Page 8 of 30
PE20.3 | Proteinuria — SDL Guide (Part 2)
Management and Referral Criteria
Management of proteinuria in children is guided entirely by the underlying diagnosis, and the diagnostic classification built in the preceding sections now directly drives clinical decision-making. The management options span a wide range: reassurance and annual review for benign orthostatic proteinuria; dietary salt restriction and symptom-directed diuresis for mild oedema awaiting further investigation; a structured corticosteroid trial for first-presentation nephrotic syndrome in the typical age range of 1–8 years; and urgent nephrology referral for any child with features that make MCNS unlikely or that suggest a secondary, potentially progressive cause. The steroid protocol is standardised by the IAP based on ISKDC recommendations, and adherence to the correct dose and duration is important — under-dosing or early cessation is the commonest cause of treatment failure in children who would otherwise have responded. A child with any of the red-flag features listed below requires nephrology evaluation before or concurrent with initial treatment.
Proteinuria in Children: Transient, Persistent, and Nephrotic Patterns
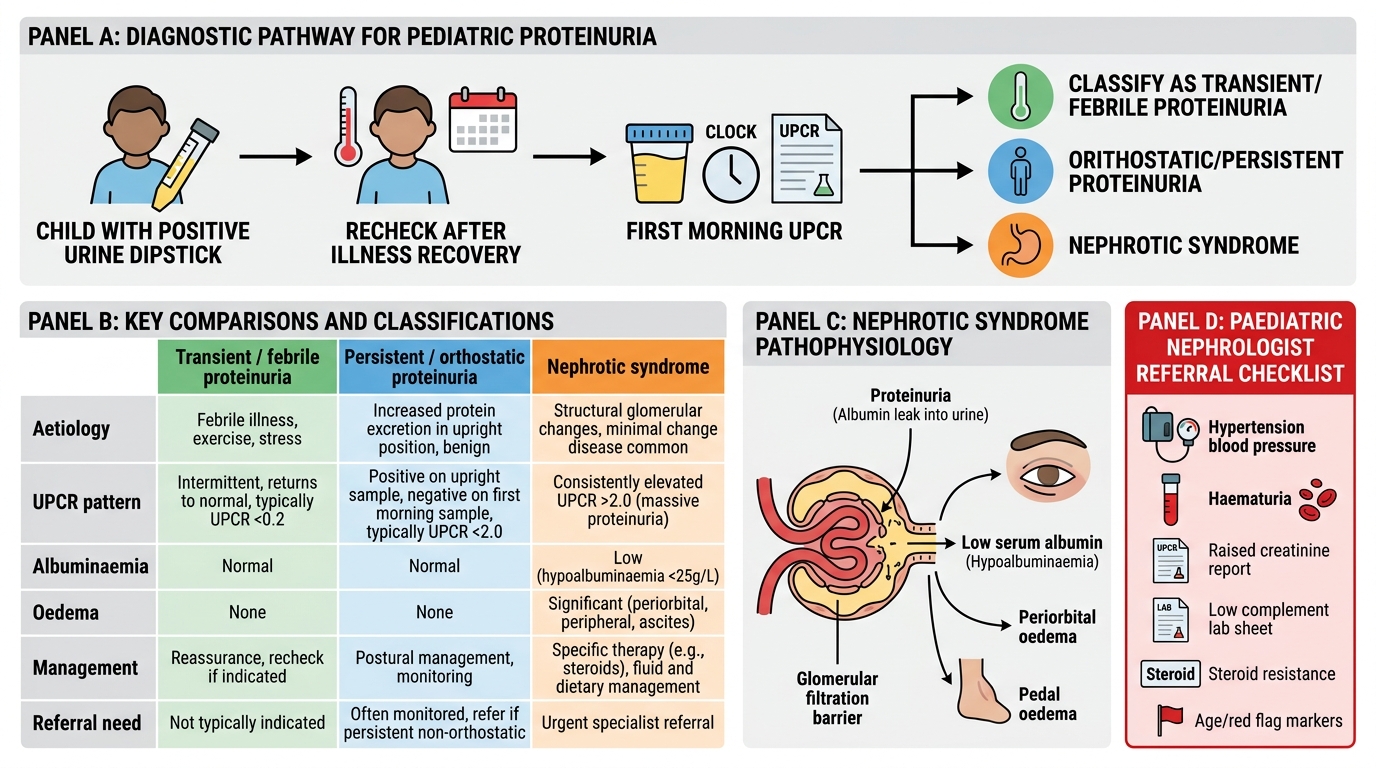
Transient / febrile proteinuria: reassure; recheck urine 2–4 weeks after recovery from the acute illness. No treatment needed.
Orthostatic proteinuria: confirm with the orthostatic test (first morning UPCR normal; upright UPCR elevated). Reassure — this is benign and does not progress. Annual urine dipstick review until it resolves spontaneously (usually by early adulthood).
First-episode nephrotic syndrome (MCNS, age 1–8 years, no red flags): treat with prednisolone 2 mg/kg/day (maximum 60 mg/day) for 4–6 weeks, then 1.5 mg/kg/alternate-day for a further 4–6 weeks (IAP standard protocol, based on ISKDC recommendations). Approximately 80–90% of children in this age group have MCNS and will enter remission within 4–6 weeks (defined as urine protein negative or trace for 3 consecutive days). Adjuncts: salt restriction, diuretics for symptomatic oedema (with caution — over-diuresis may precipitate intravascular depletion), penicillin prophylaxis against pneumococcal infection (pneumococcus is the most feared infective complication of nephrotic syndrome due to functional asplenia from peritoneal protein loss).
Steroid-resistant nephrotic syndrome (no remission after 4–6 weeks of full-dose prednisolone): refer urgently to paediatric nephrologist for renal biopsy; likely FSGS or other non-MCNS pathology.
Referral criteria to paediatric nephrology:
• Persistent proteinuria (>3 months) of any grade without an identified benign cause
• Nephrotic syndrome in any child <1 year or >10 years of age (MCNS less likely)
• Haematuria (microscopic or macroscopic) combined with nephrotic-range proteinuria
• Hypertension combined with significant proteinuria
• Low serum complement with proteinuria (suggests GN other than MCNS)
• Steroid-resistant, frequently relapsing, or steroid-dependent nephrotic syndrome
• Systemic features (rash, joint pains, fever) with proteinuria (suspect lupus, vasculitis)
• Family history of hereditary nephritis (Alport syndrome) or progressive CKD
Self-Assessment
The approach to proteinuria in children is a structured decision tree, and this module has built the branches one by one: recognition on dipstick, classification by pattern (transient versus persistent) and severity (subnephrotic versus nephrotic-range), understanding of the three pathophysiological mechanisms — glomerular filtration barrier failure, proximal tubular reabsorption failure, and overflow — and determination of the correct management pathway and referral criteria. This framework is both examination-relevant and clinically practical: you will encounter children with incidentally detected mild proteinuria in any outpatient setting, and the ability to apply the orthostatic test, interpret a UPCR result correctly, and identify the subset that needs nephrology input is a core competency of independent practice. Before attempting the self-check questions, consolidate the key pivot points: the UPCR threshold that defines nephrotic-range, the orthostatic test protocol and its interpretation, the steroid protocol for first-presentation MCNS, and the red-flag features that mandate nephrology referral rather than reassurance or a steroid trial.
- Nephrotic-range proteinuria: UPCR >2.0 on first morning urine, or >40 mg/m²/hr on timed urine.
- Normal UPCR: <0.2 in children >2 years.
- Orthostatic test: first morning void UPCR normal + upright UPCR elevated = orthostatic (benign); no treatment, annual review.
- MCNS (minimal change): commonest nephrotic in children 1–8 yr; steroid-sensitive; prednisolone 2 mg/kg/day (max 60 mg) × 4–6 weeks.
- Glomerular proteinuria = albumin predominates; tubular proteinuria = low-molecular-weight proteins, glucosuria, aminoaciduria.
- Referral triggers: persistent >3 months, age <1 or >10 yr with nephrotic syndrome, haematuria + proteinuria, hypertension + proteinuria, low complement, steroid-resistant.
SELF-CHECK
An 11-year-old girl has 3+ proteinuria on dipstick. Her first morning urine UPCR is 3.5. She has periorbital oedema, serum albumin 1.8 g/dL, serum C3 low, and ANA positive. What is the MOST appropriate next step?
A. Start prednisolone 2 mg/kg/day immediately as this is likely MCNS
B. Perform the orthostatic test and review in 3 months
C. Refer urgently to paediatric nephrology for evaluation including probable renal biopsy
D. Reassure — this is orthostatic proteinuria; no treatment needed
Reveal Answer
Answer: C. Refer urgently to paediatric nephrology for evaluation including probable renal biopsy
This child has nephrotic syndrome (UPCR >2, hypoalbuminaemia, oedema), but with multiple red flags: age >10 years (MCNS less likely), low C3 (complement pathway activation suggesting lupus or other GN), and positive ANA (autoimmune process). Standard MCNS steroid protocol is NOT appropriate here — it would delay the diagnosis of lupus nephritis or other secondary GN. Urgent nephrology referral is mandatory; renal biopsy will likely be needed. The orthostatic test is irrelevant in a child with persistent nephrotic-syndrome features.