Page 28 of 53
PE19.10 | Neonatal Hypoglycemia — SDL Guide (Part 2)
Diagnosis: Screening and Investigations
The diagnosis of neonatal hypoglycemia requires confirmation by a laboratory plasma glucose, but bedside glucometry is used for screening and real-time management decisions. The operational treatment threshold endorsed by the NNF India and the AAP is whole-blood glucose <45 mg/dL (approximately equivalent to plasma glucose <50 mg/dL, as plasma values are ~10–15% higher than whole-blood values on glucometers). Any neonate with a glucometer reading below 45 mg/dL should be treated promptly without waiting for laboratory confirmation. It is important to remember that glucometers have a coefficient of variation of 10–15% and are less accurate at low glucose values; therefore, clinical judgement must supplement the number — a lethargic, jittery neonate with a glucometer reading of 47 mg/dL still warrants close scrutiny and repeat testing. The laboratory glucose (fluoride oxalate tube, measured enzymatically) remains the gold standard when there is diagnostic uncertainty, but treatment should never be delayed while awaiting it in a symptomatic neonate.
Who to screen:
- All IDMs and LGA neonates (birth weight >4 kg)
- All SGA neonates (birth weight <10th centile or <2.5 kg)
- All preterm neonates (<37 weeks)
- Neonates with birth asphyxia, hypothermia, or polycythaemia
- Any neonate with symptoms suggestive of hypoglycemia regardless of risk category
Screening schedule: Check pre-feed blood glucose at 1–2 hours after birth, then every 3–6 hours for the first 24–48 hours in at-risk neonates. Continue until blood glucose is consistently ≥45 mg/dL on two consecutive readings while on full feeds.
Investigations for persistent or recurrent hypoglycemia (beyond 48–72 h despite adequate glucose intake):
- Critical sample at the time of hypoglycemia: insulin, C-peptide, cortisol, growth hormone, glucagon, free fatty acids (FFAs), beta-hydroxybutyrate (ketones), lactate, ammonia
- An insulin-to-glucose ratio >0.3 or detectable insulin with plasma glucose <50 mg/dL confirms hyperinsulinism
- Inappropriately low ketones (FFAs elevated but ketones low) suggests a fatty-acid oxidation defect
- Urine reducing substances: positive in galactosaemia (but negative with glucose-oxidase dipsticks)
- Genetic testing for KATP channel mutations if congenital hyperinsulinism suspected
SELF-CHECK
A 1.9 kg baby born at 34 weeks has a glucometer reading of 38 mg/dL at 2 hours of life. The baby is asymptomatic and awake. What is the correct first step?
A. Administer 50% dextrose 1 mL/kg IV immediately
B. Feed the baby expressed breast milk or formula and recheck in 30–60 minutes
C. Administer 10% dextrose 2 mL/kg IV bolus immediately
D. Observe and recheck glucose only if symptoms develop
Reveal Answer
Answer: B. Feed the baby expressed breast milk or formula and recheck in 30–60 minutes
In an asymptomatic preterm neonate with glucose 38 mg/dL, the first step is enteral feeding (expressed breast milk or formula). IV dextrose is reserved for symptomatic hypoglycemia, inability to feed, or glucose that remains below 45 mg/dL despite enteral feeds. 50% dextrose is ABSOLUTELY contraindicated in neonates — it causes rebound hypoglycemia and vascular necrosis. Option D is wrong: every at-risk neonate with glucose <45 mg/dL needs active management, not observation alone.
Management of Neonatal Hypoglycemia
Management is stratified by severity (glucose level), symptoms, and the neonate's ability to feed enterally. The overarching goal is to restore and maintain blood glucose above 45 mg/dL without causing rebound hypoglycemia or vascular injury.
Step 1 — Asymptomatic, glucose 36–44 mg/dL, able to feed:
Initiate or increase enteral feeds immediately (10–15 mL/kg expressed breast milk or formula). Recheck glucose 30–60 minutes after the feed. If glucose rises to ≥45 mg/dL, continue close monitoring. If it fails to rise or falls further, escalate to IV dextrose.
Step 2 — Symptomatic or glucose <36 mg/dL or unable to feed:
Administer a mini-bolus of 10% dextrose 2 mL/kg IV (approximately 200 mg/kg glucose) over 5 minutes. This rapidly restores blood glucose. NEVER use 50% dextrose in neonates — the hyperosmolar load causes rebound hyperinsulinism (worsening subsequent hypoglycemia), and extravasation causes severe tissue necrosis. Immediately after the bolus, start a continuous glucose infusion at a glucose infusion rate (GIR) of 6–8 mg/kg/min using 10% dextrose at an appropriate rate.
Calculating GIR: GIR (mg/kg/min) = [Dextrose concentration (%) × infusion rate (mL/hr)] ÷ [6 × weight (kg)]
For a 2 kg neonate on 10% dextrose: a rate of 7.2 mL/hr delivers GIR ≈ 6 mg/kg/min.
Step 3 — Escalation for persistent hypoglycemia (glucose <45 mg/dL despite GIR ≥8 mg/kg/min):
- Increase GIR in increments of 2 mg/kg/min up to 12–15 mg/kg/min
- Central venous access (umbilical venous catheter) is needed for dextrose concentrations >12.5%
- If hyperinsulinism is confirmed or strongly suspected: diazoxide (5–15 mg/kg/day in 2–3 divided doses, opens KATP channels to suppress insulin) or octreotide (5–20 µg/kg/day) for diazoxide-unresponsive cases
- Glucagon (0.1–0.3 mg/kg IM/IV, max 1 mg) can temporarily mobilise hepatic glycogen in emergencies
- Surgical pancreatectomy (partial or near-total) is reserved for medically refractory congenital hyperinsulinism
Weaning: Once glucose is stable on IV for 12–24 hours and enteral feeds are tolerated, gradually wean GIR by 2 mg/kg/min every 4–6 hours while monitoring pre-feed glucose.
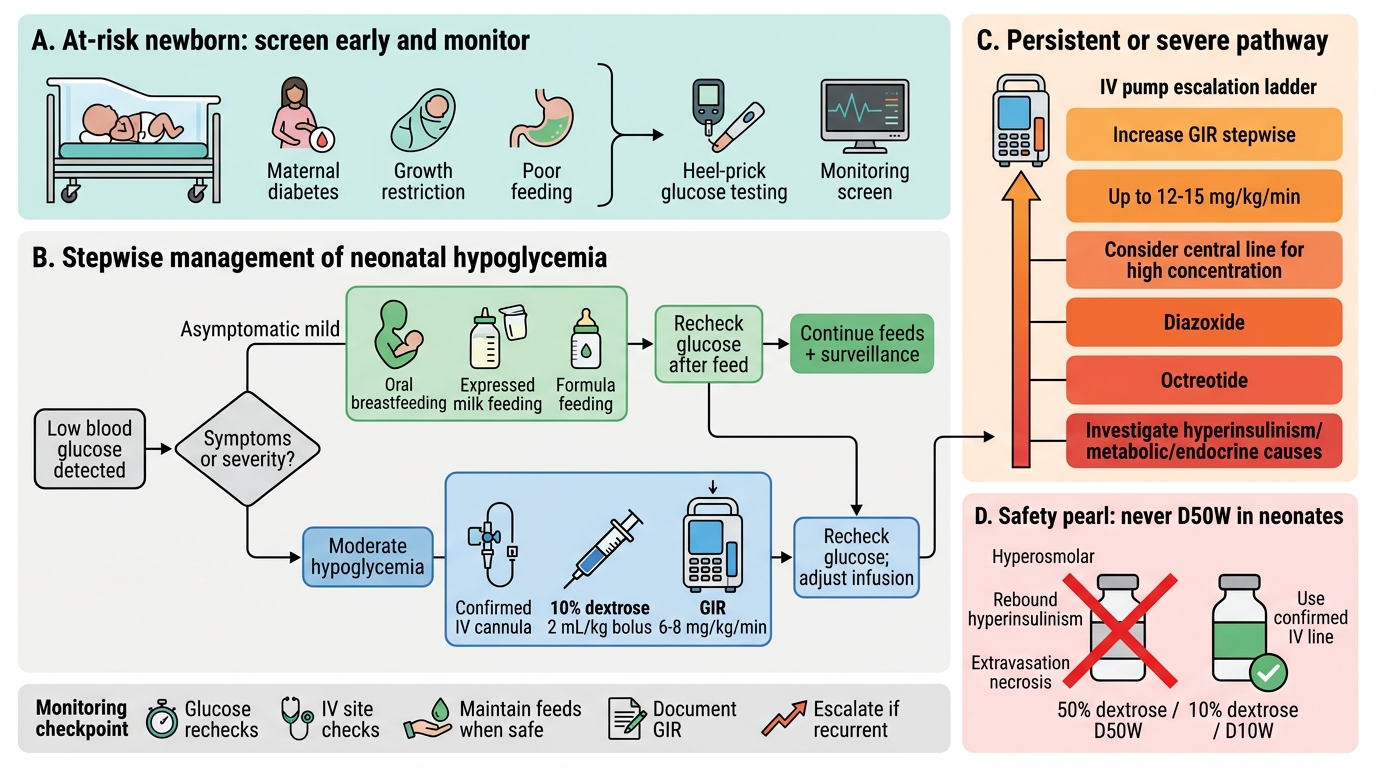
Stepwise Management of Neonatal Hypoglycemia
CLINICAL PEARL
Never use 50% dextrose in neonates. The adult reflex of giving 50% dextrose (D50W) is dangerous in neonates. The hyperosmolar bolus (2,500 mOsm/L) causes rebound hyperinsulinism — blood glucose overshoots, β-cells respond with an insulin surge, and glucose crashes again worse than before. If the 50% dextrose extravasates into subcutaneous tissue, it causes full-thickness necrosis requiring skin grafting. The correct concentration for emergency IV use in neonates is 10% dextrose, and even this must be delivered through a confirmed IV line. A useful aide-memoire: '10% for neonates, 50% for adults — never mix them up.'
Prevention and Monitoring
Prevention begins with identifying at-risk neonates before hypoglycemia occurs, not after. A systematic approach to risk stratification and early enteral feeding is the most effective and cost-efficient preventive strategy. In most cases, the at-risk category is identifiable antenatally — maternal diabetes, growth restriction on antenatal ultrasound, or known preterm delivery — so the neonatal team can prepare for proactive glucose surveillance from the moment of birth. Risk stratification should be completed within the first hour of birth, and the first pre-feed glucose check should be performed at 1–2 hours regardless of whether symptoms are present. Timely initiation of breastfeeding or expressed breast milk feeds is both the safest and most physiological first-line preventive measure for mild transitional hypoglycemia. It also confers benefits beyond glucose homeostasis: breast milk contains lactose (galactose + glucose), medium-chain triglycerides, and enteroglucagon stimulants that collectively sustain postprandial glucose stability more durably than formula or IV dextrose alone.
At-risk categories requiring proactive glucose screening:
- Maternal diabetes (gestational or pre-gestational) — IDMs should have glucose checked at 1–2 hours, then every 3–6 hours for 24 hours
- Preterm neonates (<37 weeks) — regardless of other risk factors
- SGA/IUGR — any baby below the 10th centile or below 2.5 kg
- LGA (birth weight >4 kg) — suspect maternal diabetes even if not formally diagnosed
- Perinatal asphyxia — impaired glycogen mobilisation and increased anaerobic glucose consumption
- Polycythaemia — haematocrit >65%; treat underlying polycythaemia if symptomatic hypoglycemia persists
- Hypothermia — any neonate with core temperature <36.5°C should have glucose checked
Preventive measures:
1. Early initiation of breastfeeding within 30–60 minutes of birth for all neonates
2. Kangaroo mother care (skin-to-skin contact) maintains thermal stability, promotes breastfeeding, and has been shown to reduce hypoglycemia incidence in LBW and preterm neonates
3. Maintenance of neutral thermal environment in incubators or radiant warmers for preterm and LBW neonates — warm babies burn less glucose
4. Avoidance of unnecessary separation of mother and newborn that delays the first feed
5. Prophylactic buccal dextrose gel (40% oral gel 200 mg/kg, 0.5 mL/kg × 1–2 doses) for high-risk neonates in settings where IV access may be delayed — endorsed by some NNF centres
Monitoring frequency should be individualised: check pre-feed glucose every 3–6 hours for at least 24 hours in at-risk neonates. Discharge or reduction of monitoring frequency requires two consecutive pre-feed readings ≥45 mg/dL while on full enteral feeds.