Page 5 of 16
PE15.2 | Sodium Potassium Imbalance — SDL Guide (Part 2)
Interpreting the Electrolyte Report
A systematic approach to interpreting a serum electrolyte report prevents errors from fixation on a single value. The report must always be interpreted in clinical context — the patient's history, volume status, medications, and urine findings. Four steps guide interpretation:
Step 1 — Identify the abnormality: Compare each value against the age-appropriate reference range. Normal ranges in children (serum): Na 135-145 mmol/L; K 3.5-5.5 mmol/L; Cl 98-107 mmol/L; bicarbonate (venous) 22-29 mmol/L. Note: the upper limit for K in neonates is slightly higher (~5.7-6.0) due to lower aldosterone responsiveness.
Step 2 — Assess volume status clinically: Is the child hypovolaemic (dehydrated, sunken eyes, tachycardia), euvolaemic (normal), or hypervolaemic (oedematous)? This categorises sodium disorders and identifies whether renin-aldosterone is activated (causing low urine Na).
Step 3 — Check urine sodium and osmolality (if available): Urine Na < 10 mmol/L → kidney is avid for sodium (extra-renal loss, low cardiac output/nephrotic state); Urine Na > 20 mmol/L → kidney is wasting sodium (renal loss, SIADH, adrenal insufficiency, diuretics). Urine osmolality > plasma osmolality in a hyponatraemic patient = SIADH until proven otherwise.
Step 4 — Assess associated electrolyte changes: Hypokalaemia with metabolic alkalosis → suspect diuretics, vomiting (HCl loss), or hyperaldosteronism. Hyperkalaemia with metabolic acidosis → suspect renal failure, adrenal insufficiency, or acidosis-driven transcellular shift. Co-existing hyponatraemia and hypokalaemia in a child on furosemide is a classic diuretic effect.
Common co-existent patterns in children:
| Condition | Na | K | Key clue |
|---|---|---|---|
| Diarrhoea | Low or normal | Low | Stool rich in both Na and K |
| Diuretic (furosemide) | Low | Low | Metabolic alkalosis; on loop diuretic |
| Renal failure | Low or normal | High | Oliguria, raised creatinine |
| SIADH | Low | Normal | Euvolaemic; urine Na > 20 |
| Addison's disease | Low | High | Hyperpigmentation, hypotension |
Always integrate electrolyte values with the clinical picture — isolated numbers without context lead to dangerous overcorrection or under-treatment.
Management of Sodium Imbalance
The fundamental principle governing sodium correction in children is that the speed of correction must not exceed the speed at which the disorder developed. Chronic sodium disorders have been compensated at the cellular level; rapid reversal disrupts these adaptations and causes iatrogenic injury.
Provided image
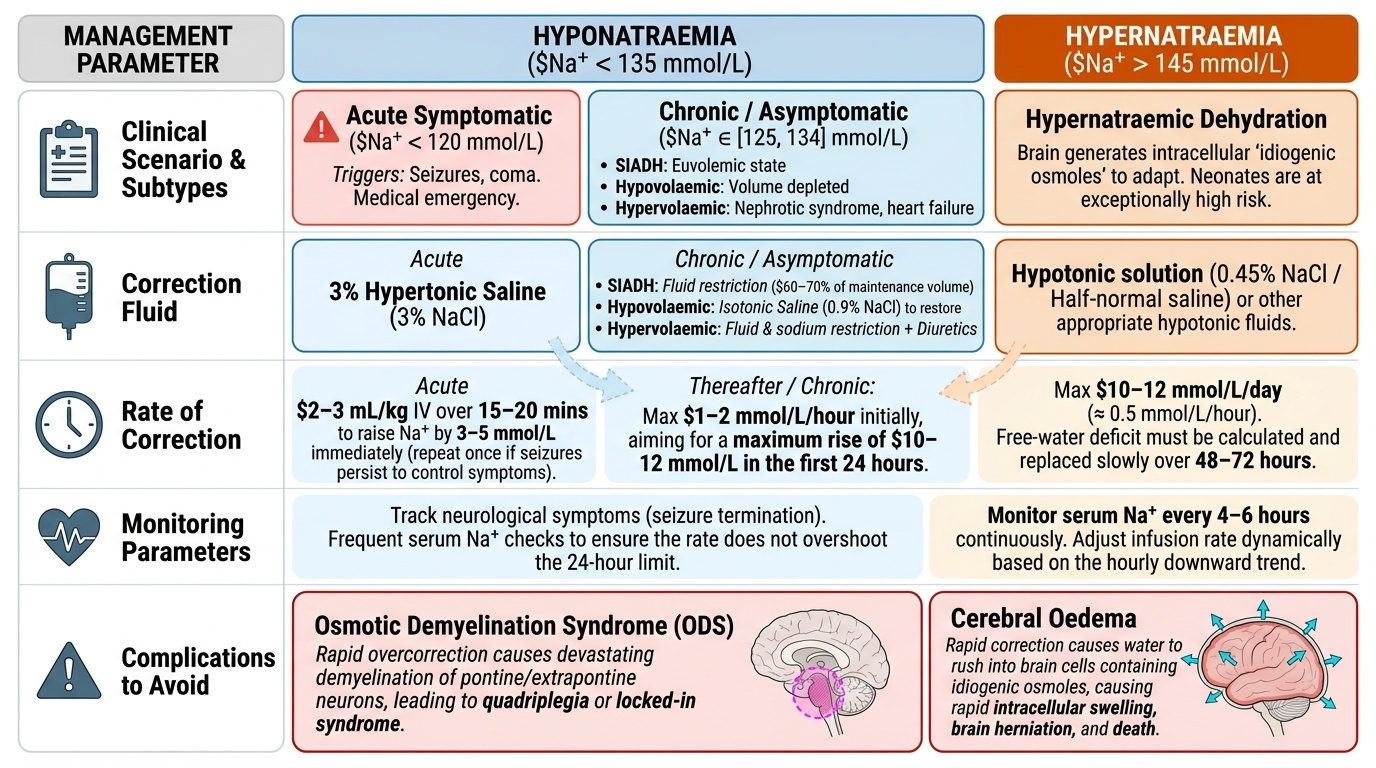
Hyponatraemia management is guided by severity and acuity:
Acute symptomatic hyponatraemia (seizures, coma — typically acute-onset, Na < 120): This is a medical emergency requiring immediate treatment regardless of volume status. Give hypertonic saline (3% NaCl) 2-3 mL/kg IV over 15-20 minutes to raise Na by 3-5 mmol/L and terminate seizures. Repeat once if seizures persist. The goal here is symptom control, NOT full correction. Thereafter correct at no more than 1-2 mmol/L/hour initially, aiming to raise Na by no more than 10-12 mmol/L in the first 24 hours. Overshoot beyond this risks osmotic demyelination syndrome (ODS) — a devastating demyelination of pontine and extrapontine neurons causing locked-in syndrome or quadriplegia.
Chronic or asymptomatic hyponatraemia (Na 125-134, no symptoms): Identify and treat the underlying cause. For SIADH: fluid restriction (usually 60-70% of maintenance) is the cornerstone; no sodium replacement unless severely symptomatic. For hypovolaemic hyponatraemia: restore volume with isotonic saline (0.9% NaCl) — correcting the volume deficit reduces ADH stimulus, and Na will rise spontaneously. For hypervolaemic hyponatraemia (nephrotic, cardiac failure): treat the underlying cause, fluid and sodium restriction, diuretics as appropriate.
Hypernatraemia management: The brain adapts to hypernatraemia by generating intracellular osmoles (idiogenic osmoles) to maintain cell volume. Rapid correction reverses this and causes cerebral oedema. The maximum safe correction rate is no more than 10-12 mmol/L/day (approximately 0.5 mmol/L/hour). Use 0.45% NaCl (half-normal saline) or an appropriate hypotonic solution; calculate the free-water deficit and replace it over 48-72 hours. Monitor serum Na every 4-6 hours and adjust the rate accordingly. In hypernatraemic dehydration in neonates, be especially cautious — never rehydrate faster than this rate.
SELF-CHECK
A 4-year-old child with meningitis has serum Na 118 mmol/L and is having repeated seizures. What is the most appropriate immediate management?
A. Fluid restrict to 60% maintenance and monitor hourly
B. Normal saline (0.9% NaCl) bolus 20 mL/kg
C. Hypertonic saline (3% NaCl) 2-3 mL/kg IV over 15-20 minutes
D. Correct fully to 135 mmol/L over the next 6 hours
Reveal Answer
Answer: C. Hypertonic saline (3% NaCl) 2-3 mL/kg IV over 15-20 minutes
Acute symptomatic hyponatraemia with seizures (Na 118 mmol/L, likely from SIADH in meningitis) is an emergency requiring hypertonic saline (3% NaCl) 2-3 mL/kg IV over 15-20 minutes to raise Na by 3-5 mmol/L and abort the seizures. Full correction over 6 hours would exceed the safe limit of 10-12 mmol/L/24h and risk osmotic demyelination syndrome. Fluid restriction alone is too slow for an actively seizing child.
Management of Potassium Imbalance
Potassium disorders require management calibrated to severity and to the presence or absence of ECG changes, which are the strongest indicators of imminent arrhythmia risk.
Provided image
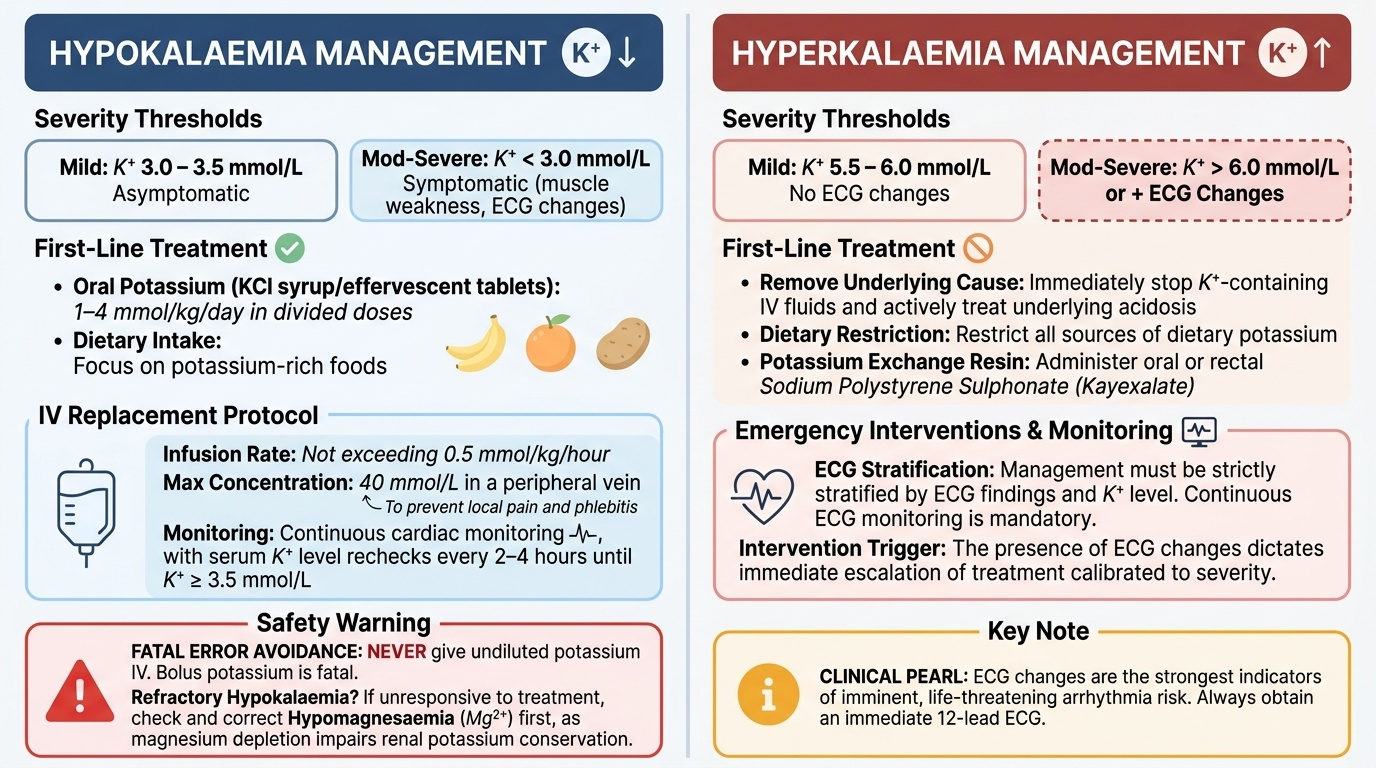
Hypokalaemia management: The underlying cause must be corrected in parallel.
Mild hypokalaemia (K 3.0-3.5 mmol/L, no symptoms): Oral potassium supplementation (KCl syrup or effervescent tablets, 1-4 mmol/kg/day in divided doses) combined with dietary potassium-rich foods (banana, orange, potato). Preferred whenever the child can take oral fluids.
Moderate-severe hypokalaemia (K < 3.0 mmol/L or symptomatic with weakness/ECG changes): IV potassium chloride in saline or glucose, at a rate not exceeding 0.5 mmol/kg/hour with continuous cardiac monitoring. Concentration should not exceed 40 mmol/L in a peripheral vein (risk of pain and phlebitis). Never give undiluted potassium IV — bolus potassium is fatal. Recheck K every 2-4 hours and continue replacement until K > 3.5 mmol/L.
If hypokalaemia is refractory, look for concurrent hypomagnesaemia — magnesium depletion impairs renal potassium conservation and causes aldosterone activation; correct Mg first.
Hyperkalaemia management is stratified by ECG findings and K level:
Mild hyperkalaemia (K 5.5-6.0 mmol/L, no ECG changes): Remove the cause (stop K-containing IV fluids, treat acidosis), dietary K restriction, exchange resin (sodium polystyrene sulphonate, Kayexalate) orally or rectally to enhance faecal K excretion.
Moderate hyperkalaemia (K 6.0-6.5 mmol/L) or any ECG changes: Cardiac membrane stabilisation is the immediate priority — calcium gluconate 10% solution, 0.5-1 mL/kg IV over 5-10 minutes (up to 10 mL), with cardiac monitoring. Calcium does NOT lower K; it raises the threshold potential of the myocardium, protecting it from arrhythmia while other measures reduce K.
Definitive K reduction: (a) Insulin (0.1 units/kg short-acting) + dextrose (0.5 g/kg, i.e., 5 mL/kg of 10% dextrose) IV — shifts K into cells within 15-30 minutes; (b) Nebulised salbutamol (beta-2 agonist) — also shifts K into cells via Na-K ATPase; (c) Sodium bicarbonate (if metabolic acidosis present) — correcting acidosis shifts K into cells; (d) Furosemide (if urine output adequate) — increases renal K excretion; (e) Dialysis — for renal failure or refractory life-threatening hyperkalaemia.
SELF-CHECK
A 6-year-old boy with acute kidney injury has serum K 6.8 mmol/L. His ECG shows peaked T waves and a widened QRS complex. What is the FIRST step in management?
A. Sodium polystyrene sulphonate (Kayexalate) enema
B. Calcium gluconate 10% 0.5-1 mL/kg IV over 5-10 minutes
C. Insulin + dextrose infusion
D. Dietary potassium restriction and recheck in 4 hours
Reveal Answer
Answer: B. Calcium gluconate 10% 0.5-1 mL/kg IV over 5-10 minutes
In hyperkalaemia with ECG changes (peaked T waves, widened QRS), the immediate priority is cardiac membrane stabilisation — NOT K removal. Calcium gluconate 10% 0.5-1 mL/kg IV over 5-10 minutes antagonises the myocardial membrane effects of hyperkalaemia and protects against arrhythmia. It takes effect within 1-3 minutes. Insulin + dextrose and Kayexalate are definitive K-lowering measures that follow; dietary restriction alone is inadequate for an emergency.