Page 3 of 53
PE19.{1,3} | Normal Newborn Care — SDL Guide (Part 3)
Routine Care and Procedures at Birth
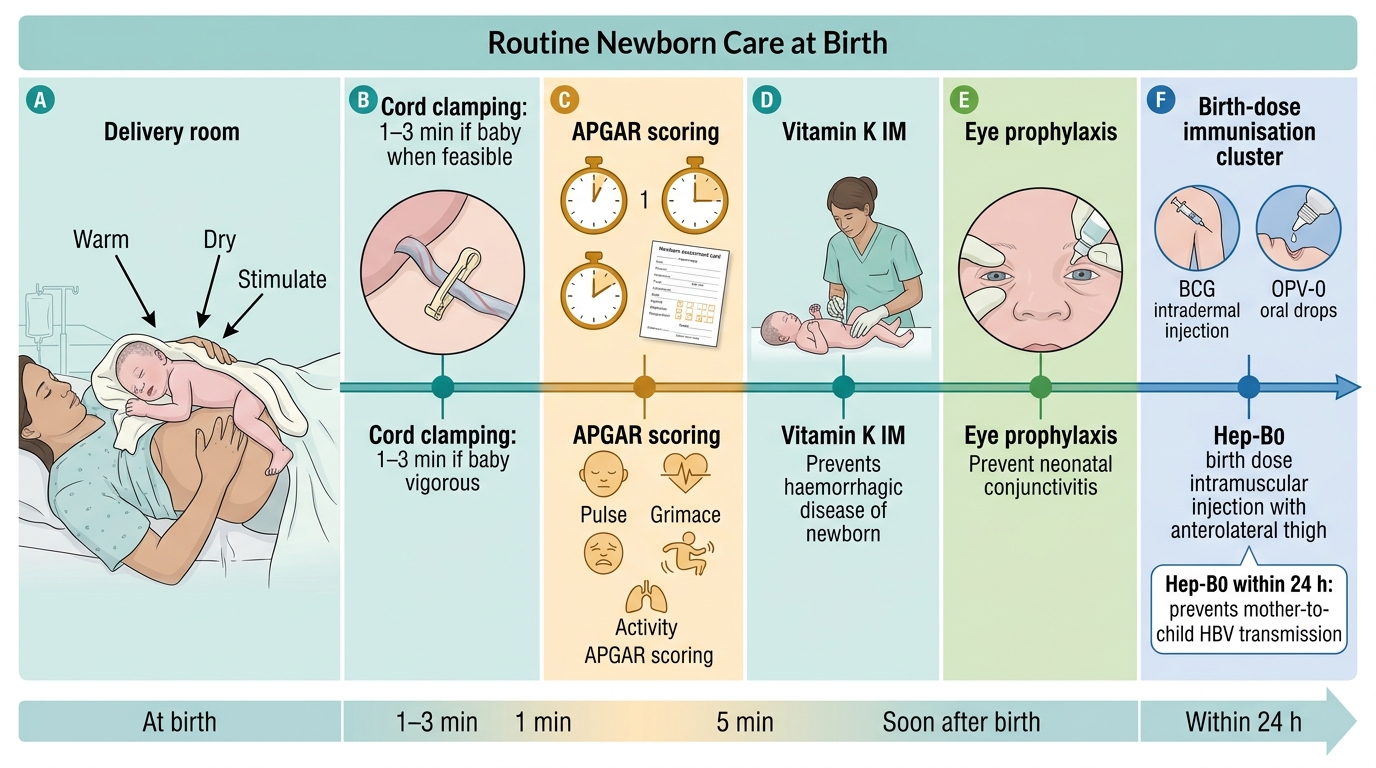
Routine newborn care at birth follows a defined bundle of evidence-based interventions that together constitute the Essential Newborn Care (ENC) protocol — the standard of care in India's institutional delivery settings under the National Health Mission. Every element of this bundle addresses a specific physiological vulnerability of the neonate: the risk of hypothermia from evaporative cooling, the risk of haemorrhagic disease from vitamin K deficiency, the risk of gonococcal blindness from birth-canal pathogens, and the risk of chronic hepatitis B from maternal transmission. Understanding not just what to do but why each intervention exists transforms a checklist into a clinical reasoning exercise. The ENC protocol is designed to be completed within the first 60 minutes — the golden hour — when the neonate is transitioning from fetal to extrauterine physiology and is most susceptible to iatrogenic harm from omission. In busy Indian labour rooms, where a single nurse or junior doctor may manage multiple deliveries simultaneously, a systematic mental checklist anchored to the protocol prevents life-threatening omissions. Each step has a defined timing, route, site, and dose — and examiners routinely test these specifics.
Immediate steps (within the first minute — the 'golden minute'):
- Dry the baby immediately with a warm, clean cloth; this stimulates breathing and prevents evaporative heat loss
- Keep warm — place under a radiant warmer or on the mother's chest (skin-to-skin)
- Clear the airway only if secretions are visible and obstructing — routine suctioning is NOT recommended for vigorous neonates as it can cause vagal bradycardia
- Assess — crying? breathing? good tone? (the three rapid questions that decide if basic stabilisation or resuscitation is needed)
Cord care: Delayed cord clamping (DCC) for 60–180 seconds after birth increases iron stores and reduces anaemia in the neonate (WHO recommendation; NHM policy). Apply 0.7% chlorhexidine gel/solution to the cord stump in community/home-birth settings per NHM guidelines (reduces umbilical infection rates). In hospital settings, dry cord care (keeping the stump clean and dry, fold the nappy below the stump) is acceptable. Signs of omphalitis (redness, swelling, pus, fever) require urgent treatment with antibiotics.
Vitamin K₁ (phytomenadione): All neonates receive vitamin K₁ 1 mg IM into the anterolateral thigh within the first hour of birth. Neonates are born with low vitamin K stores because vitamin K crosses the placenta poorly, and gut bacteria (which synthesise vitamin K₂) have not yet colonised the neonatal gut. Without prophylaxis, neonates are at risk of Haemorrhagic Disease of the Newborn (HDN) — now termed Vitamin K Deficiency Bleeding (VKDB) — which can cause intracranial haemorrhage. Exclusively breastfed neonates are at higher risk (formula is vitamin K-fortified).
Eye prophylaxis: A single dose of 1% tetracycline eye ointment (or erythromycin 0.5% where available) is applied to both eyes at birth to prevent neonatal conjunctivitis (ophthalmia neonatorum), most critically that caused by Neisseria gonorrhoeae and Chlamydia trachomatis acquired during passage through an infected birth canal. Gonococcal ophthalmia, if untreated, causes corneal ulceration and blindness within days.
Birth-dose immunisation (per National Immunization Schedule, India):
- BCG (Bacillus Calmette-Guérin): 0.1 mL intradermal, left deltoid — protects against severe disseminated tuberculosis in the neonate
- OPV-0 (oral poliovirus vaccine birth dose): 2 drops oral — provides early mucosal immunity
- Hepatitis B (Hep-B₀): 0.5 mL IM, right anterolateral thigh — within 24 hours of birth, this birth dose is critical to interrupt mother-to-child transmission of HBV (perinatal transmission is the most common route of chronic HBV in Asia)
Temperature maintenance: Target axillary temperature is 36.5–37.5°C. Avoid over-wrapping (hyperthermia) and ensure the room temperature is adequate (≥25°C). For LBW/preterm stable neonates, Kangaroo Mother Care (KMC) — continuous skin-to-skin contact with the mother, the infant in upright position between her breasts — is WHO-recommended as superior to incubator care for stable neonates, improving temperature regulation, breastfeeding success, and neurodevelopmental outcomes.
Routine Newborn Care at Birth
SELF-CHECK
Which of the following immunisations is given at birth as part of the National Immunization Schedule (India) and is specifically aimed at preventing mother-to-child transmission?
A. BCG
B. Hepatitis B birth dose
C. OPV-0
D. Rotavirus
Reveal Answer
Answer: B. Hepatitis B birth dose
Hepatitis B birth dose (0.5 mL IM, within 24 hours of birth) is specifically designed to interrupt perinatal (mother-to-child) transmission of HBV, which is the most common mechanism of chronic hepatitis B in Asia. All three — BCG, OPV-0, and Hep-B₀ — are given at birth per the NIS, but only Hep-B₀ is primarily intended for transmission interruption from an infected mother. Rotavirus vaccine starts at 6 weeks, not at birth.
Follow-up, Growth Monitoring, and Red Flags
The postnatal period is not over when the mother and baby leave the hospital. The first two weeks of life require structured follow-up to catch late-onset infections, monitor weight gain, reinforce breastfeeding, and identify neonates who are deteriorating at home. Under India's HBNC (Home-Based Newborn Care) programme, ASHAs make scheduled visits on days 1, 3, 7, 14, 21, and 28 for home deliveries; for institutional deliveries, the first postnatal visit is recommended within 48–72 hours of discharge.
Normal neonatal weight trajectory: As established earlier, neonates normally lose up to 10% of birth weight in the first 3–4 days, then regain birth weight by day 10–14 and subsequently gain approximately 25–30 g per day (or ~180–210 g per week) in the first three months. Growth is plotted on WHO 2006 Child Growth Standards (India officially adopted these through IAP and the NHM in 2013). The key measurements are weight, length/height, and head circumference, ideally plotted at each visit.
Immunisation follow-up: After birth-dose vaccines, the next visit at 6 weeks initiates the primary immunisation series:
- Pentavalent vaccine (DTP + Hep-B + Hib) at 6, 10, and 14 weeks
- OPV at 6, 10, 14 weeks (in addition to birth OPV-0)
- Rotavirus vaccine at 6 and 10 weeks (in States where implemented)
- fIPV (fractional inactivated poliovirus) at 6 and 14 weeks
- PCV (pneumococcal conjugate vaccine) at 6 and 14 weeks (Universal Immunization Programme, UIP)
Newborn screening: Under the NHM, congenital hypothyroidism, congenital adrenal hyperplasia, and haemoglobinopathies are priority targets for newborn screening (a blood spot test ideally at 48–72 hours of life). Congenital hypothyroidism affects approximately 1:1,000 to 1:2,000 Indian neonates; untreated, it causes irreversible intellectual disability (cretinism). TSH screening at birth catches it before symptoms appear.
Red flags requiring urgent review (within 24 hours or emergency referral):
- Fever (axillary temperature >37.5°C) or hypothermia (<36.0°C)
- Jaundice within 24 hours of birth (always pathological — haemolytic disease until proven otherwise)
- Feeding difficulties — not sucking, refusing breast, <6 wet nappies after day 4
- Lethargy or poor tone — floppy baby
- Respiratory distress — grunting, nasal flaring, subcostal/intercostal retractions, RR >60/min
- Seizures or abnormal movements
- Umbilical redness, swelling, pus, or foul odour (omphalitis)
- Persistent vomiting or abdominal distension (possible intestinal obstruction or sepsis)
- Pallor, cyanosis, or mottled skin
- Excessive weight loss (>10% of birth weight) or failure to regain birth weight by day 14
Counselling parents on these red flags at the time of hospital discharge is a mandatory part of essential newborn care. Simple, illustrated take-home materials in the regional language significantly improve early recognition and care-seeking in community settings.
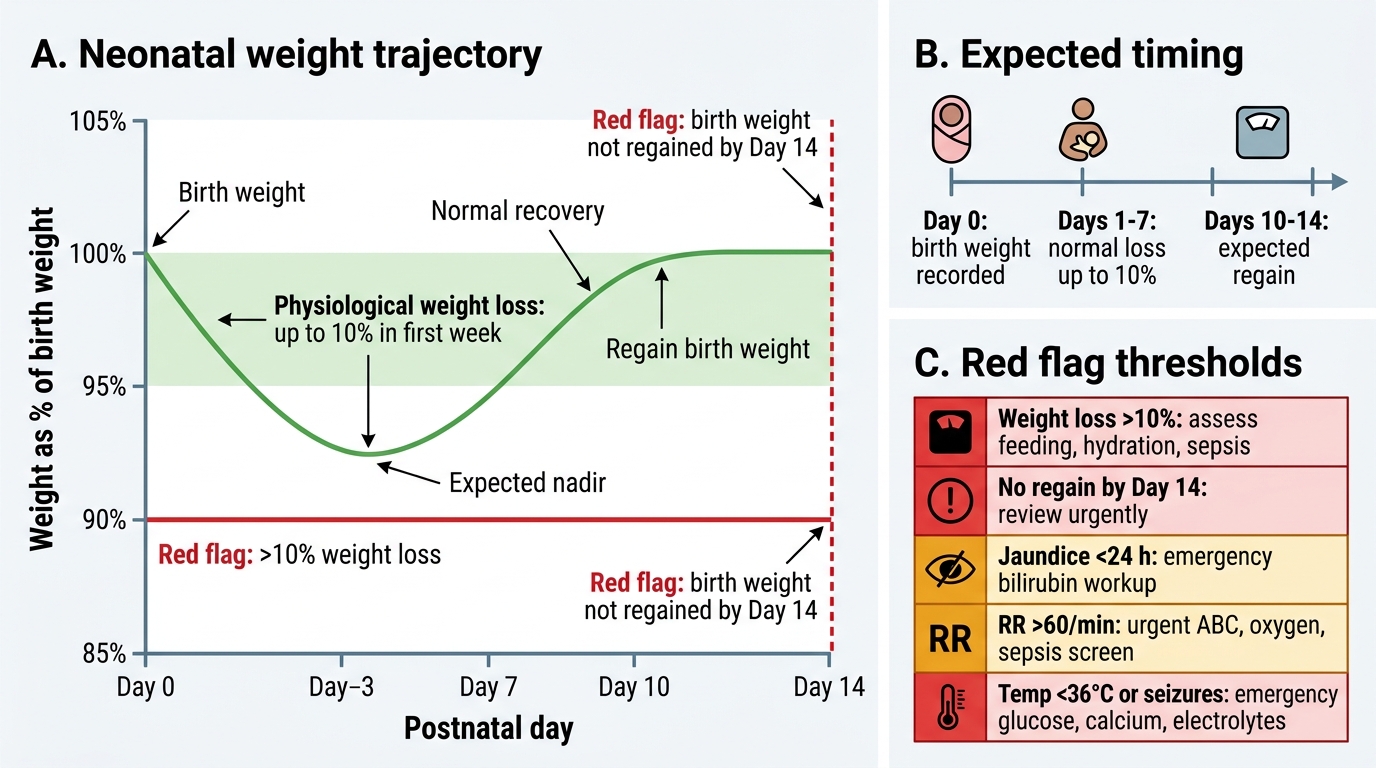
Neonatal Weight Loss and Red Flag Thresholds
| Red flag | Likely significance | Action |
|---|---|---|
| Jaundice < 24 h | Haemolytic (Rh/ABO/G6PD) | Emergency: serum bilirubin, blood group, Coombs |
| Jaundice after 2 weeks | Prolonged jaundice — rule out hypothyroidism, biliary atresia | Review: split bilirubin, TFT |
| RR >60 /min | Respiratory distress | Urgent: ABC assessment, O₂, sepsis screen |
| Axillary temp <36°C | Hypothermia | Warm immediately, KMC, feed, monitor glucose |
| Seizures | Hypoglycaemia, HIE, sepsis, metabolic | Emergency: glucose, Ca²⁺, electrolytes, LP |
Self-Assessment: Applying Newborn Care Knowledge
This section consolidates the module through integrative clinical reasoning. Review the key discriminating questions that examiners and clinical supervisors frequently test in neonatal settings.
Discriminating question 1 — APGAR vs Ballard vs Silverman-Anderson: You are in the labour room. The obstetrician asks you to 'score the baby'. Which score do you apply at 1 minute and 5 minutes after birth? (Answer: APGAR — evaluating HR, respiration, tone, reflex, colour.) A neonatologist later asks about the gestational maturity of a preterm baby brought from another facility with uncertain dates. Which scoring system is now appropriate? (Answer: Ballard/New Ballard — assessing neuromuscular and physical maturity criteria.) The NICU nurse asks you to monitor the respiratory distress in a preterm neonate on CPAP. Which score tracks this? (Answer: Silverman-Anderson Retraction Score.)
Discriminating question 2 — NIS at birth: From memory, list the three vaccines given at birth per the Indian NIS, their routes, and sites. (Answer: BCG 0.1 mL intradermal left deltoid; OPV-0 2 drops oral; Hep-B₀ 0.5 mL IM right anterolateral thigh.) Which of these specifically interrupts mother-to-child transmission? (Hep-B₀.)
Discriminating question 3 — normal vs pathological weight loss: A breastfed neonate weighing 3,200 g at birth is 2,960 g on day 4. Should you intervene? (Answer: weight loss = (3200-2960)/3200 × 100 = 7.5%, within the 10% normal physiological limit; reassure, reinforce breastfeeding.) If the same neonate is 2,780 g on day 4, what is the weight loss percentage and what should you do? (Answer: (3200-2780)/3200 × 100 = 13.1%; this exceeds 10% — formal breastfeeding assessment, lactation support, supplement if needed.)
Discriminating question 4 — red flag integration: A mother brings her 3-day-old home baby with 'yellowish eyes since yesterday'. The baby was born at term by normal delivery, birth weight 3.0 kg, and BCG/OPV/Hep-B were given. What is the key question to ask first? (Answer: when exactly did the jaundice appear? Jaundice within the first 24 hours = pathological, requires serum bilirubin, blood group and Coombs test urgently. Jaundice appearing after 24 hours in a term, well baby peaking day 3–5 = likely physiological, but monitor.)
| Scoring system | Timing | Parameters | Purpose |
|---|---|---|---|
| APGAR | 1 min & 5 min | HR, resp, tone, reflex, colour (5 items) | Immediate post-birth condition |
| New Ballard | Postnatal (first 12–96 h) | Neuromuscular + physical maturity (12 items) | Gestational age estimation |
| Silverman-Anderson | Serial, in NICU | Chest retraction, grunting, flaring (5 items) | Respiratory distress severity |
SELF-CHECK
A 5-day-old term neonate is noted to have jaundice by the mother. The baby is feeding well, active, and afebrile. Bilirubin is 14 mg/dL. This is most consistent with:
A. Pathological jaundice — Rh incompatibility
B. Physiological jaundice of the newborn
C. Neonatal hepatitis
D. Biliary atresia
Reveal Answer
Answer: B. Physiological jaundice of the newborn
Physiological jaundice appears after 24 hours of life, peaks around day 3–5, is predominantly unconjugated, and occurs in a well, active, feeding baby. The bilirubin of 14 mg/dL in a term neonate on day 5 fits within expected physiological range. Rh incompatibility presents within the first 24 hours with rapidly rising bilirubin and positive Coombs test. Neonatal hepatitis and biliary atresia typically present with conjugated (direct) hyperbilirubinaemia, pale stools, and dark urine — and usually not before 2 weeks. Biliary atresia jaundice persists beyond 2 weeks.