Page 5 of 20
PE21.2 | Henoch Schonlein Purpura — SDL Guide (Part 2)
Management of HSP
The management of HSP is stratified by organ involvement and severity, and the approach has been substantially refined by randomised evidence over the past two decades. The majority of children — probably 70–80% — have mild, self-limiting disease that resolves completely with supportive care alone and never requires immunosuppression. The challenge is identifying the minority who need escalation: those with severe, refractory abdominal pain that prevents oral intake, and those with significant nephritis that risks permanent renal damage. The evidence base is clear on one critical point: corticosteroids relieve abdominal pain and arthritis effectively but do not prevent or reduce the severity of renal disease — this was definitively shown by the Ronkainen 2006 randomised trial. Keeping this distinction in mind prevents the common clinical error of giving steroids to every child with HSP out of a (misplaced) desire to protect the kidneys.
Supportive care (all patients):
• Adequate hydration and rest; encourage oral fluids
• Analgesics: NSAIDs (ibuprofen 5–10 mg/kg/dose three times daily) for joint pain and mild arthritis — effective and appropriate; avoid in children with significant renal impairment
• Paracetamol for pain where NSAIDs are contraindicated
• Monitor urine dipstick for haematuria and proteinuria weekly for at least 4–6 weeks, then monthly for 6 months
• Monitor blood pressure at each visit — hypertension is a marker of significant nephritis
Role of corticosteroids — evidence-based guidance:
Corticosteroids do NOT prevent renal disease in HSP (Ronkainen 2006 randomised trial: prednisolone did not reduce incidence of renal involvement compared to placebo at 1 year). However, corticosteroids DO significantly shorten the duration and severity of abdominal pain and arthritis. Therefore:
• Prednisolone 1–2 mg/kg/day (max 60 mg/day) for 1–2 weeks, then taper over 2 weeks: indicated for severe abdominal pain (colicky, preventing oral intake, or with bloody stools), severe arthritis limiting mobility, and scrotal involvement
• Do NOT give steroids routinely for the rash alone
• Do NOT give steroids hoping to prevent renal disease — evidence does not support this
Management of HSP nephritis:
• Mild (haematuria only, minimal proteinuria, normal BP, normal renal function): monitoring only — weekly dipstick × 4 weeks, then monthly × 6 months; refer to paediatric nephrology if proteinuria persists >4 weeks
• Moderate (persistent proteinuria <nephrotic range): nephrology referral; consider ACE inhibitor (enalapril) for renoprotection if proteinuria persists
• Severe (nephrotic-range proteinuria, hypertension, rising creatinine, ISKDC class IIIb–IV crescentic nephritis on biopsy): oral prednisolone 1–2 mg/kg/day × 4 weeks + azathioprine 2 mg/kg/day, or pulse methylprednisolone + cyclophosphamide for rapidly progressive disease; managed in paediatric nephrology unit
Follow-up schedule: urine dipstick at each visit; BP monitoring; monthly for 6 months even after apparent full recovery. If urinalysis remains completely normal for 6 months, discharge with parental advice to check urine dipstick with any febrile illness (recurrence risk ~30% within 4–6 months after first episode).
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
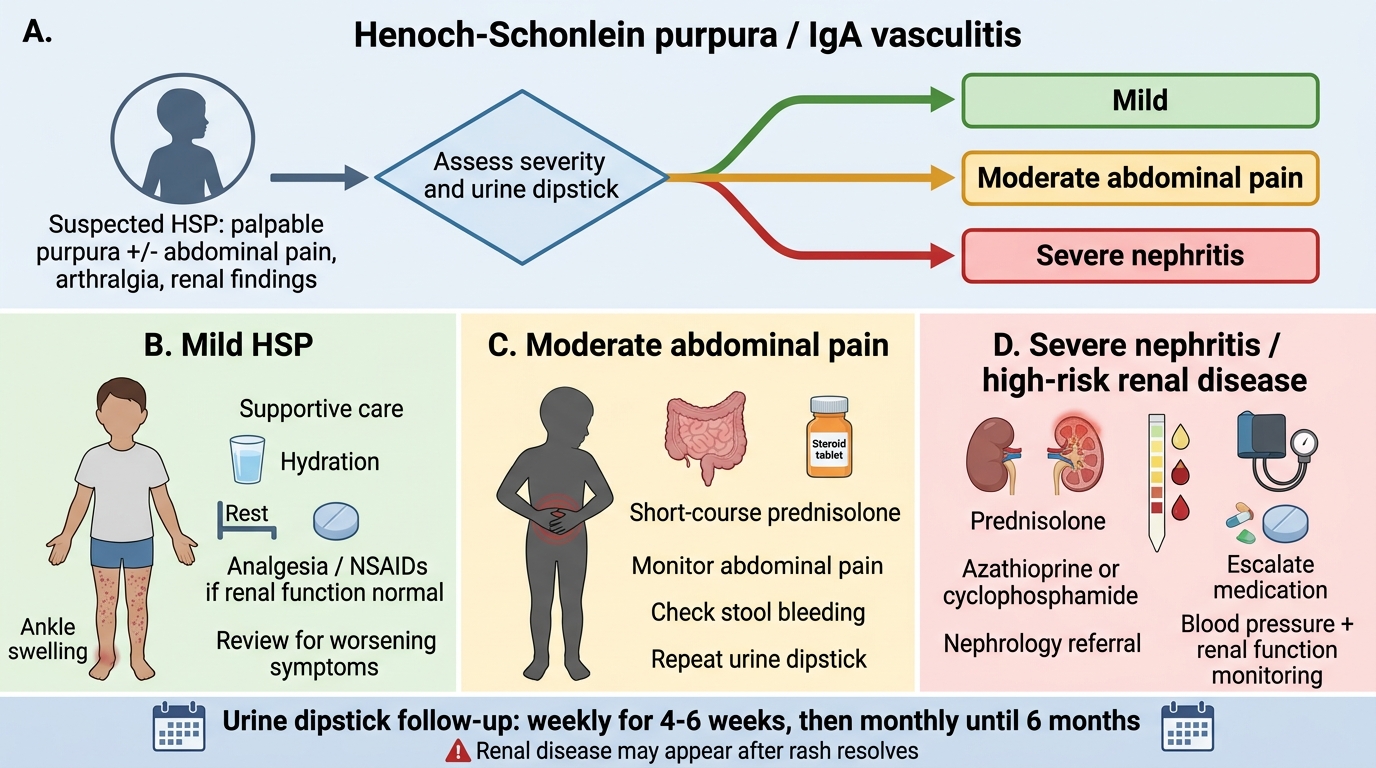
HSP Management Algorithm and Urine Monitoring
SELF-CHECK
A 5-year-old boy with HSP has been discharged after 10 days with resolution of purpura, abdominal pain, and ankle swelling. His urine dipstick at discharge showed trace blood, no protein. His mother asks whether she needs to bring him back for urine checks. What is the correct advice?
A. No further follow-up needed as the rash has resolved completely
B. Weekly urine dipstick for 4–6 weeks, then monthly for 6 months
C. Single urine check at 3 months if the child remains well
D. Only recheck if the child develops visible blood in urine
Reveal Answer
Answer: B. Weekly urine dipstick for 4–6 weeks, then monthly for 6 months
Renal involvement in HSP can appear or worsen up to 6 months after the initial presentation, even after the rash, abdominal pain, and arthritis have fully resolved. The majority of children who develop significant nephritis (heavy proteinuria, hypertension, renal impairment) do so within the first 4–6 weeks, but late onset is recognised. The SHARE guidelines and IAP recommend weekly urine dipstick monitoring for 4–6 weeks followed by monthly monitoring for 6 months. Waiting for macroscopic haematuria or symptoms is dangerous — significant nephritis is often asymptomatic until late.
Self-Assessment
Apply your knowledge to these clinical vignettes.
Case 1: A 6-year-old boy presents with a 3-day history of palpable purpura on both legs and buttocks after a sore throat 2 weeks ago. His platelet count is 220 × 10³/µL, urine dipstick shows 2+ blood, 2+ protein. BP is 106/70 mmHg. He is comfortable and eating normally. What is the diagnosis? What investigations will you order? What is your management plan?
Expected answer: Diagnosis: HSP/IgA vasculitis (mandatory criterion: palpable purpura; additional criteria: renal involvement with haematuria + proteinuria). Investigations: FBC (confirm normal platelet count — done), urine protein:creatinine ratio, renal function (urea, creatinine), ASOT, ultrasound abdomen (if pain develops). Management: admit for monitoring (2+ protein is significant), avoid NSAIDs (renal involvement present), adequate hydration, repeat urine after 24h; if proteinuria heavy or rising creatinine → refer paediatric nephrology + consider renal biopsy.
Case 2: A 7-year-old boy with HSP has severe colicky abdominal pain for 24 hours, unable to tolerate oral intake, no bloody stool, ultrasound normal. Urine dipstick: trace blood, no protein. Platelet count 250 × 10³/µL. What treatment will you prescribe, and what are you explicitly NOT trying to prevent with this treatment?
Expected answer: Prednisolone 1–2 mg/kg/day for 1–2 weeks, then taper — to reduce duration and severity of abdominal pain and enable oral intake. NOT to prevent renal disease — the Ronkainen 2006 RCT showed prednisolone does not prevent renal involvement in HSP.
Case 3: A child with HSP had resolution of purpura 3 weeks ago. Today's urine dipstick shows 3+ protein, 2+ blood. BP is 118/78 mmHg (elevated for age). What is the diagnosis and what is the next step?
Expected answer: HSP nephritis with heavy proteinuria and hypertension (marker of significant glomerular injury). Calculate protein:creatinine ratio; if nephrotic-range (>2), refer urgently to paediatric nephrology for renal biopsy and consideration of prednisolone + azathioprine or pulse therapy depending on ISKDC histological grade.