Page 2 of 53
PE19.{1,3} | Normal Newborn Care — SDL Guide (Part 2)
APGAR Score and Immediate Newborn Assessment
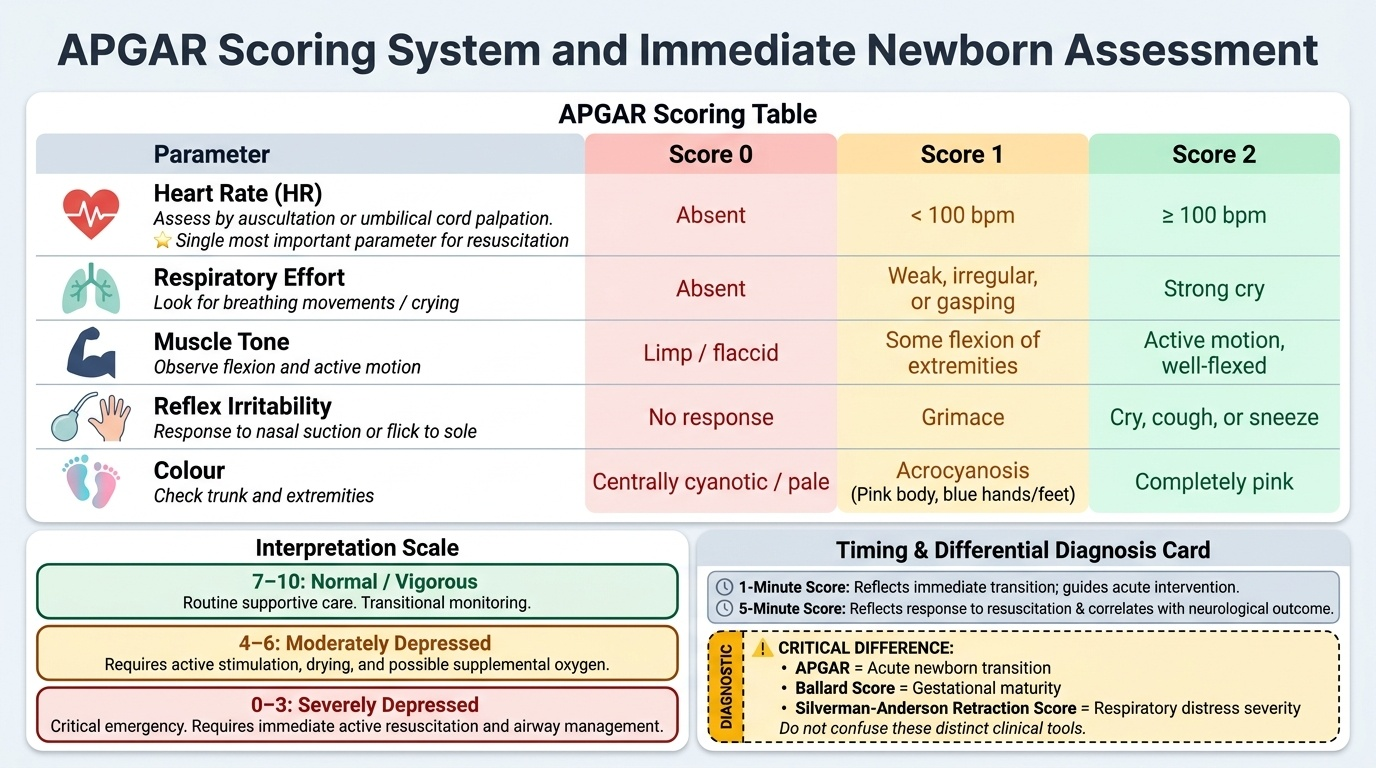
The APGAR score (devised by Dr Virginia Apgar in 1952) is a standardised, rapid assessment tool that evaluates the immediate condition of a newborn at 1 minute and 5 minutes after birth. It is critically important to remember that the APGAR is NOT a measure of gestational maturity (that is the Ballard/New Ballard Score) and NOT a measure of respiratory distress severity (that is the Silverman-Anderson Retraction Score). These three scoring systems serve entirely different clinical purposes and must not be confused. The APGAR score was initially designed to standardise the decision to intervene in the delivery room — to shift newborn assessment from an ad hoc clinical impression to a reproducible, numeric scale that any trained person could apply. Its genius is its simplicity: five observable parameters, each scored 0, 1, or 2, with no equipment beyond a stethoscope and a clock. The score is not a substitute for clinical judgment, nor does a normal APGAR guarantee absence of subtle neurological injury — but it is the universally adopted communication tool for conveying the condition of a newborn to any receiving team, anywhere in the world.
Provided image
The APGAR score evaluates five physiological parameters, each scored 0, 1, or 2, giving a maximum score of 10:
- Heart Rate (HR): Absent = 0; <100 bpm = 1; ≥100 bpm = 2. Heart rate is assessed by auscultation or palpation of the umbilical cord. It is the single most important APGAR parameter for deciding resuscitation.
- Respiratory effort: Absent = 0; weak/irregular/gasping = 1; strong cry = 2.
- Muscle tone: Limp/flaccid = 0; some flexion of extremities = 1; active motion, well-flexed = 2.
- Reflex irritability (response to stimulation, e.g., suction catheter in nose or flick to sole): No response = 0; grimace = 1; cry/cough/sneeze = 2.
- Colour: Centrally cyanotic/pale = 0; acrocyanosis (blue hands and feet, pink body) = 1; completely pink = 2.
Interpretation: Total score ≥7 = normal/vigorous; 4–6 = moderate depression (requires stimulation, possible supplemental oxygen); ≤3 = severe depression (requires immediate resuscitation). The 1-minute score reflects the neonate's condition at the time of delivery and guides immediate intervention. The 5-minute score reflects response to resuscitation and correlates with neurological outcome. If the 5-minute score is <7, assessment continues every 5 minutes up to 20 minutes.
Important distinction — Ballard Score: The New Ballard Score estimates gestational age by assessing six neuromuscular maturity signs (posture, square window, arm recoil, popliteal angle, scarf sign, heel-to-ear) and six physical maturity signs (skin, lanugo, plantar surface, breast, eye/ear, genitals), each scored 0–5. It is used postnatally when GA is uncertain. It has nothing to do with the neonate's immediate condition.
Important distinction — Silverman-Anderson Retraction Score: This scoring system assesses the severity of respiratory distress in a neonate. Five parameters — upper chest retraction, lower chest retraction, xiphoid retraction, nares dilatation, and expiratory grunt — are each scored 0, 1, or 2. A score of 0 = no respiratory distress; ≥7 = severe distress. It is used to monitor respiratory distress syndrome or other causes of neonatal respiratory compromise — not to assess the immediate post-birth condition.
SELF-CHECK
A neonate at 1 minute of life has a heart rate of 88 bpm, weak respiratory effort, good muscle tone, grimace on stimulation, and acrocyanosis. What is the APGAR score?
A. 5
B. 6
C. 7
D. 8
Reveal Answer
Answer: B. 6
Score each parameter: HR 88 bpm (<100) = 1; weak respiratory effort = 1; good muscle tone = 2; grimace = 1; acrocyanosis = 1. Total = 6. This is moderate neonatal depression. The most important signal here is the HR below 100 bpm — stimulation should begin immediately and response monitored at 5 minutes.
Neonatal Physiology — Transition from Fetal to Extrauterine Life
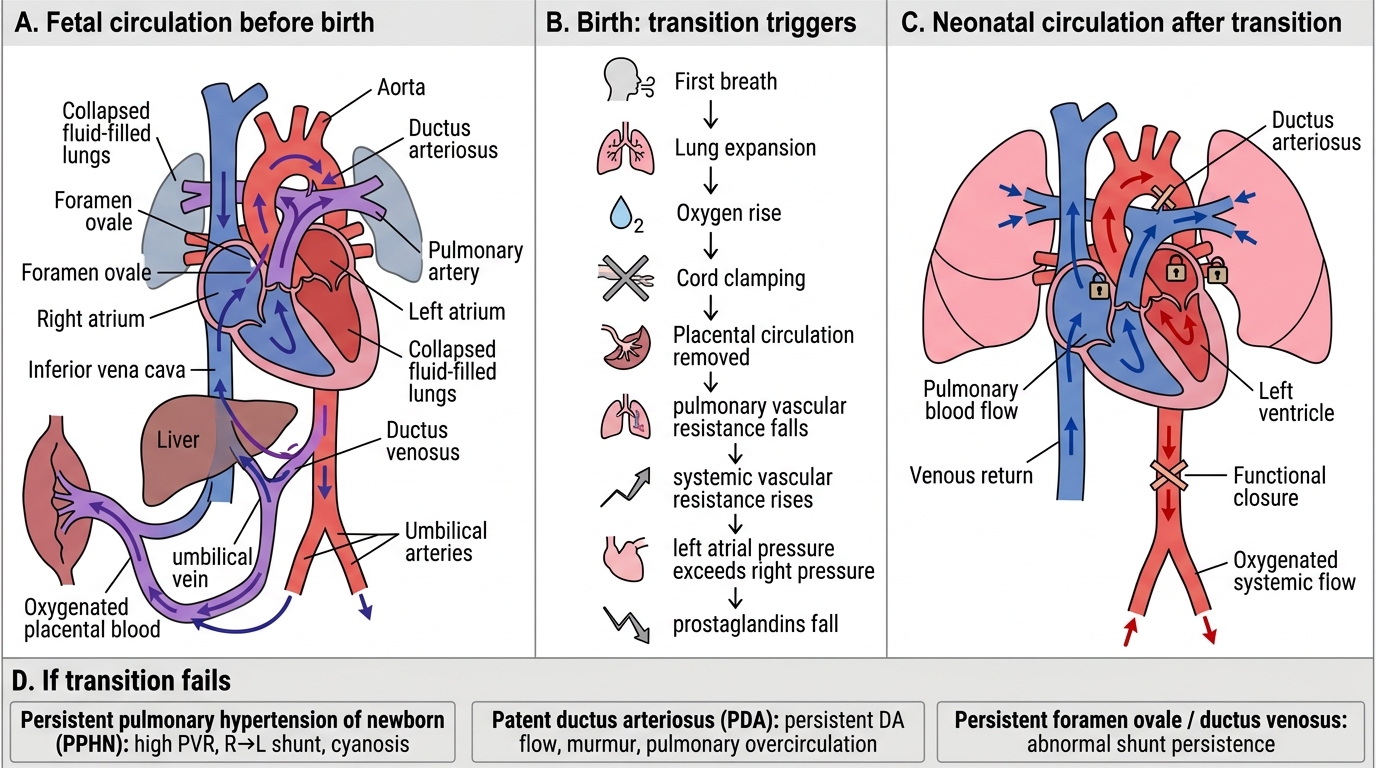
Birth triggers the most dramatic physiological transition in human life. Within seconds to minutes, the neonate must switch from fetal physiology (umbilical gas exchange, low-resistance placental circulation, fluid-filled lungs) to neonatal physiology (pulmonary respiration, independent thermoregulation, enteral nutrition). Understanding this transition clarifies why normal newborns behave the way they do and why high-risk neonates fail specific transitions.
Cardiovascular transition: In fetal circulation, oxygenated blood from the placenta bypasses the lungs through three fetal shunts: the foramen ovale (right-to-left atrial shunt), the ductus arteriosus (pulmonary artery to aorta), and the ductus venosus (umbilical vein to inferior vena cava). At birth, lung expansion causes a dramatic fall in pulmonary vascular resistance (PVR), while systemic vascular resistance (SVR) rises with clamping of the umbilical cord. The resulting pressure reversal closes the foramen ovale functionally within minutes (anatomical fusion over weeks–months) and causes the ductus arteriosus to constrict in response to rising oxygen tension. Failure of these closures results in persistent fetal circulation (PFC) or persistent pulmonary hypertension of the newborn (PPHN), clinically manifesting as severe hypoxia unresponsive to oxygen alone.
Respiratory transition: The fetal lung contains approximately 30 mL/kg of fluid. During vaginal delivery, thoracic compression expels roughly a third of this fluid; the remainder is absorbed by pulmonary lymphatics and capillaries over the first few hours. The first breath requires a large negative inspiratory pressure (−40 to −70 cm H₂O) to overcome surface tension. Surfactant (dipalmitoyl phosphatidylcholine, produced by type II pneumocytes from ≈34 weeks GA) dramatically lowers alveolar surface tension and prevents alveolar collapse at end-expiration. Surfactant deficiency in premature neonates causes respiratory distress syndrome (RDS) — the subject of a separate SDL in this cluster.
Thermoregulation: Neonates have a large surface area-to-body mass ratio, thin subcutaneous fat, and immature vasomotor control — making them exquisitely prone to cold stress. The primary mechanism of neonatal heat production is non-shivering thermogenesis via brown adipose tissue (BAT), located in the nape of the neck, interscapular region, and around the kidneys and adrenals. Neonates cannot shiver effectively. Hypothermia (<36.5°C axillary) increases metabolic rate, oxygen consumption, and glucose demand, contributing to hypoxia and hypoglycaemia. The prevention hierarchy is: dry immediately, warm the environment, skin-to-skin contact (Kangaroo Mother Care for LBW), and delay bathing (at least 6 hours per WHO guidelines, 24 hours preferred).
Metabolic and hepatic transition: Fetal glucose is supplied by the placenta; at birth, this supply stops abruptly. The neonate must activate gluconeogenesis and glycogenolysis. Term AGA neonates handle this transition well if breastfed promptly. Preterm, SGA, LGA (infant of diabetic mother), and asphyxiated neonates are at higher risk of neonatal hypoglycaemia (blood glucose <2.6 mmol/L or <47 mg/dL by WHO criteria in symptomatic neonates). Unconjugated bilirubin rises physiologically as fetal haemoglobin (HbF) is broken down and the immature neonatal liver cannot conjugate it efficiently — the mechanism behind physiological neonatal jaundice.
Neonatal Cardiovascular Transition at Birth
| System | Fetal state | Neonatal transition | Clinical consequence if fails |
|---|---|---|---|
| Cardiovascular | R→L shunts via FO + DA | FO/DA close, PVR falls | PPHN, cyanosis |
| Respiratory | Lung fluid-filled | Fluid absorbed, surfactant activates | RDS if preterm |
| Thermoregulation | Placenta maintains temp | BAT thermogenesis | Cold stress → hypoglycaemia |
| Metabolic | Placental glucose supply | Gluconeogenesis + glycogenolysis | Neonatal hypoglycaemia |
Breastfeeding and Nutritional Care of the Neonate
Breastfeeding is the single most effective preventive health intervention for the neonate. Exclusive breastfeeding (EBF) — defined as giving no food or liquid other than breast milk (and permitted medicines) for the first 6 months — reduces neonatal mortality by up to 45% in low-income settings (WHO/UNICEF data). In India, the Mother's Absolute Affection (MAA) programme under NHM promotes early initiation (within one hour of birth) and EBF through counselling and community support. The importance of this recommendation cannot be overstated: breast milk is not merely nutrition; it is a complex, living biological fluid that adapts daily to the infant's needs and provides immunological protection that no formula can replicate. In a country where gastrointestinal infections and pneumonia remain major causes of infant death, the secretory IgA in breast milk coats the gut epithelium and represents the neonate's first line of external immune protection before its own adaptive immune system matures. For a clinician, the practical implication is that every interaction with a new mother — in the postnatal ward, at the 6-week visit, or in the community — is an opportunity to reinforce, troubleshoot, or rescue a breastfeeding pair. Failure to breastfeed exclusively in the first 6 months is associated with a doubled risk of hospitalisation for respiratory and gastrointestinal illness in the first year of life.
Breast milk composition evolves in three stages:
1. Colostrum (days 1–5): thick, yellowish, low in volume (2–20 mL per feed) but extraordinarily rich in secretory IgA, lactoferrin, leukocytes, and growth factors. Colostrum is the neonate's first immunisation — it coats the gut mucosa and prevents colonisation by pathogens. It is also a mild laxative that promotes passage of meconium. Do not advise pre-lacteal feeds (honey, water, formula) — these displace colostrum.
2. Transitional milk (days 5–14): volume increases, fat content rises.
3. Mature milk (after day 14): fore-milk (watery, satisfies thirst) and hind-milk (fat-rich, provides calories). The infant must empty one breast before switching to ensure adequate caloric intake from hind-milk.
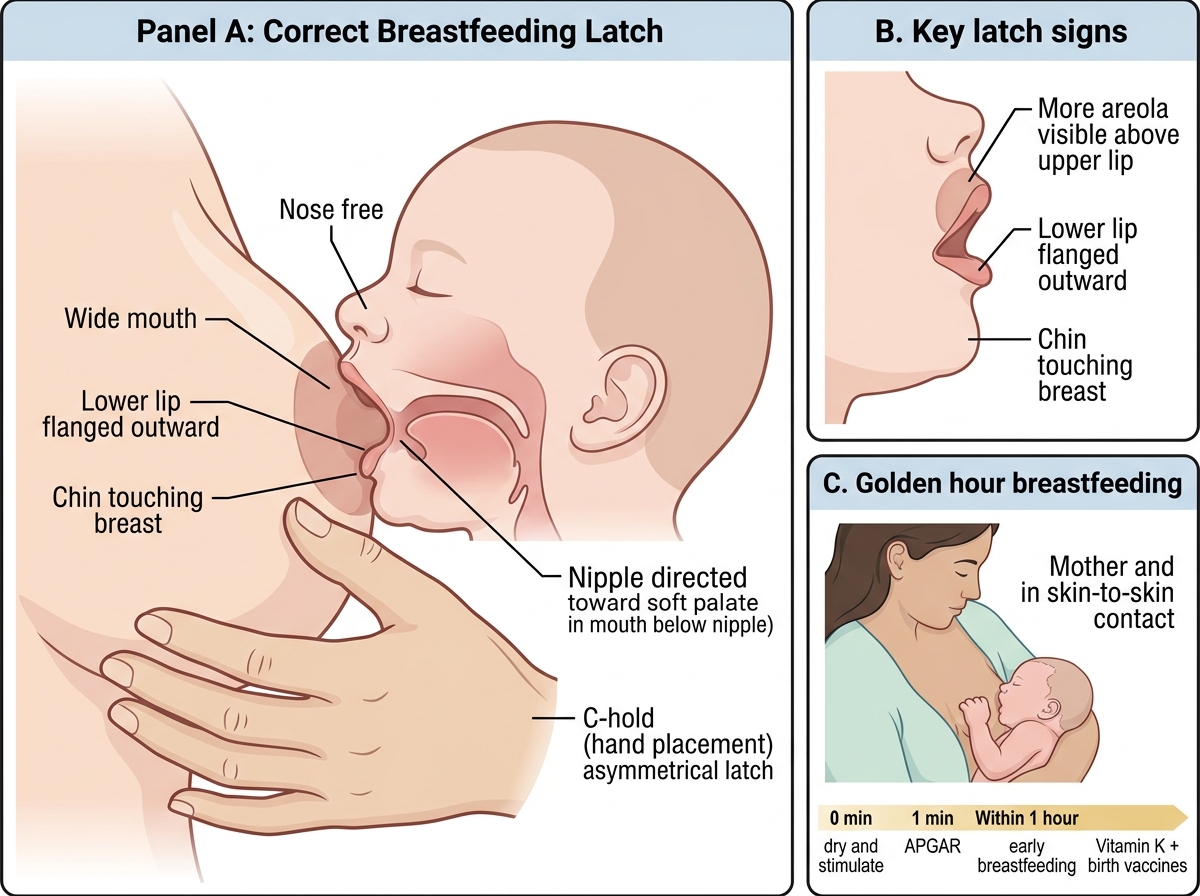
Correct breastfeeding technique is essential for effectiveness and to prevent complications (cracked nipples, engorgement, mastitis):
- Position: cradle, cross-cradle, football, or side-lying — all acceptable if comfortable
- Latch (the most common site of failure): the infant's mouth should cover most of the areola (not just the nipple); the lower lip should be flanged outward; chin should touch the breast
- Feeding frequency: demand feeding — typically 8–12 times per 24 hours in the first weeks; the newborn's stomach capacity is ~5–7 mL at birth, expanding to ~50 mL by day 10
- Signs of adequate intake: 6–8 wet nappies per day after day 4; passage of stools; weight gain after the initial physiological loss
Baby-Friendly Hospital Initiative (BFHI) by WHO/UNICEF promotes Ten Steps to Successful Breastfeeding in hospitals, including rooming-in (mother and baby in same room 24 hours) and no supplementation without medical indication.
Vitamin D and iron supplementation: exclusively breastfed term infants should receive Vitamin D 400 IU/day from birth (IAP recommendation 2021) as breast milk alone is insufficient. Preterm and LBW infants require additional iron supplementation from 2 weeks of age (2–4 mg/kg/day elemental iron) under NHM guidelines.
Correct Breastfeeding Latch and Golden Hour Care
CLINICAL PEARL
The 'golden hour' of newborn care is the first 60 minutes after birth. In this window: dry and stimulate immediately (within 30 seconds), assign APGAR at 1 minute, initiate skin-to-skin contact, begin early breastfeeding within the first hour, give vitamin K 1 mg IM, administer birth-dose vaccines (BCG, OPV-0, Hep-B), and apply cord care. Research shows that initiating breastfeeding within one hour of birth reduces neonatal mortality by up to 22%. A neonate placed skin-to-skin on the mother's chest maintains temperature better than a warmer in a healthy dyad. The single most important axiomatic rule of neonatal care: DRY → WARM → ASSESS → ACT — in that order. A wet, cold neonate cannot be accurately assessed, because cold stress activates survival physiology that mimics distress.