Page 10 of 30
PE20.4 | Hematuria — SDL Guide
Learning Objectives
- Distinguish macroscopic from microscopic haematuria and identify false-positive causes on urine dipstick
- Classify haematuria as glomerular or non-glomerular based on urine microscopy findings
- Enumerate the common causes of glomerular and non-glomerular haematuria in Indian children
- Outline a systematic diagnostic approach including history, urine microscopy, UPCR, complement, serology, imaging, and family history
- Identify the referral criteria for haematuria in a child and outline initial management for common non-glomerular causes
INSTRUCTIONS
Haematuria — blood in the urine — is a common and often alarming finding that brings children and their families to medical attention. The challenge lies in determining whether the blood is originating from the glomerulus (where it points to potentially progressive glomerular disease) or from the urological tract (where it points to infection, stones, hypercalciuria, or — rarely — tumour). A structured approach to this distinction, built on urine microscopy rather than urine colour alone, is the essential skill this module develops.
References
- Ghai Essential Pediatrics, 9th edition, Ch 18 — Nephrology (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 536 — Haematuria (textbook)
- IAP Standard Treatment Guidelines — Haematuria in Children (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-year-old girl is brought urgently because her mother noticed that her urine turned red-pink two hours ago. She has no fever, no dysuria, no abdominal pain, and no recent trauma. She had beetroot in her meal last night. Her urine dipstick is positive for blood (3+). You send a midstream urine for microscopy. While waiting, the mother says she recalls her brother 'had kidney trouble' in childhood. How do you approach this child? What does the dipstick result tell you, and what does it NOT tell you? What single microscopic finding will most decisively direct your next steps?
WHY THIS MATTERS
Haematuria is the second most common urinary abnormality after proteinuria referred to a paediatric nephrologist, and it is also a source of considerable parental anxiety. Its clinical significance ranges from entirely benign isolated microscopic haematuria (which affects up to 1–2% of school-age children and most commonly reflects hypercalciuria or thin glomerular basement membrane disease) to the visible sign of serious glomerulonephritis, urological pathology, or — rarely — a renal tumour. The skill this module develops — the ability to systematically distinguish glomerular from non-glomerular haematuria, to apply appropriate investigations, and to identify the red flags that demand nephrology referral — will prevent both the over-referral of children with benign haematuria and the under-referral of those with progressive glomerular disease that, if missed, could result in chronic kidney disease.
RECALL
Before proceeding, recall:
- Glomerular filtration (from AN/PY): red blood cells (diameter ~7 µm) do not normally pass through the glomerular filtration barrier. When they do — due to glomerular inflammation or basement membrane defects — they are deformed by the mechanical shear and osmotic stress of transit through the tubule, producing dysmorphic RBCs.
- APSGN (from PE20.2): the prototype post-infectious nephritic syndrome, where haematuria is the cardinal presenting sign, arising from immune-complex-mediated glomerular inflammation. Recall the latent period (1–2 weeks after pharyngitis; 3–6 weeks after pyoderma) and the C3-low/C4-normal complement pattern.
- UTI (from PE20.1): the commonest non-glomerular cause of haematuria in young children; always exclude infection as the first step by urine culture.
- Urine dipstick for haematuria: reagent strips detect haemoglobin (and myoglobin) by their peroxidase activity; a positive dipstick therefore indicates the presence of haem, not necessarily intact red blood cells — haemoglobinuria and myoglobinuria give positive dipsticks with few or no RBCs on microscopy.
Clinical Presentation and Recognition of Haematuria
Haematuria in children presents either symptomatically — with red, pink, brown, or cola-coloured urine that alarms the family — or incidentally on routine dipstick testing. The first clinical task is to confirm that the dipstick positivity represents genuine haematuria (intact red blood cells), not a dipstick false-positive or red discolouration from a non-haematological cause. This distinction is made by urine microscopy, not by dipstick alone, and its importance cannot be overstated: a confident erroneous diagnosis of haematuria from a beetroot-pigment positive dipstick leads to unnecessary investigation, anxiety, and cost.
Macroscopic (gross) haematuria: visibly discoloured urine, ranging from pink to bright red to dark brown or cola-coloured. Dark brown (cola-coloured) urine suggests that RBCs have been in the urine long enough to degrade — a feature more common with glomerular bleeding (where blood has been in the tubular fluid for longer) than with fresh urological bleeding (which tends to produce bright red urine). The volume of blood required to colour urine is surprisingly small — as little as 1 mL of blood per litre of urine produces visible discolouration.
Dipstick haematuria: dipstick sensitivity for detecting ≥5 RBC/hpf exceeds 95%, making it a reliable screening tool. However, false-positives occur with haemoglobinuria (intravascular haemolysis), myoglobinuria (rhabdomyolysis), and certain foods and pigments (beetroot/betacyanin, rifampicin, some dyes). The key differentiator is urine microscopy: a positive dipstick with fewer than 5 RBC/hpf on microscopy = haemoglobin or myoglobin in the urine, not intact RBCs = not haematuria.
Microscopic haematuria: ≥5 RBC/hpf on centrifuged urine sediment, or ≥5 RBC/mm³ on unspun urine. Asymptomatic microscopic haematuria is defined as this finding confirmed on ≥2 of ≥3 occasions over ≥3 months in the absence of infection.
The initial clinical assessment of haematuria should document:
• Associated urinary symptoms: dysuria, frequency, urgency → UTI; flank pain (colicky, radiating) → calculus; painless macroscopic → glomerular or tumour.
• Systemic features: periorbital oedema, hypertension → glomerulonephritis; rash, joint pains → HSP (Henoch-Schönlein purpura) or lupus; fever, weight loss → systemic disease or tumour.
• Family history: haematuria or early CKD in first-degree relatives → Alport syndrome or thin GBM disease; nephrolithiasis → familial hypercalciuria.
• Recent history: streptococcal throat or skin infection (APSGN), vigorous exercise (exercise-induced haematuria), trauma.
Pathophysiology and Aetiology
The single most clinically important classification in the approach to haematuria is the distinction between glomerular and non-glomerular (urological) origin. This distinction determines the entire investigation pathway, referral decision, and prognosis.
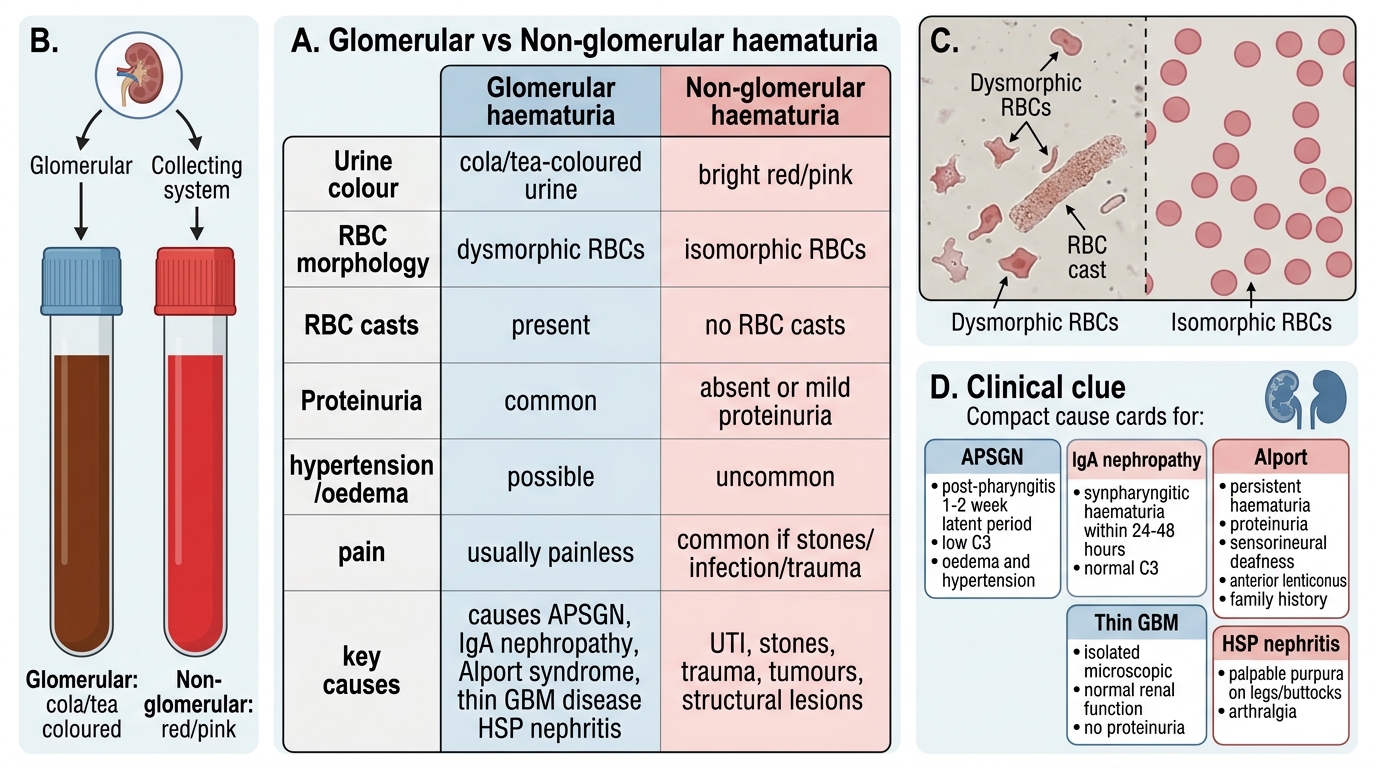
Glomerular haematuria arises when red blood cells pass through defects in the glomerular filtration barrier (inflamed endothelium, damaged GBM, or disrupted podocytes). The mechanical and osmotic stress of traversing the tubule distorts these RBCs into acanthocytes (spiculated, irregular), ghost cells, and other dysmorphic forms. When they aggregate in the tubular lumen with Tamm-Horsfall protein, they form RBC casts — the pathognomonic marker of glomerular haematuria. The urine in glomerular haematuria is typically brown, cola-coloured, or smoky (haemoglobin degraded to methaemoglobin), rarely bright red.
Non-glomerular haematuria arises from anywhere in the urological tract below the glomerulus — the renal tubules, renal pelvis, ureter, bladder, or urethra. RBCs enter the urine without deformation and appear isomorphic (eumorphic, uniform) on microscopy. The urine is typically bright red or pink, particularly with bladder or lower tract bleeding. Pain (colicky flank pain with calculi, suprapubic pain with cystitis) is more characteristic of non-glomerular causes.
Glomerular vs Non-glomerular Haematuria
Key glomerular causes of haematuria in children:
• APSGN: post-infectious, nephritic, C3 low — the prototype covered in PE20.2. Cola-coloured urine, hypertension, oedema, 1–2 week post-pharyngitis latent period.
• IgA nephropathy: synpharyngitic haematuria (within 24–48 hours of pharyngitis, NO latent period) — the most important distinguishing feature from APSGN. C3 is NORMAL. Mesangial IgA deposition on biopsy. Episodic macroscopic haematuria with persistent microscopic haematuria between episodes.
• Alport syndrome: X-linked hereditary nephritis caused by mutations in the COL4A5 gene (X-linked, ~85%) or COL4A3/COL4A4 (autosomal recessive, ~15%). Clinical triad: persistent haematuria + progressive proteinuria + sensorineural deafness + anterior lenticonus (ocular sign). Males with X-linked Alport progress to ESRD by age 20–30 years. Positive family history of haematuria and CKD is the critical clue.
• Thin glomerular basement membrane (thin GBM) disease / benign familial haematuria: isolated persistent microscopic haematuria with normal renal function, no proteinuria, and family history of microscopic haematuria; due to heterozygous COL4A3/A4 mutations; usually benign and does not progress.
• HSP (Henoch-Schönlein purpura / IgA vasculitis) nephritis: palpable purpuric rash on buttocks/legs + arthralgia + abdominal pain + haematuria ± proteinuria; IgA-mediated small-vessel vasculitis.
• Lupus nephritis: girls >10 years with systemic features (butterfly rash, arthritis, serositis); ANA positive; haematuria + proteinuria + low C3+C4.
Key non-glomerular causes:
• Urinary tract infection (UTI): commonest non-glomerular cause in young children; always exclude first. Dipstick positive for leucocyte esterase + nitrites; treat with antibiotics.
• Hypercalciuria: commonest cause of isolated microscopic haematuria with isomorphic RBCs in school-age children; diagnosed by spot urine calcium-to-creatinine ratio >0.2 (in children >2 years). May also cause nephrolithiasis.
• Nephrolithiasis: colicky flank pain, haematuria, USG shows calculus; associated with hypercalciuria, hyperoxaluria, or hypocitraturia.
• Trauma: blunt abdominal/renal trauma; haematuria + flank tenderness + history of injury.
• Wilms tumour (nephroblastoma): commonest renal malignancy in children <5 years; presents with painless abdominal mass ± haematuria ± hypertension — ALWAYS palpate the abdomen in a child with haematuria.
• Sickle-cell trait/disease: painless haematuria from renal papillary ischaemia; important in children of African/Indian descent.
SELF-CHECK
A 10-year-old boy has an episode of red-coloured urine that began within 24 hours of a sore throat. His urine microscopy shows 30–40 RBC/hpf, dysmorphic with acanthocytes, but NO casts. Serum C3 is normal. Which diagnosis is MOST consistent with this presentation?
A. Acute post-streptococcal glomerulonephritis (APSGN)
B. IgA nephropathy
C. Nephrolithiasis
D. UTI
Reveal Answer
Answer: B. IgA nephropathy
The key is the timing: haematuria within 24 hours of pharyngitis = SYNPHARYNGITIC haematuria = IgA nephropathy (not APSGN, which has a 1–2 week latent period). The normal C3 further supports IgA nephropathy (C3 is LOW in APSGN). Dysmorphic RBCs confirm glomerular origin. Nephrolithiasis would present with colicky pain and isomorphic RBCs. UTI would show leucocyturia and bacteriuria.
Diagnostic Approach and Investigation
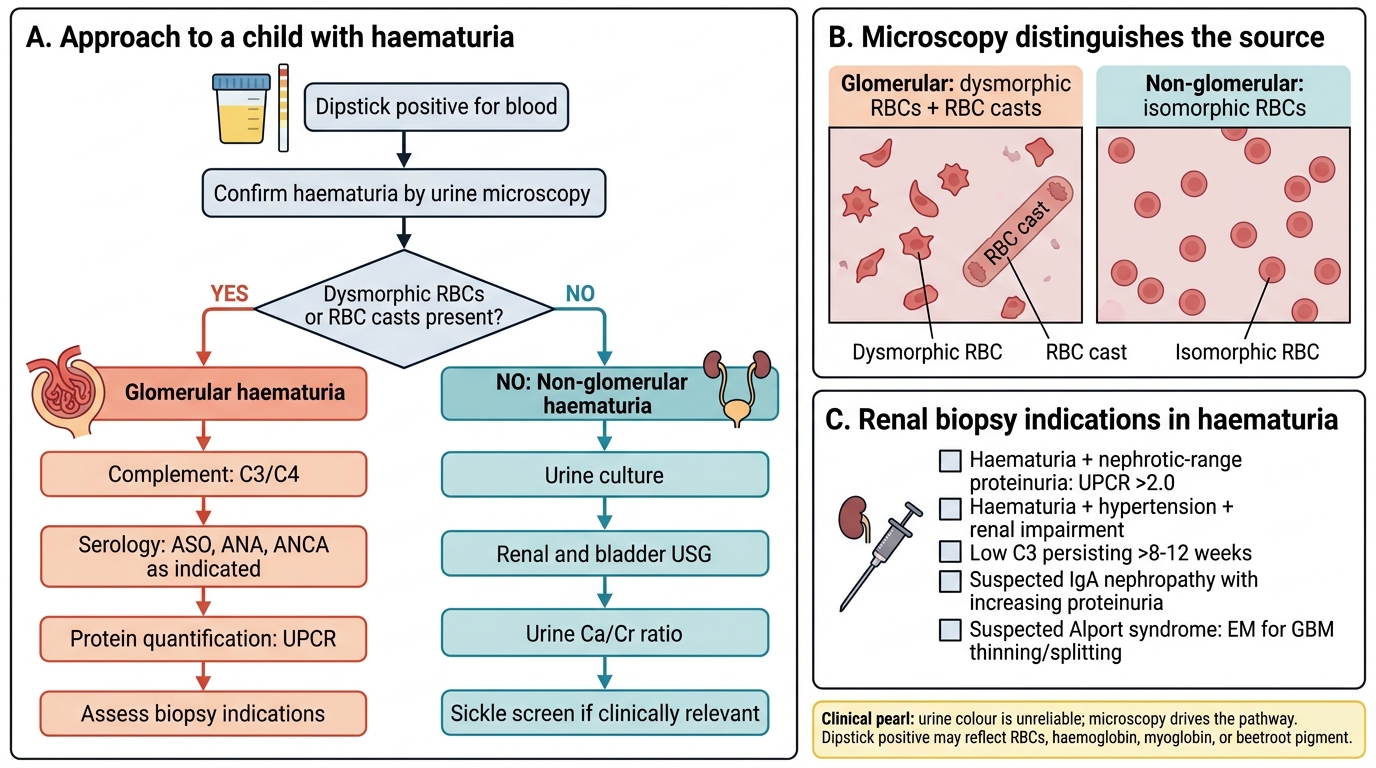
The diagnostic approach to haematuria follows a logical, stepwise sequence that begins with urine microscopy to confirm genuine haematuria and determine its anatomical origin, then proceeds to targeted investigations based on whether the origin is glomerular or non-glomerular. This ordering is not arbitrary: no child with a positive dipstick should undergo imaging or renal biopsy before microscopy has first confirmed the presence of intact red blood cells and assessed their morphology. Skipping this gatekeeper step leads either to unnecessary invasive investigation when the dipstick was a false-positive, or to misdirected investigation when the morphology clearly points to a non-glomerular cause. The clinical history, examination findings, and family history inform the investigation choice at each step but do not replace the morphological classification.
Step 1 — Confirm haematuria by microscopy: centrifuged midstream urine; ≥5 RBC/hpf confirms haematuria. Assess morphology: dysmorphic RBCs (acanthocytes, ghost cells, crenated cells) and/or RBC casts = glomerular. Isomorphic (eumorphic) RBCs without casts = non-glomerular. Pyuria (>10 WBC/hpf) with bacteriuria → UTI; send culture.
Step 2 — Glomerular haematuria workup:
• UPCR on first morning urine: haematuria + UPCR >2.0 = nephrotic-range proteinuria + haematuria = urgent biopsy indication (never seen in benign causes).
• Serum complement C3 and C4: C3 low (C4 normal) = APSGN or MPGN; C3+C4 low = lupus nephritis; normal = IgA nephropathy, thin GBM, Alport.
• Streptococcal serology: ASO + anti-DNase B if latent period and nephritic features suggest APSGN.
• ANA, anti-dsDNA: if girl >10 years, systemic features, or mixed nephritic-nephrotic.
• Audiometry: in any child with persistent haematuria and family history of haematuria + CKD (Alport syndrome).
• Slit-lamp eye examination: anterior lenticonus in Alport syndrome.
• Family history: screen first-degree relatives with dipstick if Alport or thin GBM disease is suspected.
Step 3 — Non-glomerular haematuria workup:
• Urine culture: for all children with haematuria to exclude UTI.
• Urine calcium-to-creatinine ratio (spot urine, mg:mg): >0.2 in children >2 years = hypercalciuria. Confirm with 24-hour urine if elevated.
• USG KUB: identifies nephrolithiasis, hydronephrosis, renal/pelvic masses. MUST be performed in any child with macroscopic haematuria.
• Haemoglobin electrophoresis / sickle-cell screen: if descent is relevant.
• Urine for haemoglobin and myoglobin: if dipstick positive with few RBCs on microscopy.
Approach to Haematuria in a Child
Renal biopsy indications in haematuria:
• Haematuria + nephrotic-range proteinuria (UPCR >2.0)
• Haematuria + hypertension + renal impairment
• Haematuria + low complement (C3 persisting >8–12 weeks)
• Suspected IgA nephropathy with increasing proteinuria (to guide therapy)
• Suspected Alport syndrome (for electron microscopy — thinning and splitting of GBM)
CLINICAL PEARL
Urine colour does NOT reliably distinguish glomerular from non-glomerular haematuria — only microscopy does. Dark cola-coloured urine suggests glomerular bleeding (older blood, haemoglobin degraded), but bright red urine does not exclude glomerular disease, and dark urine does not exclude a urological cause. Furthermore, a positive dipstick is not the same as haematuria — betacyanin (beetroot), haemoglobin, and myoglobin all give positive dipstick reactions. Always look at the microscopy result: dysmorphic RBCs + RBC casts = glomerular; isomorphic RBCs = non-glomerular. This distinction drives the entire investigation pathway.