Page 34 of 53
PE19.12 | Neonatal Seizures — SDL Guide
Learning Objectives
- Describe the clinical types of neonatal seizures, emphasising subtle seizures as the most common and most easily missed
- Enumerate the causes of neonatal seizures in order of frequency, with emphasis on hypoxic-ischaemic encephalopathy, hypoglycemia, and hypocalcemia
- Outline the structured diagnostic approach including urgent metabolic screen, EEG, and neuroimaging
- Apply the antiepileptic drug ladder for neonatal seizures: correct the metabolic cause first, then phenobarbitone 20 mg/kg IV as first-line AED
- Describe the role of therapeutic hypothermia in HIE-related neonatal seizures
INSTRUCTIONS
Neonatal seizures are a neurological emergency occurring in 1–5 per 1,000 live births, with significantly higher rates in preterm neonates. They are a signal of significant brain dysfunction and carry a substantial risk of mortality and neurodevelopmental disability. Unlike older children, neonates rarely have the classic generalised tonic-clonic seizure — the most common type is 'subtle', presenting as eye deviation, lip smacking, or cycling limb movements, easily mistaken for normal newborn behaviour or jitteriness. Recognising these subtle signs, rapidly identifying the treatable metabolic causes, and knowing the correct antiepileptic drug ladder are the core competencies this module builds.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 7 — Neonatal Neurology (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 619 — Neonatal Seizures (textbook)
- NNF India — Clinical Practice Guidelines on Neonatal Seizures (2020) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 1-day-old term neonate, born after a prolonged second stage with fetal bradycardia, is noted by the bedside nurse to have intermittent episodes of staring, horizontal eye deviation, and repetitive lip smacking lasting about 30 seconds, recurring every 10 minutes. The Apgar scores were 4 at 1 minute and 7 at 5 minutes. Blood glucose is 58 mg/dL. The intern observes the next episode and is unsure whether it is a seizure or normal newborn behaviour. Is it a seizure? What is the most likely cause? And what must be done in the next 30 minutes?
WHY THIS MATTERS
Neonatal seizures occur in approximately 1–5 per 1,000 term live births and up to 57 per 1,000 very preterm neonates. They are clinically important for three reasons: they signal significant underlying brain pathology, they cause additional neuronal injury through excitotoxicity and metabolic demand during the seizure itself, and — crucially — a significant proportion are caused by rapidly reversible metabolic disturbances. Hypoglycemia, hypocalcemia, and hyponatraemia together account for 10–15% of neonatal seizures; these cases resolve promptly with metabolite correction and may not require antiepileptic drugs at all. Failing to check glucose and calcium before starting phenobarbitone is a common and preventable clinical error. Additionally, HIE-associated seizures are now a strong indication for therapeutic hypothermia, which reduces long-term neurodevelopmental disability if started within 6 hours of birth — making rapid diagnosis essential.
RECALL
From Physiology, recall that neuronal excitability is determined by the balance between excitatory (glutamate, acting on NMDA/AMPA receptors) and inhibitory (GABA, acting on GABA-A receptors) neurotransmission. A seizure occurs when this balance is disrupted: either excess glutamate activation, or failure of GABAergic inhibition, leads to synchronised, self-sustaining neuronal discharge. Importantly, in neonates, GABA is paradoxically excitatory rather than inhibitory in the first days of life — because the neuronal chloride transporter NKCC1 is more active than KCC2, keeping intracellular chloride high, so GABA-A channel opening causes chloride efflux (depolarisation) rather than influx (hyperpolarisation). This explains why benzodiazepines (GABA-A agonists) are less effective in neonates than in older children. Metabolic factors such as hypoglycemia, hypocalcemia, and hyponatraemia all reduce the seizure threshold by reducing neuronal membrane stability and depleting ATP-dependent Na⁺/K⁺-ATPase function.
Clinical Presentation: Types of Neonatal Seizures
Neonatal seizures differ fundamentally from childhood seizures in their clinical expression, because the neonatal brain lacks the mature myelination and cortical organisation needed to generate the synchronised, bilaterally propagated discharges that produce classic generalised tonic-clonic activity. Instead, neonatal seizures are predominantly focal or fragmentary, and many have no EEG correlate at all — so-called 'electroclinical dissociation.' The most important practical consequence is that the most common seizure type — subtle seizures — is easy to miss or misattribute to normal neonatal behaviour. A final-year student must be able to recognise all four clinical types and understand which types correlate with EEG abnormality and which do not.
Subtle seizures are the most common type, occurring in both term and preterm neonates. They manifest as brief, stereotyped, non-suppressible movements or behaviours that recur with a regular periodicity. The specific manifestations include: horizontal eye deviation or sustained eye opening with glazed stare; repetitive blinking or fluttering of the eyelids; oral-buccal-lingual movements (lip smacking, sucking, chewing, tongue protrusion); autonomic phenomena (apnoea, changes in heart rate, salivation, flushing); and 'swimming', 'cycling', or 'pedalling' limb movements. The key distinguishing feature from jitteriness is that subtle seizures are not suppressible by gentle restraint of the limb or repositioning, whereas jitteriness stops when the limb is gently held. Subtle seizures often lack a consistent EEG correlate — they may be 'motor automatisms' driven by subcortical release rather than cortical discharge — but this does not make them benign.
Focal clonic seizures are rhythmic, repetitive jerking of a single limb or one side of the face, at a rate of 1–3 per second. They have a clear EEG correlate and are most often caused by focal cortical injury (perinatal arterial ischaemic stroke, focal haemorrhage). The baby is typically awake and the jerking cannot be stopped by restraint.
Tonic seizures involve sustained posturing — either tonic extension of all four limbs (resembling decerebrate posturing) or focal tonic deviation of head and eyes. Generalised tonic seizures often reflect brainstem release from cortical inhibition and have a poor prognosis; they are common in preterm neonates with intraventricular haemorrhage.
Myoclonic seizures are rapid, single, or repetitive jerks — brief, lightning-like contractions — that may be focal, multifocal, or generalised. Focal and multifocal myoclonic seizures may have no EEG correlate; generalised myoclonic seizures (especially the 'early myoclonic encephalopathy' pattern) correlate with severe brain pathology and inborn errors of metabolism.
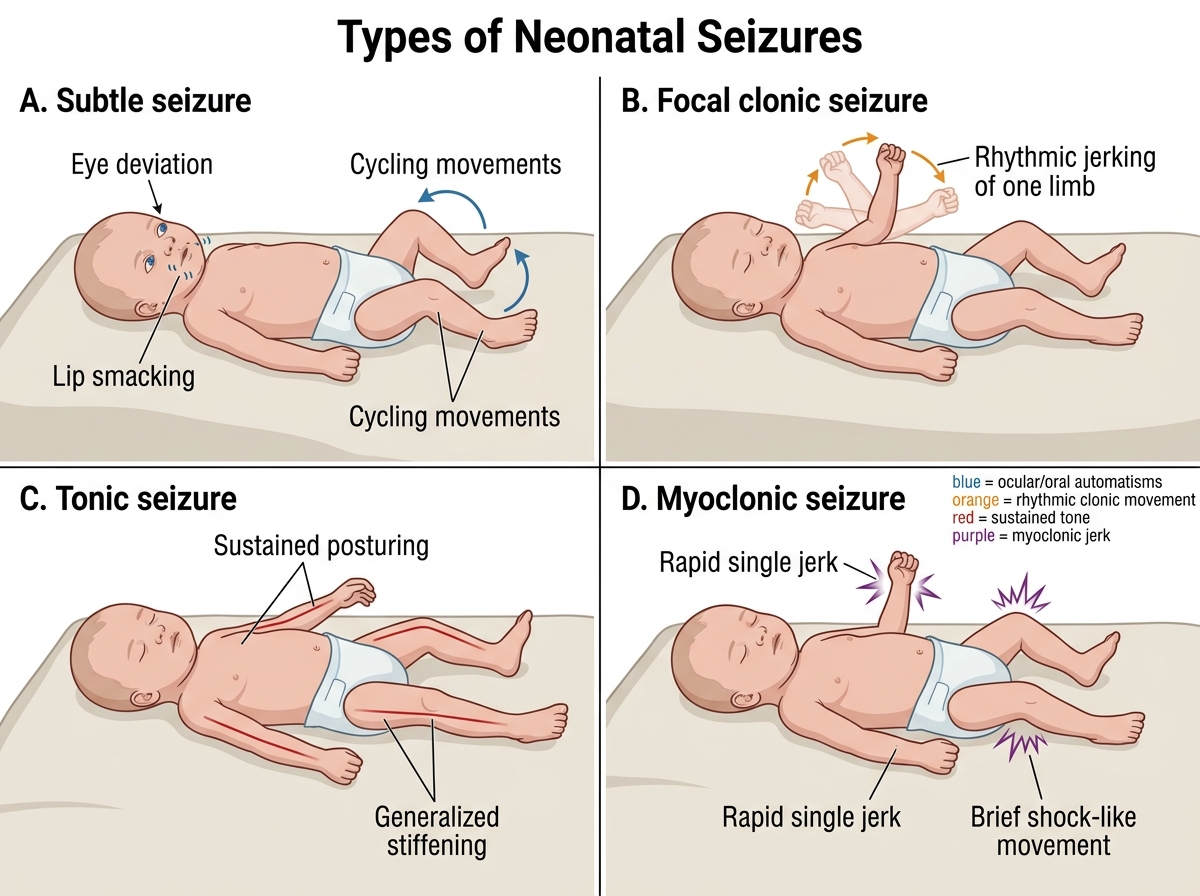
Four Types of Neonatal Seizures
Aetiology and Pathophysiology
The aetiology of neonatal seizures varies by gestational age and by postnatal timing. In term neonates, hypoxic-ischaemic encephalopathy (HIE) is overwhelmingly the most common cause, accounting for approximately 50–60% of all neonatal seizures. In very preterm neonates, intraventricular haemorrhage (IVH) and periventricular leukomalacia (PVL) become prominent. A structured aetiological classification is essential because treatment of the underlying cause is both the first priority and often the most effective intervention — particularly for the metabolic causes that are rapidly and completely reversible.
The pathophysiology of HIE-related seizures illustrates the central mechanism: perinatal asphyxia causes reduced cerebral oxygen delivery → failure of the Na⁺/K⁺-ATPase pump (which requires ATP) → cellular depolarisation → massive release of glutamate → NMDA receptor activation → calcium influx into neurons → mitochondrial dysfunction and apoptotic cell death (excitotoxicity). This cascade begins during the hypoxic insult but paradoxically worsens during reperfusion ('secondary energy failure'), 6–48 hours after birth — this is the window that therapeutic hypothermia exploits.
The most important causes in order of approximate frequency are:
| Cause | Frequency | Onset | Key clue |
|---|---|---|---|
| Hypoxic-ischaemic encephalopathy (HIE) | ~50–60% | Day 1 | Asphyxia history; Apgar <7 at 5 min; meconium, abnormal CTG |
| Metabolic (hypoglycemia, hypocalcemia, hyponatraemia, hypomagnesaemia) | ~10–15% | Variable | Responds to metabolite correction; no structural lesion |
| Intracranial infections (bacterial meningitis, HSV encephalitis) | ~5–10% | Day 2–7 | Fever/hypothermia; CSF abnormal; consider HSV empirically |
| Intracranial haemorrhage/infarction (IVH, subdural, SAH, PAIS) | ~10–15% | Day 1–3 | Imaging; IVH common in preterm |
| Genetic/structural (cortical malformations, metabolic encephalopathies, pyridoxine dependency) | ~10–15% | Variable | Family history; refractory; pyridoxine trial |
| Drug withdrawal (maternal opioids, SSRIs, benzodiazepines) | Rare | Day 1–3 | Maternal medication history; exaggerated Moro |
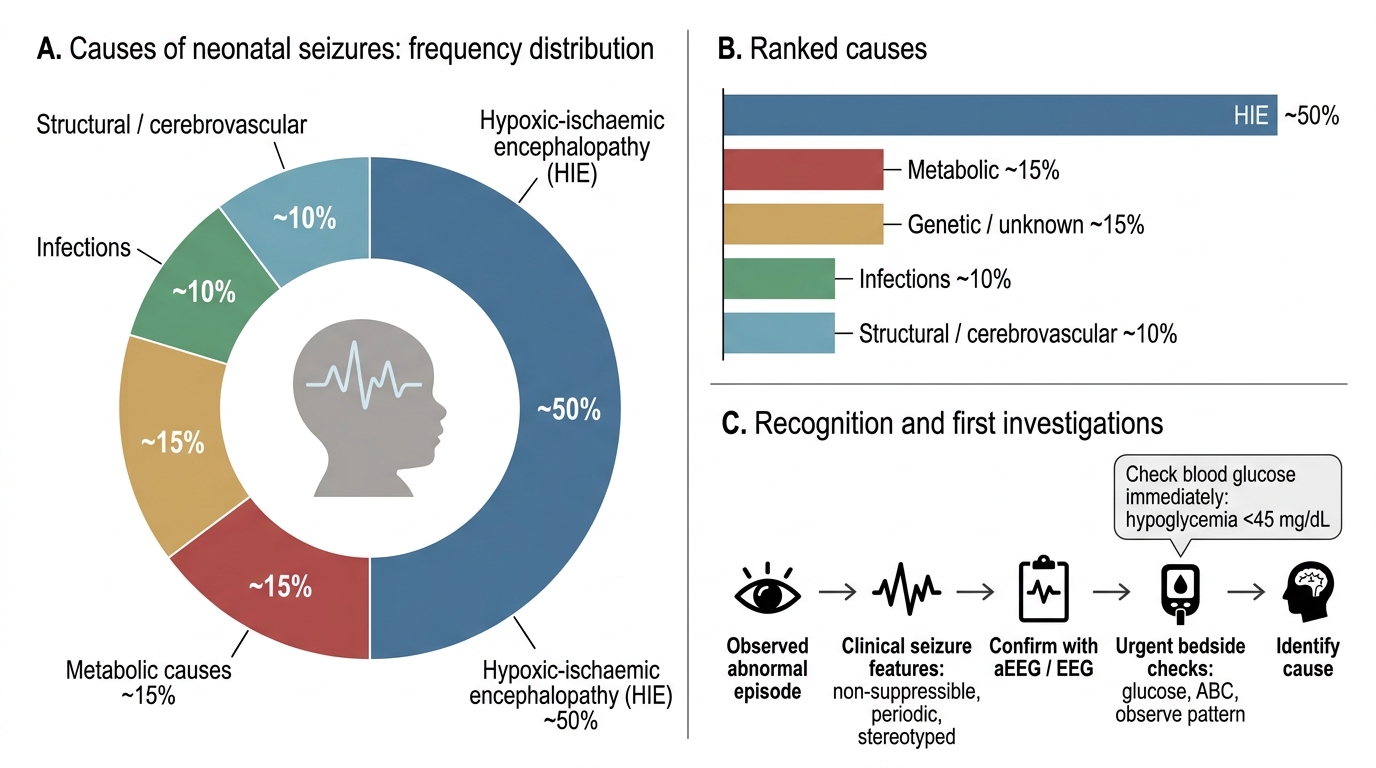
Frequency Distribution of Causes of Neonatal Seizures
Diagnosis: Clinical Recognition and Investigations
Diagnosing neonatal seizures is a two-step process: first, establishing that what is being observed is genuinely a seizure (clinical recognition supported by EEG), and second, identifying the underlying cause with a systematic investigation protocol. The clinical diagnosis rests on recognising the non-suppressibility, periodicity, and stereotypy of the episodes described in the previous section. However, up to 85% of electrographic seizures in neonates (particularly after antiepileptic drug loading) are subclinical — detectable only on EEG — making continuous amplitude-integrated EEG (aEEG) or standard multi-channel EEG an essential tool in any neonatal unit caring for at-risk babies. aEEG is the practical bedside tool in most Indian neonatal units; standard EEG is the gold standard for seizure confirmation and classification.
Urgent bedside assessment (within 5 minutes):
- Bedside blood glucose — exclude hypoglycemia (<45 mg/dL) immediately; this is the single most important and fastest reversible cause
- Airway, breathing, circulation — ensure oxygenation and haemodynamic stability
- Observe the episode: is it suppressible? Is there eye deviation? What is the motor pattern? What is the recurrence interval?
Urgent laboratory investigations (within 30 minutes):
- Blood glucose (glucometer + confirmatory serum)
- Serum electrolytes: sodium, calcium (total and ionised), magnesium, potassium
- Venous or arterial blood gas (pH, lactate — acidosis suggests HIE or metabolic disease)
- Full blood count and CRP/blood culture (if infection suspected)
- Serum ammonia and lactate if inborn error of metabolism is suspected
Neuroimaging:
- Cranial ultrasound (CUS) — first-line for preterm neonates; detects IVH, PVL, major malformations
- MRI brain (with diffusion-weighted imaging, DWI) — gold standard for detecting HIE injury pattern, arterial infarction, and cortical malformations; ideally performed at 3–5 days of age to capture the full extent of HIE injury
- CT brain — used acutely when MRI is unavailable; good for haemorrhage but radiation exposure
Lumbar puncture (LP): Mandatory if meningitis or HSV encephalitis is suspected (fever, CSF pleocytosis, vesicular rash). Do not defer LP due to seizures alone if the neonate is stable. HSV encephalitis requires empirical acyclovir until PCR results are available.
EEG/aEEG: Start continuous monitoring as soon as seizures are suspected. Background pattern (burst suppression, low voltage) is more prognostically important than seizure morphology in HIE.
SELF-CHECK
A 2-day-old term neonate has repetitive lip smacking and eye deviation episodes lasting 30 seconds, recurring every 8 minutes. Blood glucose is 52 mg/dL and serum calcium is 8.2 mg/dL. What is the correct first step in management?
A. Administer phenobarbitone 20 mg/kg IV immediately
B. Perform a lumbar puncture to exclude meningitis
C. Ensure airway patency and administer IV dextrose to correct metabolic cause
D. Order an urgent MRI brain to identify HIE
Reveal Answer
Answer: A. Administer phenobarbitone 20 mg/kg IV immediately
Wait — glucose 52 mg/dL (>45 mg/dL) and calcium 8.2 mg/dL (normal) mean the metabolic screen is normal. The clinical features — stereotyped, non-suppressible eye deviation and lip smacking in a neonate with a history of possible asphyxia — are consistent with subtle seizures from HIE. With metabolic causes excluded, phenobarbitone 20 mg/kg IV is the correct first-line antiepileptic intervention. LP is important but not the first step once metabolic causes are excluded and the baby is seizing. MRI is important later but not the immediate action.