Page 7 of 30
PE20.3 | Proteinuria — SDL Guide
Learning Objectives
- Recognise the clinical and laboratory features that suggest proteinuria in a child
- Classify proteinuria by pattern (transient vs persistent) and severity (subnephrotic vs nephrotic-range) using UPCR and timed urine thresholds
- Describe the pathophysiology of glomerular, tubular, and overflow proteinuria and their common paediatric causes
- Outline the diagnostic approach to proteinuria including the orthostatic test, UPCR, blood investigations, and indications for renal biopsy
- Plan appropriate management for transient proteinuria and first-episode nephrotic syndrome (MCNS protocol), and identify referral criteria for persistent, heavy, or complex proteinuria
INSTRUCTIONS
Proteinuria detected on routine or opportunistic urine dipstick testing is one of the most common abnormal findings referred to a paediatrician. Its significance ranges from entirely benign (orthostatic proteinuria, post-febrile) to the sentinel of serious glomerular disease (nephrotic syndrome, lupus nephritis). The ability to rapidly classify proteinuria — transient versus persistent, subnephrotic versus nephrotic-range — and to apply the correct diagnostic algorithm determines whether a child receives reassurance, a monitored trial of steroids, or an urgent nephrology referral. This module builds that decision logic from first principles.
References
- Ghai Essential Pediatrics, 9th edition, Ch 18 — Nephrology (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 535 — Nephrotic Syndrome (textbook)
- IAP Standard Treatment Guidelines — Nephrotic Syndrome in Children, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-year-old boy is brought for a pre-school medical check-up. He is well, has no swelling or symptoms, but his routine urine dipstick shows 2+ protein. His mother is worried. You perform a repeat dipstick on a fresh urine sample the next morning: it shows trace protein. On examination the child is entirely normal — no oedema, normal blood pressure, normal growth parameters. How do you interpret this finding? What is the next single most important investigation, and when would you refer this child to a paediatric nephrologist?
WHY THIS MATTERS
Proteinuria is the single most important urinary abnormality linking a simple dipstick finding to a spectrum of conditions ranging from inconsequential orthostatic variation to progressive glomerular disease with the potential for long-term renal impairment. In clinical practice, it is the hallmark biochemical feature of nephrotic syndrome — the commonest chronic glomerular disease of childhood — and also appears as a secondary feature in almost every form of glomerulonephritis. The paediatrician who can confidently classify proteinuria, perform the orthostatic test, apply UPCR thresholds, and identify red-flag features requiring nephrology referral prevents both under-investigation (missing significant glomerular disease) and over-investigation (unnecessary renal biopsies for benign orthostatic proteinuria). This competency is tested in professional examinations and applied in every paediatric nephrology outpatient encounter.
RECALL
Before proceeding, recall:
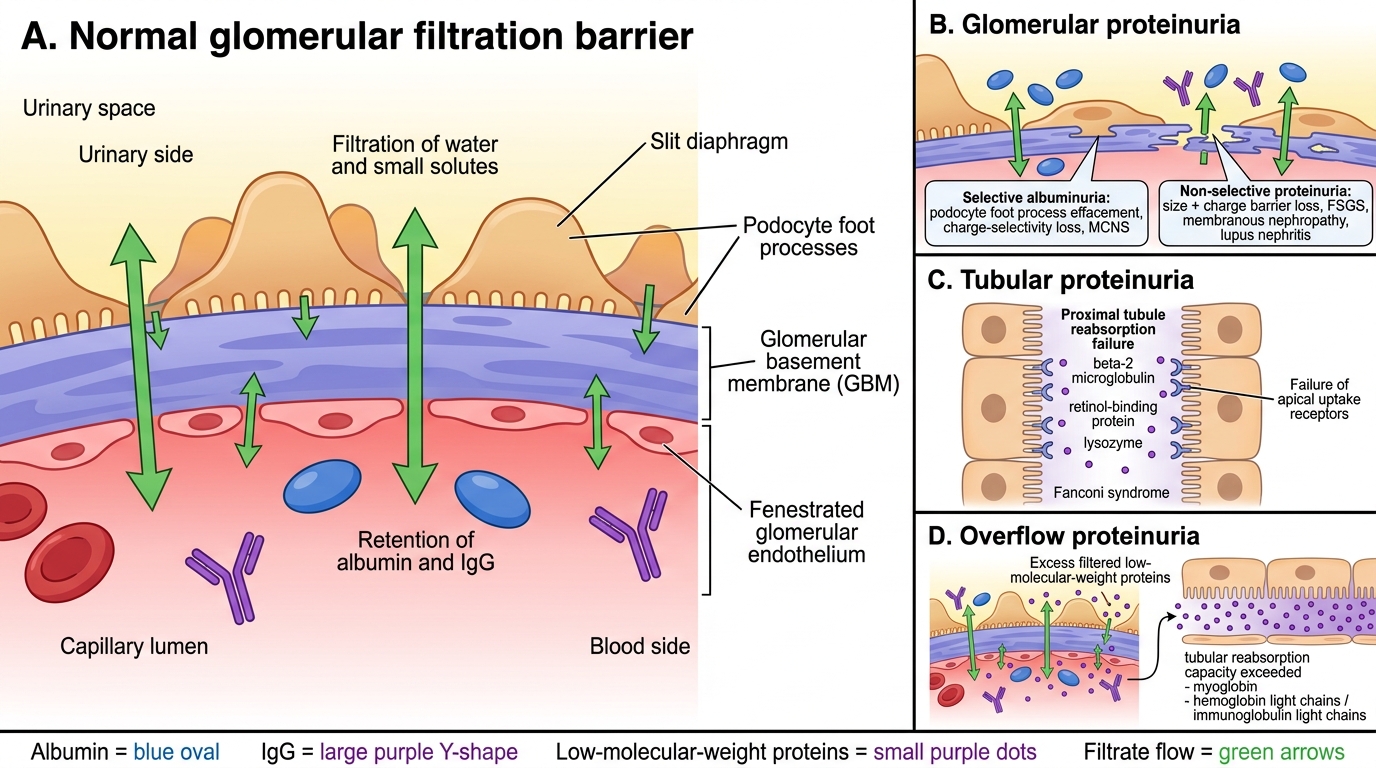
- Glomerular filtration barrier (from AN): consists of three layers — fenestrated capillary endothelium, glomerular basement membrane (GBM), and podocyte foot processes with slit diaphragms. Normally this barrier is size-selective (blocks proteins >70 kDa) and charge-selective (GBM is negatively charged, repelling anionic albumin).
- Albumin and oncotic pressure (from PY): albumin (MW ~69 kDa) is the principal plasma protein maintaining colloid osmotic pressure (~25 mmHg). Hypoalbuminaemia (serum albumin <2.5 g/dL in nephrotic syndrome) reduces oncotic pressure, favouring movement of fluid from the vascular to the interstitial compartment — causing oedema.
- Urine dipstick: reagent strips detect predominantly albumin via the protein-error-of-indicators method; they under-detect Bence-Jones proteins and tubular low-molecular-weight proteins. A positive dipstick should always be confirmed on a first morning midstream urine to avoid false-positives from concentrated upright urine.
Clinical Presentation and Recognition of Proteinuria
Proteinuria in children comes to clinical attention in one of two ways: either through symptomatic presentation, when significant protein loss leads to oedema and the family notices frothy urine or facial swelling, or through incidental detection on a dipstick performed during a well-child visit, fever assessment, or pre-operative work-up. The clinical presentation therefore spans a wide severity range, and the doctor's initial task is to determine whether the child is systemically well (pointing to benign or transient causes) or unwell (pointing to nephrotic syndrome, glomerulonephritis, or systemic disease).
Symptomatic proteinuria of clinical significance typically presents as the full nephrotic syndrome — characterised by massive urinary protein loss (>40 mg/m²/hr or UPCR >2.0), hypoalbuminaemia (serum albumin <2.5 g/dL), generalised oedema (periorbital first, then lower limbs, ascites, pleural effusion in severe cases), hyperlipidaemia, and lipiduria (oval fat bodies, fatty casts on microscopy). Parents describe the urine as frothy or bubbly — a practical sign worth asking about. The classic presentation is a 2–6-year-old boy with periorbital swelling worse in the morning (mistaken for allergy) and gradually increasing abdominal distension.
Asymptomatic proteinuria detected incidentally requires careful interpretation. Dipstick grading (trace ≈10–20 mg/dL; 1+ ≈30 mg/dL; 2+ ≈100 mg/dL; 3+ ≈300 mg/dL; 4+ >2000 mg/dL) gives only a rough concentration estimate. The first and most important step after a positive dipstick is to repeat the test on a first-void morning urine — this eliminates orthostatic proteinuria (which disappears in the supine position) and concentration artefacts from afternoon urine. If the first morning sample is negative, benign transient or orthostatic proteinuria is the likely explanation.
Glomerular Filtration Barrier and Mechanisms of Proteinuria
Pathophysiology and Classification
Proteinuria arises by three distinct mechanisms, each pointing to a different part of the nephron and a different set of underlying diseases. Understanding the mechanism determines the investigation pathway and the differential diagnosis.
Glomerular proteinuria results from loss of the size-selectivity and/or charge-selectivity of the glomerular filtration barrier. In minimal change nephrotic syndrome (MCNS) — the commonest cause of nephrotic syndrome in children aged 1–8 years — podocyte foot process effacement causes loss of the charge-selective barrier, resulting in selective albuminuria (albumin predominates; IgG not lost = 'highly selective proteinuria'). In focal segmental glomerulosclerosis (FSGS), membranous nephropathy, and lupus nephritis, both size and charge selectivity are disrupted, leading to non-selective proteinuria (albumin + IgG + other large proteins). APSGN produces subnephrotic glomerular proteinuria from transient glomerular inflammation.
Tubular proteinuria results from failure of the proximal tubule to reabsorb low-molecular-weight proteins (beta-2 microglobulin, retinol-binding protein, lysozyme) that normally pass the glomerular barrier and are reabsorbed proximally. Causes include Fanconi syndrome (proximal tubular dysfunction from cystinosis, Wilson's disease, galactosaemia, heavy metals, tenofovir), renal tubular acidosis, and pyelonephritis. Tubular proteinuria is characteristically low-grade (usually <1+ on dipstick) and accompanied by glucosuria (with normal blood glucose), aminoaciduria, and phosphaturia — the tubular transport failure is generalised.
Overflow proteinuria occurs when plasma levels of a freely-filtered low-molecular-weight protein overwhelm tubular reabsorption capacity. The prototype is Bence-Jones proteinuria in myeloma (not relevant to children) but the same mechanism operates in haemoglobinuria and myoglobinuria.
Transient vs persistent proteinuria:
• Febrile proteinuria: mild proteinuria during acute illness (fever, exercise, emotional stress) from transient glomerular haemodynamic changes; resolves as illness resolves.
• Orthostatic (postural) proteinuria: proteinuria in the upright posture only — the most common cause of asymptomatic proteinuria in older children (10–16 years). The mechanism involves increased renal venous pressure in the upright position. It is entirely benign, does not progress to renal disease, and requires only annual review.
• Persistent proteinuria (>3 months): requires full investigation — likely represents significant glomerular pathology.
Persistent causes in children by frequency: MCNS (steroid-sensitive; ~85% of nephrotic syndrome <8 yr), FSGS (steroid-resistant), lupus nephritis (females >10 yr with systemic features), IgA nephropathy (haematuria + subnephrotic proteinuria), APSGN (transient, post-infectious), Alport syndrome (haematuria + family history of renal disease), and Fanconi syndrome.
SELF-CHECK
A 5-year-old boy has a spot urine protein-to-creatinine ratio (UPCR) of 3.2 on a midstream urine sample. Which of the following is the most appropriate interpretation?
A. Normal finding; repeat in 6 months
B. Subnephrotic proteinuria; investigate for orthostatic cause
C. Nephrotic-range proteinuria; proceed to full nephrotic syndrome workup
D. Likely contamination; repeat dipstick only
Reveal Answer
Answer: C. Nephrotic-range proteinuria; proceed to full nephrotic syndrome workup
A UPCR of 3.2 exceeds the nephrotic-range threshold of >2.0 (equivalent to >40 mg/m²/hr on timed urine). This mandates a full workup for nephrotic syndrome including serum albumin, lipid profile, complement, renal function, and urine microscopy. UPCR <0.2 is normal in children >2 years; 0.2–2.0 is subnephrotic. UPCR >2.0 on a first morning specimen (to exclude orthostatic) is nephrotic-range and requires clinical evaluation.
Diagnostic Approach and Investigation
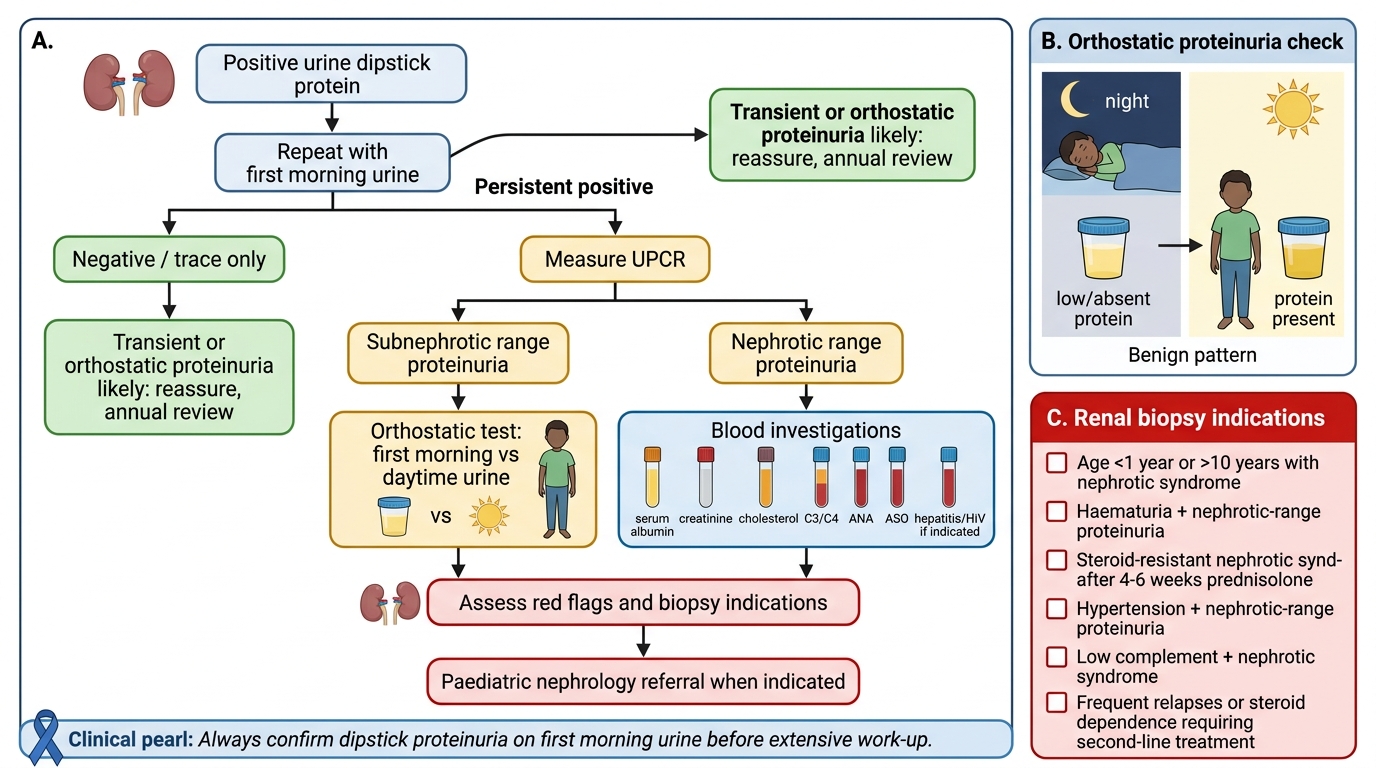
The diagnostic approach to proteinuria in a child is systematic and stepwise, designed to confirm the finding, classify it by pattern and severity, identify the probable underlying cause, and decide on the need for referral or renal biopsy. The key principle is to always perform investigations on a first morning urine before concluding that proteinuria is persistent.
The orthostatic (postural) test is the first and most important evaluation in an asymptomatic child with mild proteinuria detected on an afternoon or random sample. The child empties the bladder at bedtime, remains supine overnight, and provides the first morning void on rising (Sample A — supine). The child then remains upright and active for 2 hours and provides a second specimen (Sample B — upright). UPCR is measured on both: if Sample A UPCR is normal (<0.2) and Sample B UPCR is elevated, orthostatic proteinuria is confirmed — a benign condition requiring no treatment, only annual review.
Urine protein-to-creatinine ratio (UPCR) on a spot first morning urine is the preferred method for quantifying proteinuria in clinical practice, replacing cumbersome 24-hour urine collections. Thresholds:
• Normal: UPCR <0.2 (children >2 years)
• Subnephrotic: UPCR 0.2–2.0
• Nephrotic-range: UPCR >2.0 (equivalent to >40 mg/m²/hr on timed urine)
Blood investigations in a child with persistent proteinuria:
• Serum albumin: <2.5 g/dL confirms hypoalbuminaemia of nephrotic syndrome.
• Serum lipids: hypercholesterolaemia and hypertriglyceridaemia in nephrotic syndrome (increased hepatic lipoprotein synthesis to compensate for oncotic loss).
• Serum complement C3 and C4: C3 low in APSGN (alternative pathway); C3 + C4 low in lupus nephritis (classical pathway); normal in MCNS/FSGS.
• Serum urea, creatinine, electrolytes: assess renal function.
• ANA and anti-dsDNA: screen for lupus nephritis in girls >10 years with nephrotic syndrome or mixed nephritic-nephrotic features.
Urine microscopy: RBC casts and dysmorphic RBCs = active glomerulonephritis (not typical of pure MCNS). Oval fat bodies and fatty casts = heavy proteinuria/nephrotic syndrome.
Systematic Approach to Proteinuria in a Child
Renal biopsy indications in paediatric proteinuria:
• Age <1 year or >10 years with nephrotic syndrome (lower probability of MCNS)
• Haematuria + nephrotic-range proteinuria (suggests FSGS, lupus, or other proliferative GN)
• Steroid-resistant nephrotic syndrome (no response after 4–6 weeks of prednisolone)
• Hypertension + nephrotic range proteinuria
• Low complement + nephrotic syndrome
• Frequently relapsing or steroid-dependent nephrotic syndrome requiring second-line treatment
CLINICAL PEARL
Always confirm dipstick proteinuria on a first morning urine before investigating further. Urine concentrated during the night accurately reflects the kidney's baseline protein excretion, and orthostatic or transient proteinuria will disappear in this sample. A child with trace or 1+ proteinuria on an afternoon dipstick who has a negative first morning urine has benign orthostatic or transient proteinuria — reassure, review annually, and save the family the anxiety and cost of a renal biopsy work-up. This single clinical step prevents the majority of unnecessary referrals for mild proteinuria.