Page 35 of 53
PE19.12 | Neonatal Seizures — SDL Guide (Part 2)
Management: Treat the Cause and AED Ladder
Management of neonatal seizures follows two simultaneous tracks: correcting any identifiable underlying cause (which may terminate the seizures without antiepileptic drugs), and escalating antiepileptic drug therapy if seizures persist. The most critical principle is that metabolic causes must be excluded and treated before or concurrent with AED loading — a baby whose seizures are caused by hypoglycemia will not respond to phenobarbitone, and the underlying brain injury from untreated hypoglycemia will continue during the AED trial.
Provided image
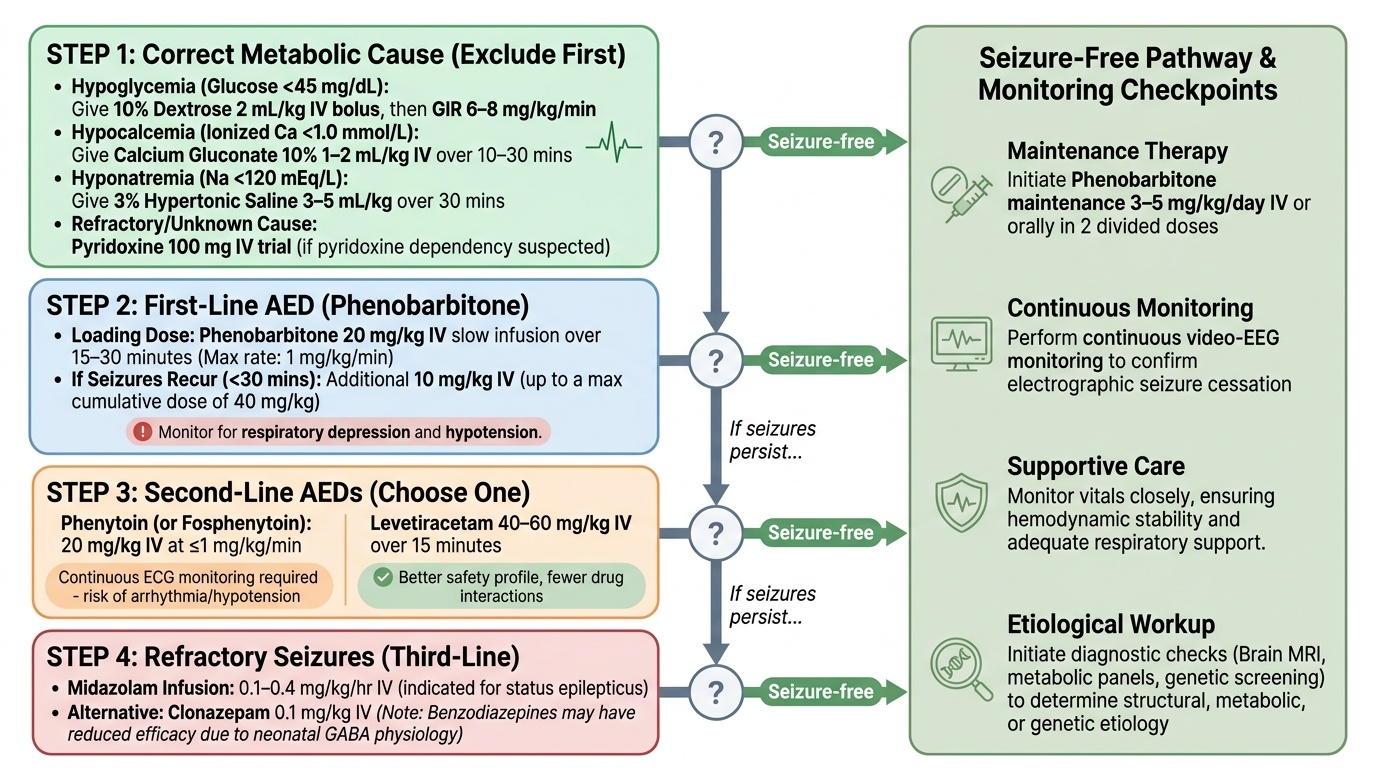
Step 0 — Correct the metabolic cause first:
If blood glucose <45 mg/dL: 10% dextrose 2 mL/kg IV bolus, then GIR 6–8 mg/kg/min (see Neonatal Hypoglycemia SDL).
If ionised calcium <1.0 mmol/L: calcium gluconate 10% 1–2 mL/kg IV over 10–30 minutes with ECG monitoring.
If hyponatraemia (Na <120 mEq/L) causing seizures: hypertonic saline 3% at 3–5 mL/kg over 30 minutes.
If pyridoxine dependency suspected (refractory seizures, no metabolic/structural cause): pyridoxine 100 mg IV trial.
Step 1 — First-line AED: Phenobarbitone
Phenobarbitone is the first-line antiepileptic drug for neonatal seizures in most international and Indian (NNF) guidelines. Loading dose: 20 mg/kg IV slow infusion over 15–30 minutes (maximum rate 1 mg/kg/min to avoid respiratory depression). If seizures recur within 30 minutes, an additional 10 mg/kg can be given, up to a total of 40 mg/kg. Phenobarbitone acts by potentiating GABA-A receptors and also has NMDA antagonist properties — important in neonates given their paradoxically excitatory GABA. Maintenance dose after loading: 3–5 mg/kg/day IV or orally in two divided doses. Monitor for respiratory depression and hypotension after loading.
Step 2 — Second-line AEDs (if seizures persist after maximum phenobarbitone):
- Phenytoin (or fosphenytoin, if available): 20 mg/kg IV at ≤1 mg/kg/min, with continuous ECG monitoring (risk of arrhythmia and hypotension); acts by blocking sodium channels
- Levetiracetam: 40–60 mg/kg IV over 15 minutes; increasingly used as second-line due to better safety profile and fewer drug interactions; mechanism involves SV2A synaptic vesicle protein modulation
Step 3 — Third-line / refractory seizures:
- Midazolam infusion: 0.1–0.4 mg/kg/hr; useful for status epilepticus
- Clonazepam: 0.1 mg/kg IV; note benzodiazepines may be less effective in neonates due to paradoxically excitatory GABA
- Lidocaine infusion: used in some centres for refractory neonatal seizures (limited evidence)
Therapeutic hypothermia for HIE:
For term neonates (≥36 weeks) with moderate-to-severe HIE, whole-body cooling to 33–34°C for 72 hours, started within 6 hours of birth, reduces mortality and neurodevelopmental disability (NNT approximately 7–9). Hypothermia also reduces seizure burden. It must be combined with continuous aEEG monitoring and seizure management with AEDs.
CLINICAL PEARL
Subtle seizures are the most dangerous because they are the most easily missed. The cycling limb movements, lip smacking, and eye deviation of neonatal subtle seizures are often dismissed as 'normal newborn behaviour' or 'jitteriness.' The distinguishing test is simple: gently restrain the moving limb — jitteriness stops; a seizure motor automatism does not. In a baby with a history of perinatal asphyxia, any stereotyped, recurrent, non-suppressible abnormal movement must be assumed to be a seizure until proved otherwise. Waiting for a 'classic' tonic-clonic seizure in a neonate will mean seizures are treated hours late — and every minute of uncontrolled seizure activity deepens excitotoxic neuronal injury.
Self-Assessment
Use these questions to test your integration of the clinical, investigative, and therapeutic aspects of neonatal seizures.
Q1. A 1-day-old term neonate with Apgar 5/8 has 10 episodes of lip smacking and eye deviation. Blood glucose is 58 mg/dL, serum calcium 8.5 mg/dL, sodium 138 mEq/L. What drug do you give first, and at what dose?
Answer: Phenobarbitone 20 mg/kg IV over 15–30 minutes. Metabolic causes have been excluded (glucose, calcium, sodium all normal). Phenobarbitone is the first-line AED. Do not start with benzodiazepines in neonates.
Q2. After 20 mg/kg phenobarbitone, seizures recur within 20 minutes. What is the next step?
Answer: Give a second dose of phenobarbitone 10 mg/kg IV (maximum cumulative dose 40 mg/kg). If seizures persist after maximum phenobarbitone, escalate to phenytoin 20 mg/kg IV or levetiracetam 40–60 mg/kg IV.
Q3. Which seizure type in neonates is most common and most easily confused with normal behaviour?
Answer: Subtle seizures — comprising eye deviation, lip smacking, cycling/swimming limb movements, and apnoea. They differ from jitteriness in being non-suppressible by restraint and lacking a stimulus-sensitive trigger.
Q4. A 36-week neonate with HIE is started on therapeutic hypothermia at 4 hours of age. Why is the 6-hour window critical?
Answer: The secondary energy failure phase of HIE (during which therapeutic hypothermia exerts its neuroprotective effect by slowing apoptotic cascades and reducing excitotoxic glutamate release) begins 6–48 hours after the primary insult. Hypothermia must be established before this window closes; after 6 hours, the neuroprotective benefit is lost.
SELF-CHECK
Why are benzodiazepines relatively less effective as first-line antiepileptic drugs in neonates compared to older children?
A. Neonates have immature hepatic metabolism and cannot break down benzodiazepines
B. GABA is paradoxically excitatory in neonates due to high intracellular chloride from NKCC1 transporter dominance
C. Benzodiazepines cross the blood-brain barrier poorly in the first week of life
D. Neonatal seizures are driven by dopamine excess, not GABA deficiency
Reveal Answer
Answer: B. GABA is paradoxically excitatory in neonates due to high intracellular chloride from NKCC1 transporter dominance
In neonates, the NKCC1 chloride cotransporter is more active than KCC2, maintaining high intracellular chloride. When GABA-A channels open (in response to benzodiazepines), chloride flows OUT of the neuron (not in), causing depolarisation rather than hyperpolarisation — meaning GABA is excitatory, not inhibitory, in the immature nervous system. This is a fundamental difference from older children and explains why phenobarbitone (NMDA antagonist + GABA potentiator) is preferred as first-line over benzodiazepines in neonatal seizures. The NKCC1/KCC2 ratio gradually normalises over the first few weeks of postnatal life.