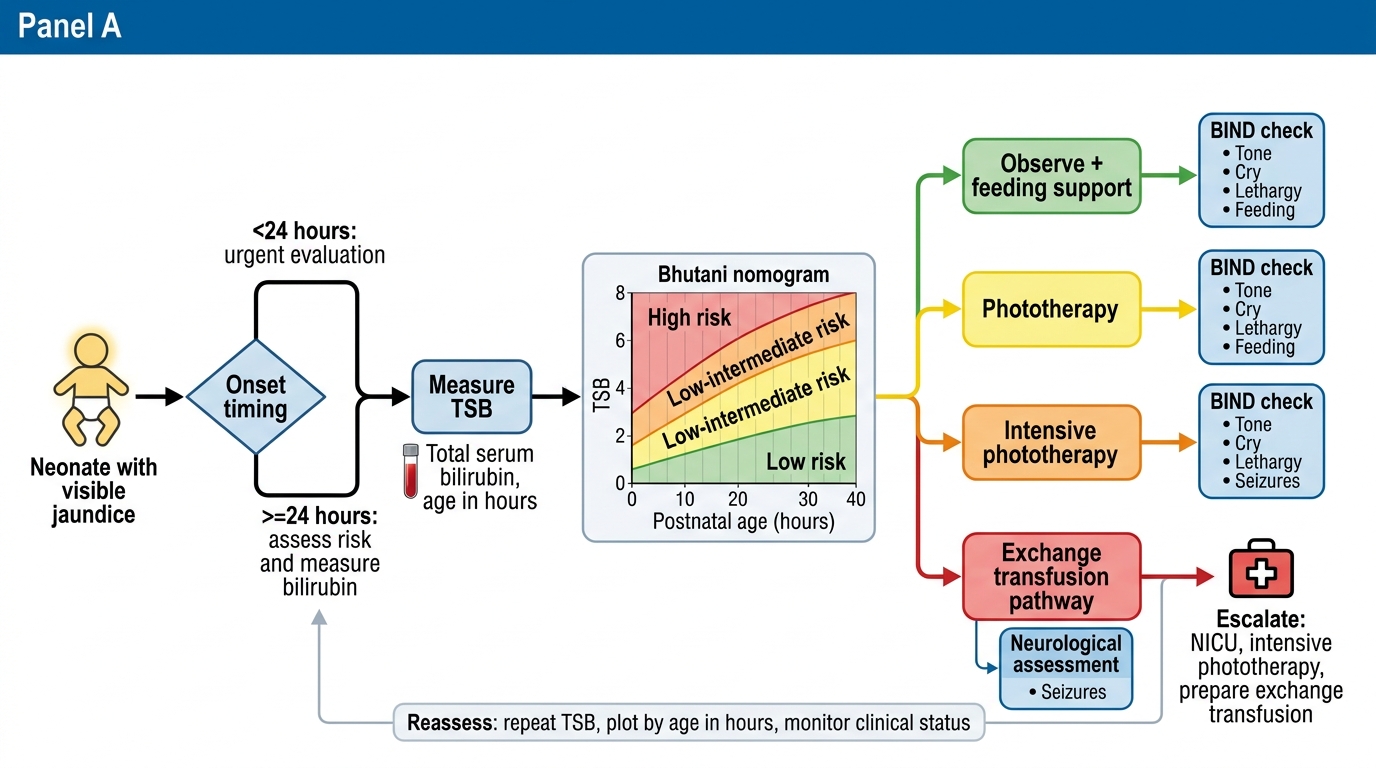
The following questions consolidate your learning on neonatal hyperbilirubinaemia — a condition where the margin between observation and intervention can be measured in hours, and where delayed recognition leads to preventable permanent neurological injury. Neonatal jaundice is ubiquitous in the newborn nursery, but the clinical skill lies in distinguishing the benign physiological variant from the pathological forms that demand urgent investigation and treatment. As you work through each scenario below, apply the structured approach you have built in this module: first establish the timing of onset (day 1 versus later); second, determine whether the bilirubin is conjugated or unconjugated; third, plot the TSB on the Bhutani hour-specific nomogram for the infant's gestational age and risk-factor category; and fourth, check for any clinical features of bilirubin-induced neurological dysfunction (BIND) that override the numerical threshold and demand immediate escalation. This self-assessment is also an opportunity to internalise the practical management steps — phototherapy setup, monitoring intervals, and the precise indications for exchange transfusion — so that you can apply them confidently on the ward without hesitation.
Key diagnostic framework:
• Is onset within 24 hours? → Always pathological; haemolysis until proven otherwise
• Is the conjugated (direct) fraction raised (>1 mg/dL or >20% total)? → Always pathological; work up for biliary atresia, neonatal hepatitis
• Does TSB fall in the phototherapy or exchange transfusion zone on the hour-specific Bhutani nomogram? → Threshold is gestational-age and risk-factor dependent
• Are there signs of BIND (hypertonia, opisthotonus, high-pitched cry, seizures)? → Immediate exchange transfusion regardless of TSB level
Core recall summary:
1. Physiological jaundice: day 2–3 onset, peaks day 3–5, resolves day 7 term / day 14 preterm; NEVER day 1
2. Commonest cause of day-1 jaundice: ABO incompatibility (mother O + baby A or B); Rh disease in sensitised Rh-negative mother
3. G6PD deficiency: X-linked recessive; enzyme assay may be falsely normal if tested during acute haemolysis (reticulocytes have higher G6PD activity)
4. Prolonged jaundice (>2 weeks term): must check conjugated bilirubin; biliary atresia window for Kasai <60 days
5. Phototherapy: blue-green light 430–490 nm; intensive ≥30 µW/cm²/nm; monitor TSB every 4–6 hours on intensive phototherapy
6. Exchange transfusion: double-volume (~160–180 mL/kg); removes sensitised RBCs, IgG antibody, and bilirubin
Neonatal Jaundice Management Algorithm