Page 1 of 20
PE21.1 | Rheumatologic Referral Approach — SDL Guide
Learning Objectives
- Enumerate the common rheumatological problems encountered in children including JIA, HSP, Kawasaki disease, SLE, and reactive arthritis
- Conduct a structured clinical assessment of a child presenting with joint pain, swelling, or systemic inflammation
- Identify red-flag features that require urgent or early referral to a paediatric rheumatologist
- Apply appropriate initial investigations and interpret key laboratory findings in the context of suspected rheumatic disease
- Describe the referral pathway and criteria for paediatric rheumatology consultation in Indian clinical settings
INSTRUCTIONS
Rheumatological diseases in children are frequently misdiagnosed or delayed because joint symptoms in paediatrics overlap with common conditions such as growing pains, trauma, and infections. Yet diseases like JIA and SLE can cause irreversible joint damage, blindness from silent uveitis, or end-organ failure if treatment is delayed even by weeks. As a final-year student and future primary-care physician, your ability to recognise the clinical pattern, perform a focused assessment, and refer promptly is the most impactful intervention you can make for these children. This module builds the skill of structured recognition and referral — from the first clinical encounter to the moment you hand over to a specialist.
References
- Ghai Essential Pediatrics, 9th Ed, Ch 17 — Rheumatic Diseases (textbook)
- Nelson Textbook of Pediatrics, 21st Ed, Ch 180-184 — Rheumatic Diseases of Childhood (textbook)
- IAP Guidelines on Juvenile Idiopathic Arthritis, 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old girl is brought to your clinic by her parents with a 10-week history of morning stiffness and swelling of both knees and the left ankle. Her parents initially attributed this to growing pains and sports activity. She has no fever and her appetite is normal. On examination she has warm, swollen knee joints with restricted range of movement, and you notice subtle whitish deposits in her left eye on torch examination. Her ESR is 58 mm/hr and ANA is reported as positive at 1:320. Her parents ask, 'Is this serious? She is only nine.' You know that she likely has oligoarticular JIA with anterior uveitis — and that every week without treatment carries risk of irreversible visual loss. What should you do next?
WHY THIS MATTERS
Paediatric rheumatic diseases are not rare — juvenile idiopathic arthritis (JIA) is the most common chronic inflammatory arthritis in childhood, affecting approximately 1 in 1,000 children in India. HSP (IgA vasculitis) is the most common systemic vasculitis in childhood. SLE and Kawasaki disease, though less common, carry high morbidity when delayed. The primary-care physician is almost always the first point of contact. Recognising the difference between benign self-limiting joint pain and an evolving inflammatory arthropathy determines whether a child receives disease-modifying treatment in time or presents years later with joint damage. The skill of structured rheumatological assessment and appropriate referral is therefore central to paediatric practice at every level of the health system.
RECALL
Before proceeding, activate your prior knowledge. Recall from Anatomy: the structure of synovial joints — articular cartilage, synovium, joint capsule, and the nutrient supply of cartilage by synovial fluid. Recall from Physiology: the normal immune response, the role of T-helper cells (Th1/Th17) in driving synovial inflammation, and the concept of molecular mimicry in autoimmune disease. Recall from your clinical training: how to examine a joint (look–feel–move), how to differentiate an effusion from synovial thickening, and the basic interpretation of inflammatory markers such as ESR, CRP, CBC, and ANA. These form the foundation onto which this module builds the clinical skill of paediatric rheumatological assessment.
Common Rheumatological Problems in Children
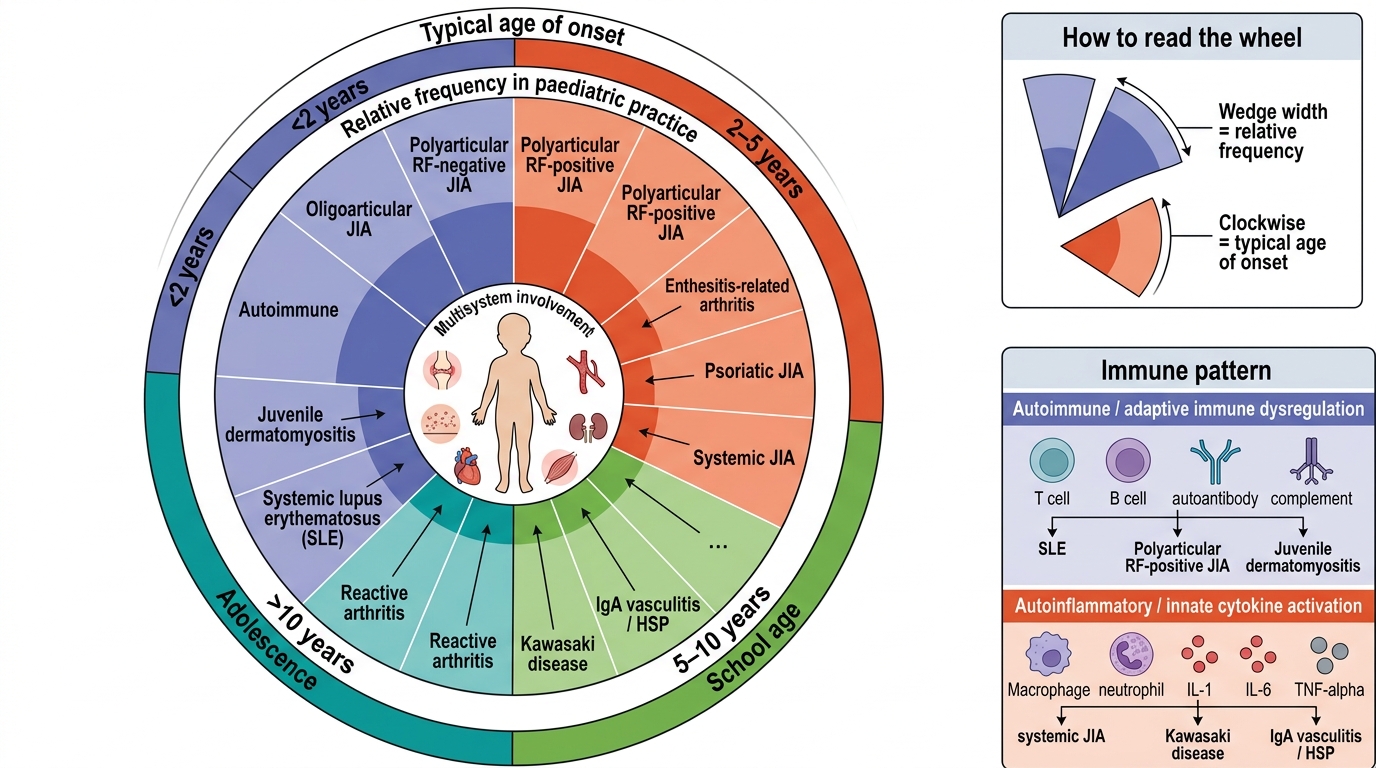
Juvenile idiopathic arthritis (JIA) is the umbrella term for a heterogeneous group of chronic arthritides beginning before age 16 years and persisting for at least 6 weeks, classified by the International League of Associations for Rheumatology (ILAR) into distinct subtypes based on joint count in the first 6 months, systemic features, and serology. Understanding these subtypes is clinically essential because their prognosis, complications, and treatment differ substantially.
Oligoarticular JIA (≤4 joints in the first 6 months) is the most common subtype in India, accounting for approximately 50–60% of cases. It predominantly affects young girls, usually involves large joints (knees, ankles), and is strongly associated with antinuclear antibody (ANA) positivity and the risk of chronic anterior uveitis — which is often asymptomatic ('white eye') and can cause blindness if missed. Polyarticular JIA involves ≥5 joints in the first 6 months and is further divided into RF-positive (similar to adult RA, more erosive) and RF-negative (better prognosis). Systemic JIA (sJIA) presents with daily spiking fever, an evanescent salmon-pink rash, and arthritis; serositis and hepatosplenomegaly may occur; macrophage activation syndrome (MAS) is a life-threatening complication.
Beyond JIA, reactive arthritis follows a preceding infection (streptococcal pharyngitis, enteric Salmonella/Shigella, Chlamydia) and typically presents as an asymmetric oligoarthritis 1–4 weeks after the trigger, often self-limiting in <3 months. Henoch Schönlein Purpura (HSP/IgA vasculitis) involves palpable purpura (mandatory), often with arthritis, abdominal pain, and renal involvement. Kawasaki disease is a medium-vessel vasculitis in young children (<5 years) with fever ≥5 days plus mucocutaneous features, and its greatest danger is coronary artery aneurysm. Systemic lupus erythematosus (SLE) in children tends to be more severe than adult SLE, with higher rates of renal and CNS involvement. Juvenile dermatomyositis (JDM) presents with proximal muscle weakness and characteristic skin changes (Gottron's papules, heliotrope rash).
| JIA Subtype | Joint Count (6 mo) | Age/Sex | ANA | RF | Key Complication |
|---|---|---|---|---|---|
| Oligoarticular | ≤4 | Young girls | ++ | – | Chronic uveitis |
| Polyarticular RF– | ≥5 | School-age girls | +/– | – | Joint damage, moderate |
| Polyarticular RF+ | ≥5 | Older girls | +/– | + | Early erosive disease |
| Systemic (sJIA) | Variable | Equal sex | – | – | MAS, systemic damage |
| Enthesitis-related | ≥1 + enthesitis | Older boys | – | – | Sacroiliitis |
Spectrum of Common Paediatric Rheumatological Conditions
Pathophysiological and Immunological Basis
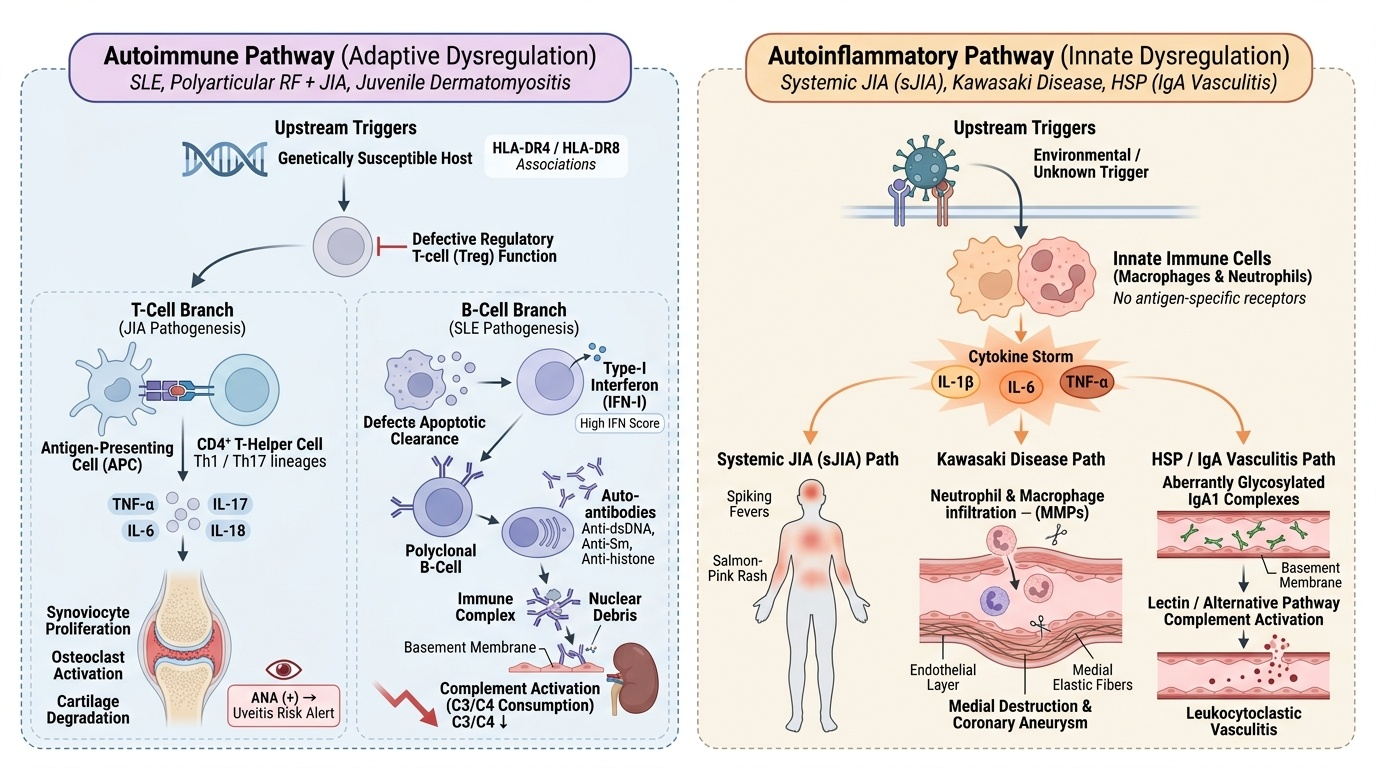
Understanding why children develop rheumatic diseases requires integrating basic immunology with clinical observation. Most paediatric rheumatic diseases fall into two broad immunological categories: autoimmune (adaptive immune dysregulation with auto-antibody production — SLE, polyarticular RF+ JIA, juvenile dermatomyositis) and autoinflammatory (innate immune dysregulation with excessive IL-1β/IL-6/TNF-α — systemic JIA, Kawasaki disease, HSP, familial Mediterranean fever).
Provided image
In oligoarticular and polyarticular JIA, activated CD4+ T-helper cells (predominantly Th1 and Th17 lineages) infiltrate the synovium and drive production of pro-inflammatory cytokines including TNF-α, IL-6, IL-17, and IL-18. These cytokines stimulate synoviocyte proliferation, osteoclast activation, and cartilage degradation. Molecular mimicry and defects in regulatory T-cell (Treg) function are proposed triggers in genetically susceptible individuals (HLA-DR4/DR8 associations). ANA in oligoarticular JIA marks a specific immune signature — its positivity alerts the clinician to uveitis risk, not disease severity.
In SLE, a failure of apoptotic debris clearance leads to sustained type-I interferon production and polyclonal B-cell activation, generating auto-antibodies against nuclear antigens (anti-dsDNA, anti-Sm, anti-histone). Immune complex deposition triggers complement activation (C3/C4 consumption) in kidneys, skin, and CNS. Paediatric SLE carries higher interferon scores and more aggressive organ involvement than adult-onset disease.
In Kawasaki disease, an unknown trigger drives massive innate immune activation in genetically susceptible children, generating an acute-phase response and vasculitis of medium-calibre vessels including the coronary arteries. Coronary aneurysm formation involves neutrophil and macrophage infiltration of the vessel wall, matrix metalloproteinase release, and medial destruction.
In HSP (IgA vasculitis), aberrantly glycosylated IgA1 deposits in small-vessel walls — particularly in skin, gut, joints, and kidney mesangium — triggering leukocytoclastic vasculitis and complement activation via the lectin/alternative pathways.
SELF-CHECK
A 4-year-old boy presents with fever for 7 days, bilateral conjunctivitis, a polymorphous rash on the trunk, and cracked red lips. His CRP is 120 mg/L and ESR is 80 mm/hr. What is the most important reason for urgent referral to a paediatric cardiologist?
A. Risk of acute glomerulonephritis
B. Risk of coronary artery aneurysm formation
C. Risk of pericardial effusion causing tamponade
D. Risk of mitral valve regurgitation
Reveal Answer
Answer: B. Risk of coronary artery aneurysm formation
This child meets criteria for Kawasaki disease (fever ≥5 days plus ≥4 of 5 mucocutaneous features). The most important and potentially fatal complication is coronary artery aneurysm (CAA), occurring in 15–25% of untreated cases. Early echocardiography and IVIG within 10 days of fever onset dramatically reduces CAA risk. While pericardial effusion can occur in Kawasaki disease, CAA is the defining and most dangerous complication requiring urgent cardiological evaluation.
Systematic Clinical Approach to the Child with Joint or Systemic Inflammation
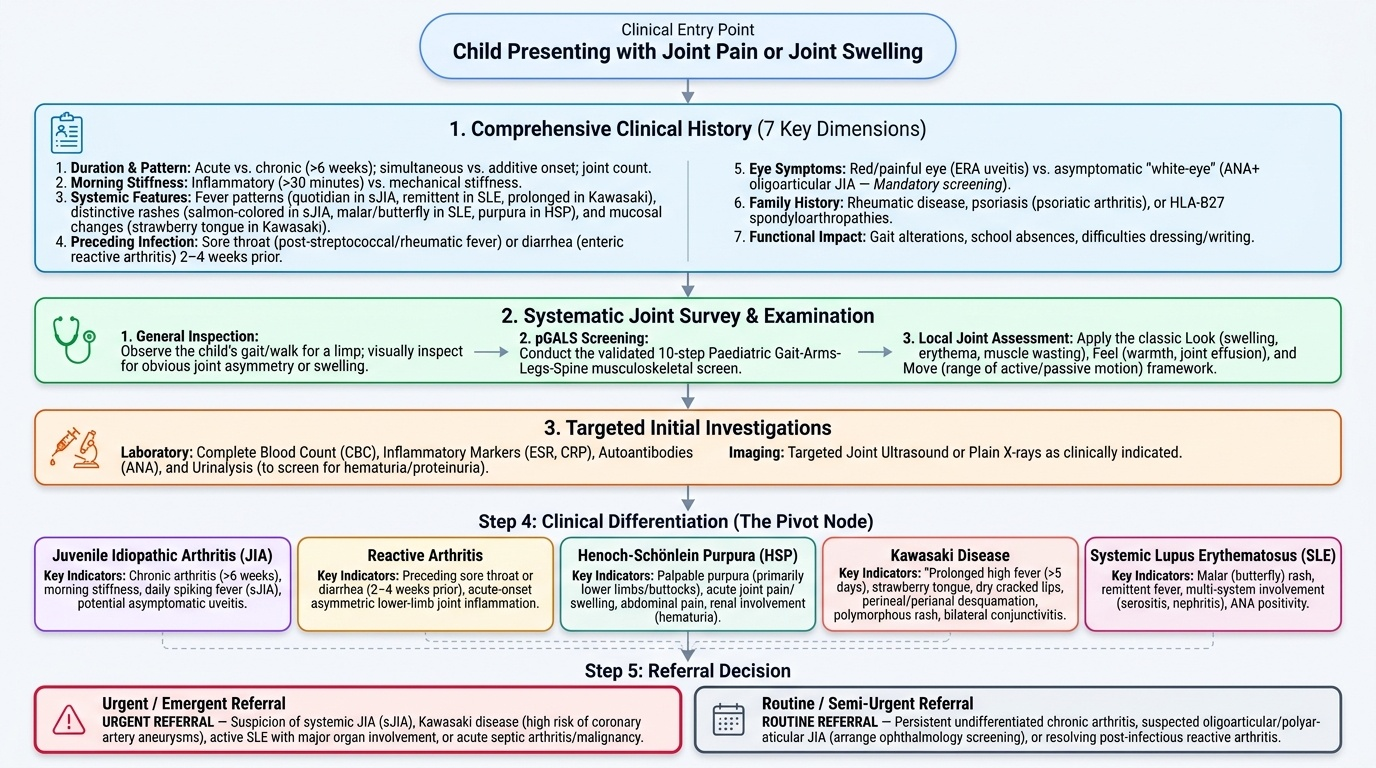
A structured clinical approach enables you to differentiate the multiple causes of joint symptoms in children efficiently. The assessment begins with the history, moves to a systematic examination, and is completed by targeted investigations — each step narrowing the differential and guiding the referral decision.
Provided image
History — seven key dimensions: (1) Duration and pattern of joint involvement: which joints, how many, was onset simultaneous or additive? (2) Morning stiffness: duration >30 minutes favours inflammatory arthritis over mechanical. (3) Systemic features: fever pattern (quotidian daily spiking in sJIA; remittent in SLE; prolonged in Kawasaki), rash (evanescent salmon-coloured rash in sJIA; butterfly malar rash in SLE; palpable purpura in HSP; periorbital heliotrope in JDM; perineal/perianal desquamation in Kawasaki), mucosal changes (strawberry tongue in Kawasaki), lymphadenopathy, serositis symptoms. (4) Preceding infection: sore throat 2–4 weeks ago (post-streptococcal reactive arthritis, rheumatic fever), diarrhoea (enteric reactive arthritis). (5) Eye symptoms: red painful eye (acute anterior uveitis in enthesitis-related arthritis) vs asymptomatic white-eye (chronic uveitis in ANA+ oligoarticular JIA — MUST be screened regardless of symptoms). (6) Family history of rheumatic disease, psoriasis (psoriatic arthritis), or HLA-B27-associated spondyloarthropathy. (7) Functional impact: school attendance, gait, ability to dress/write.
Examination — systematic joint survey: Begin with a general inspection — does the child walk with a limp? Is there joint swelling visible? Use the pGALS (paediatric Gait-Arms-Legs-Spine) screening tool, a validated 10-step paediatric musculoskeletal examination. For each affected joint: Look (swelling, erythema, muscle wasting, leg-length discrepancy), Feel (warmth by dorsum of hand, synovial thickening vs effusion, tenderness), Move (active then passive range; restricted motion confirms pathological joint). Extra-articular examination: skin (rash type and distribution), eye examination with torchlight (basic) and request slit-lamp if ANA positive, lymphadenopathy, hepatosplenomegaly, BP (hypertension in renal SLE), cardiac murmur/pericardial rub.
Initial investigations in primary care: Full blood count (anaemia of chronic disease, leukopenia/thrombocytopenia in SLE, thrombocytosis in Kawasaki); ESR and CRP (inflammatory markers — elevated in all active disease); ANA (screening test — low specificity, high sensitivity for systemic autoimmune disease); urine routine + microscopy (haematuria/proteinuria in SLE/HSP nephritis); throat swab + ASOT/anti-DNase B if post-streptococcal arthritis suspected; echocardiogram if Kawasaki disease suspected.