Page 1 of 53
PE19.{1,3} | Normal Newborn Care — SDL Guide
Learning Objectives
- Define common neonatal nomenclature and classify newborns by gestational age and birth weight
- Describe the physical characteristics and physiological transitions of a normal term neonate
- Perform and interpret an APGAR score, distinguishing it from Ballard and Silverman-Anderson scales
- Explain the routine care of a normal neonate at birth including cord care, vitamin K, immunisation, and thermal protection
- Counsel caregivers on breastfeeding, growth monitoring, follow-up schedule, and red flag signs requiring urgent review
INSTRUCTIONS
Neonatal care sits at the intersection of obstetrics, paediatrics, and public health. India's neonatal mortality rate, though declining, remains one of the highest contributors to under-5 mortality. The first 28 days of life — and especially the first 24 hours — determine survival and long-term neurodevelopmental outcome. A final-year MBBS student will encounter newborns in the labour room, postnatal ward, and community health settings. Mastering normal newborn assessment is the prerequisite for recognising what is abnormal, deciding who needs resuscitation, and counselling parents about safe home care. This module builds from nomenclature and classification through physiology, hands-on care protocols, and the follow-up red flags that can prevent avoidable neonatal deaths.
References
- Ghai Essential Pediatrics, 9th ed., Ch 6 — Neonatology (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch 119-120 — The Newborn Infant (textbook)
- National Immunization Schedule, Ministry of Health & Family Welfare, India, 2023 (guideline)
- WHO/UNICEF Baby-Friendly Hospital Initiative (BFHI), 2018 revised (guideline)
- IAP National Neonatology Forum — Essential Newborn Care Guidelines (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old primigravida delivers a full-term baby at 39 weeks after an uncomplicated vaginal birth. The delivery team hands you the baby. The infant is crying vigorously, moving all four limbs, and turns pink within seconds. The paediatric resident at your side tells you to assign an APGAR score and prepare for the routine newborn care bundle — vitamin K, cord care, eye prophylaxis, and the birth-dose vaccines. You have five minutes before the mother asks to hold her baby and begin feeding. What is the score? What does it tell you? And what are the next ten things you must do to give this newborn the best possible start?
WHY THIS MATTERS
India accounts for approximately 18% of global neonatal deaths, with roughly 500,000 neonates dying each year. Nearly half of these deaths occur in the first 24 hours of life and are attributable to birth asphyxia, infection, and preterm complications — conditions whose outcomes are dramatically altered by timely, correct immediate newborn care. The knowledge and skills in this module are deployed every single day by every doctor who works in a labour room or postnatal ward, regardless of specialty. Misidentifying a normal variant as a pathological sign leads to unnecessary investigations; missing a true red flag leads to preventable deaths. The foundation competencies here — classification, APGAR, and care protocols — are also the gateway to understanding neonatal resuscitation, respiratory distress, and birth asphyxia, which follow in this cluster.
RECALL
Before engaging with this module, activate the following prior knowledge from your pre-clinical years. From Physiology (PY): recall fetal circulation, specifically the roles of the foramen ovale, ductus arteriosus, and ductus venosus — all three close or functionally change at birth, and understanding why the newborn turns pink relates directly to this transition. From Biochemistry (BI): recall neonatal glucose metabolism and why neonates — especially small-for-gestational-age infants — are prone to hypoglycaemia. From your Obstetrics posting: recall the stages of labour, the active management of the third stage, and why the Apgar score is assessed at 1 minute AND 5 minutes. Finally, from your community medicine exposure: be aware that India's National Immunization Schedule (NIS) — not the Western ACIP schedule — defines what vaccines are given at birth in Indian hospitals.
Clinical Context: Why Every Doctor Must Know the Normal Newborn
The neonatal period is defined as the first 28 days of life, with the early neonatal period comprising the first 7 days and the late neonatal period spanning days 8 to 28. This 28-day window carries the highest mortality risk of any comparable age interval in human life. Globally, approximately 2.4 million neonates die each year; in India, neonatal deaths account for nearly 70% of infant mortality. The leading causes are preterm birth complications, birth asphyxia, and sepsis — a triad directly influenced by the quality of care in the first hours after delivery.

Provided image
The relevance for a final-year MBBS student is immediate and practical. You will be called upon to assess a newborn in the delivery room, decide whether resuscitation is needed, initiate the care bundle, and counsel parents about what is normal and what demands urgent review. A doctor who cannot distinguish a normal newborn from a high-risk one cannot triage effectively. Understanding the normal baseline — what a healthy term neonate looks like, how it behaves, what its vital signs are — is the prerequisite for detecting every deviation from it.
In India, the National Health Mission (NHM) has made neonatal care a flagship priority. Janani Suraksha Yojana (JSY) incentivises institutional delivery to ensure skilled attendance at birth. Home-Based Newborn Care (HBNC) by Accredited Social Health Activists (ASHAs) provides post-discharge follow-up visits in the community. Knowing these programme structures helps you integrate individual clinical care with the population-level system designed to support it.
- The neonatal period = first 28 days; early neonatal = days 0–7; late neonatal = days 8–28
- India's neonatal mortality rate (NMR) ≈ 20 per 1,000 live births (SRS 2020); target <12 by 2030
- Top three causes: preterm complications, birth asphyxia, neonatal sepsis
- National programmes: JSY (institutional delivery), SNCU (Sick Newborn Care Units), HBNC (ASHA visits)
Neonatal Nomenclature and Classification
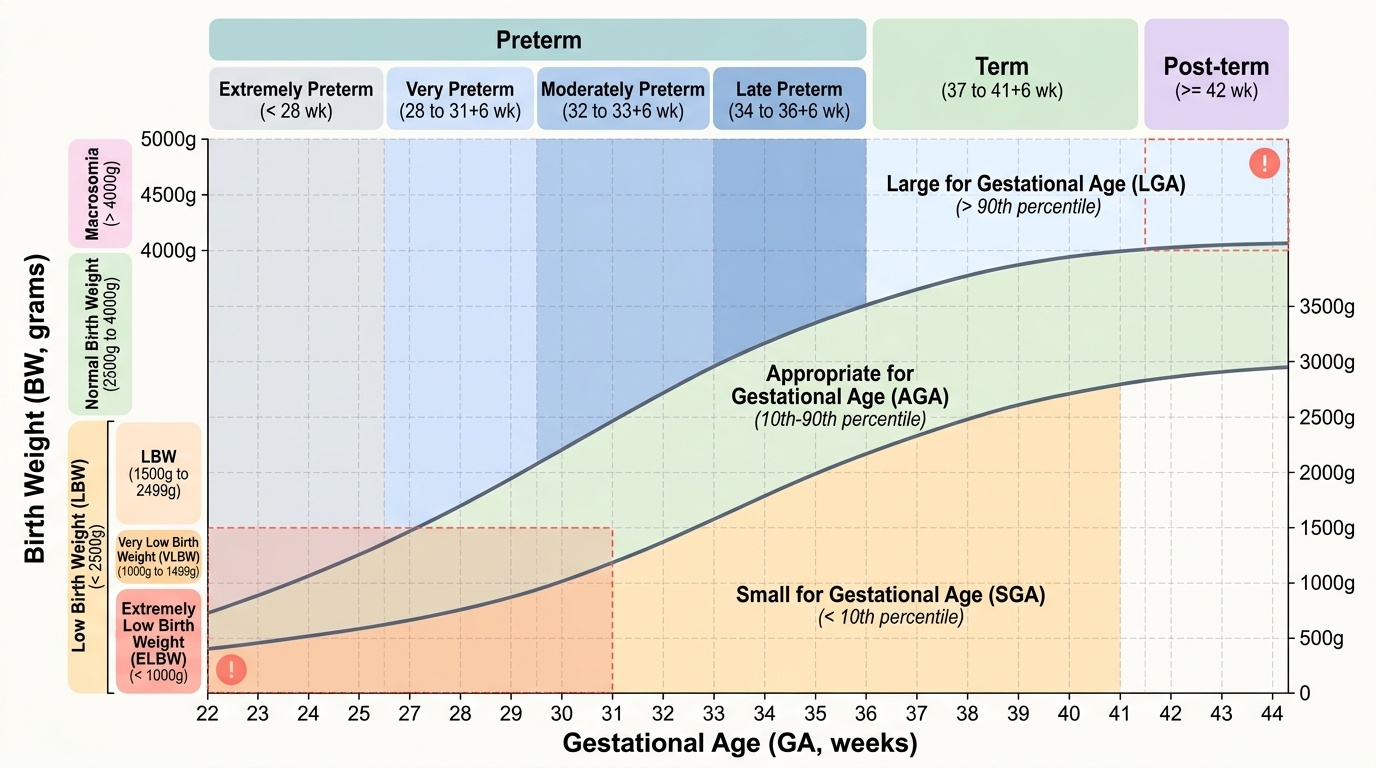
Precise neonatal nomenclature prevents clinical miscommunication and drives risk stratification. Neonates are classified simultaneously by two independent axes: gestational age (GA) at birth and birth weight (BW). These two variables are not perfectly correlated, and their mismatch generates clinically distinct high-risk groups.
Provided image
Classification by gestational age uses the last menstrual period, antenatal ultrasound, or postnatal Ballard scoring (a separate scoring system for gestational maturity — not to be confused with APGAR, which assesses immediate condition). A term neonate is born at 37+0 to 41+6 weeks; a preterm neonate before 37 complete weeks; a post-term neonate at 42 weeks or beyond. Preterm is further sub-classified: late preterm (34–36+6 wk), moderately preterm (32–33+6 wk), very preterm (28–31+6 wk), and extremely preterm (<28 wk). Each sub-class carries a distinct mortality and morbidity profile.
Classification by birth weight proceeds as follows: normal birth weight is 2,500–4,000 g. Low birth weight (LBW) is defined as birth weight <2,500 g, regardless of gestational age. Within LBW, very low birth weight (VLBW) is <1,500 g and extremely low birth weight (ELBW) is <1,000 g. A birth weight >4,000 g constitutes macrosomia, associated with maternal diabetes and birth trauma risk.
Weight for gestational age adds a third dimension: a neonate's birth weight is plotted against GA on a growth chart. Appropriate for gestational age (AGA) means weight between the 10th and 90th centiles for GA. Small for gestational age (SGA) means weight below the 10th centile — suggesting intrauterine growth restriction (IUGR) and carrying risks of hypoglycaemia, polycythaemia, and poor thermoregulation. Large for gestational age (LGA) means weight above the 90th centile — associated with maternal diabetes and shoulder dystocia risk.
High-risk neonates include: preterm, LBW/VLBW/ELBW, SGA, LGA, post-term, and those born to mothers with diabetes, hypertension, infections, or substance use. These groups require enhanced monitoring beyond routine newborn care.
| Axis | Category | Definition |
|---|---|---|
| Gestational age | Extremely preterm | <28 weeks |
| | Very preterm | 28–31+6 weeks |
| | Moderately preterm | 32–33+6 weeks |
| | Late preterm | 34–36+6 weeks |
| | Term | 37–41+6 weeks |
| | Post-term | ≥42 weeks |
| Birth weight | ELBW | <1,000 g |
| | VLBW | <1,500 g |
| | LBW | <2,500 g |
| | Normal BW | 2,500–4,000 g |
| | Macrosomia | >4,000 g |
| Weight for GA | SGA | <10th centile |
| | AGA | 10th–90th centile |
| | LGA | >90th centile |
Physical Characteristics of the Normal Term Neonate
The physical examination of a normal term neonate is both a clinical assessment and a systematic process of cataloguing normal variants — findings that alarm parents but require no intervention. Recognising these normal variants prevents unnecessary investigations and reassures families.
Anthropometry: average birth weight 2,800–3,500 g (males slightly heavier than females); crown-heel length 48–52 cm; head circumference (HC) 33–35 cm. The head circumference slightly exceeds the chest circumference (CC) at birth (HC > CC); this relationship reverses by 6 months of age. Physiological weight loss of up to 10% of birth weight in the first 3–4 days is normal due to passage of meconium, loss of vernix and fluid; birth weight should be regained by day 10–14. Weight loss exceeding 10% or failure to regain by day 14 is pathological.
Head and face: the skull of a neonate is composed of bones separated by sutures (fibrous junctions) and fontanelles (membranous intersections). The anterior fontanelle (AF) is diamond-shaped, palpable at the junction of the coronal and sagittal sutures, and normally closes by 12–18 months. The posterior fontanelle (PF) is triangular and normally closes by 6–8 weeks. A bulging fontanelle suggests raised intracranial pressure; a sunken fontanelle indicates dehydration. Caput succedaneum (oedema of the scalp crossing suture lines, resolves in 24–48 h) and cephalhaematoma (subperiosteal blood, does not cross suture lines, resolves in weeks) are common birth-related findings — distinguish them at the bedside.
Skin: vernix caseosa (white cheesy coating) protects the skin in utero and is normal at term; lanugo (fine hair) is more prominent in preterm neonates. Milia (tiny white epidermal cysts on the nose and face), Epstein pearls (on the hard palate), and erythema toxicum (blotchy erythematous patches with white centres, appearing days 1–3, benign) are all normal. Mongolian blue spots (blue-grey patches over the lumbosacral region, more common in darker-skinned infants) are benign and fade over years. Neonatal jaundice appearing after 24 hours and peaking day 3–5 may be physiological; jaundice within 24 hours is always pathological.
Neonatal reflexes test neurological integrity and disappear at predictable ages:
- Moro reflex (startle): extends arms then flexes; present 0–4 months
- Rooting reflex (turns head toward touch on cheek): 0–4 months
- Sucking reflex: 0–4 months
- Palmar/plantar grasp: 0–3–4 months
- Stepping reflex: 0–2 months
- Babinski sign (plantar fanning): normal in neonates, abnormal after 2 years
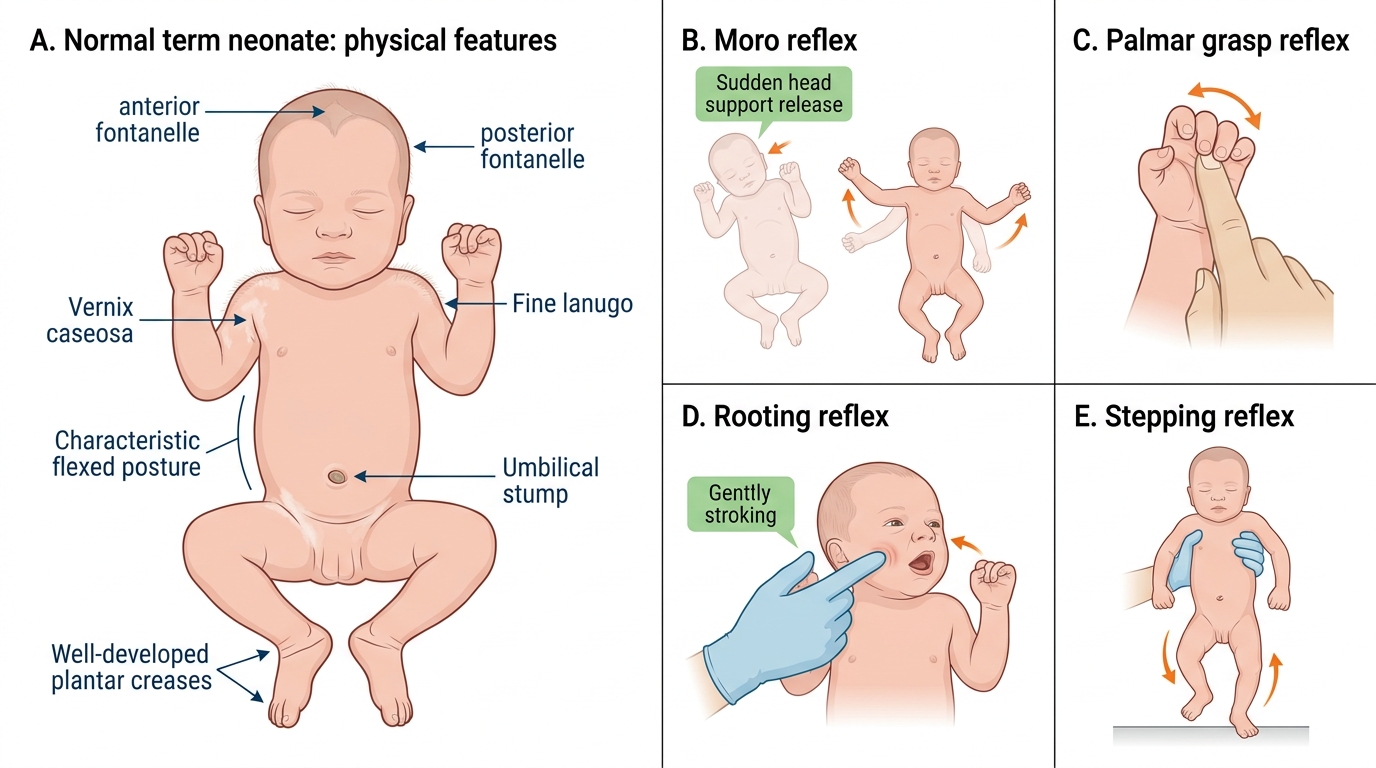
Normal Term Neonate: Physical Features and Reflexes