Page 6 of 16
PE15.2 | Sodium Potassium Imbalance — SDL Guide (Part 3)
Self-Assessment: Electrolyte Interpretation and Management
Having studied the clinical presentations, pathophysiology, interpretation framework, and management of sodium and potassium disorders, you are now ready to apply this knowledge to an integrated scenario. The ability to move from a reported electrolyte value to a safe, mechanistically justified management plan is the core clinical skill this module is designed to build. In real clinical practice these disorders rarely present in isolation — they co-exist, as in the case below, because the same underlying cause or medication drives multiple abnormalities simultaneously. Work through the following questions independently before checking the answers — each question tests a different domain of the competency.
Scenario: A 5-year-old boy with nephrotic syndrome on furosemide presents with general weakness, poor appetite, and leg cramps for 3 days. Electrolytes: Na 131 mmol/L, K 2.6 mmol/L, Cl 88 mmol/L, bicarbonate 28 mmol/L. ECG shows flattened T waves.
Questions:
1. Classify the sodium and potassium abnormalities.
2. What is the likely mechanism for both abnormalities in this child?
3. What is the appropriate immediate management for the hypokalaemia?
4. Is immediate correction of the hyponatraemia warranted? Why or why not?
Worked answers:
1. Hyponatraemia (Na 131 — mild) + Hypokalaemia (K 2.6 — moderate) + metabolic alkalosis (bicarbonate 28, Cl low).
2. Furosemide causes both — it inhibits the Na-K-2Cl co-transporter in the loop of Henle, causing urinary loss of Na, K, and Cl, with compensatory bicarbonate retention (metabolic alkalosis). In nephrotic syndrome, the primary disorder also promotes Na retention and oedema.
3. IV KCl in saline at ≤ 0.5 mmol/kg/hour with continuous cardiac monitoring; switch to oral KCl supplementation when K > 3.0 and the child can tolerate oral intake. Ensure potassium-rich diet (banana, orange juice).
4. No — Na 131 is asymptomatic mild hyponatraemia; do NOT give hypertonic saline. Furosemide-induced hyponatraemia responds to dose reduction and addressing the underlying cause; correction will occur spontaneously as the potassium and volume status are restored.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
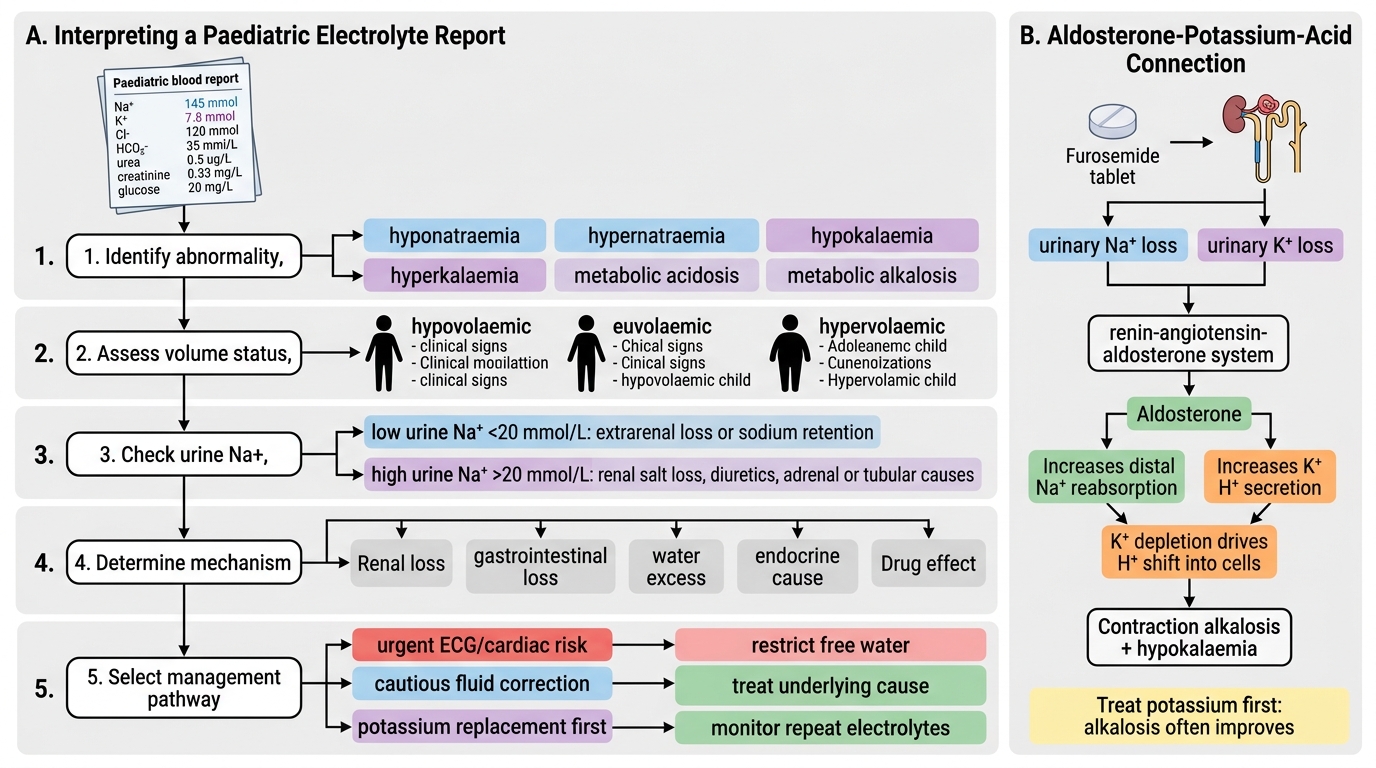
Paediatric Electrolyte Report Interpretation Algorithm
CLINICAL PEARL
The aldosterone-potassium-acid connection: Many electrolyte disorders co-exist because of shared regulatory pathways. Furosemide causes both hypokalaemia AND hyponatraemia by promoting urinary Na and K loss. Metabolic alkalosis then develops because K depletion causes H⁺ to shift intracellularly to maintain electroneutrality, and aldosterone activation from volume depletion causes further H⁺ excretion. This 'contraction alkalosis with hypokalaemia' is one of the most common electrolyte patterns you will encounter in a paediatric ward. Treat the potassium first — it will often correct the alkalosis too.