Page 2 of 20
PE21.1 | Rheumatologic Referral Approach — SDL Guide (Part 2)
Interpreting Investigations and Red-Flag Features
Interpreting investigations in paediatric rheumatology requires understanding that no single test diagnoses JIA, SLE, or HSP in isolation — diagnoses are clinical, with investigations serving to confirm, classify, and monitor. However, certain findings are highly informative and certain patterns should trigger immediate action.
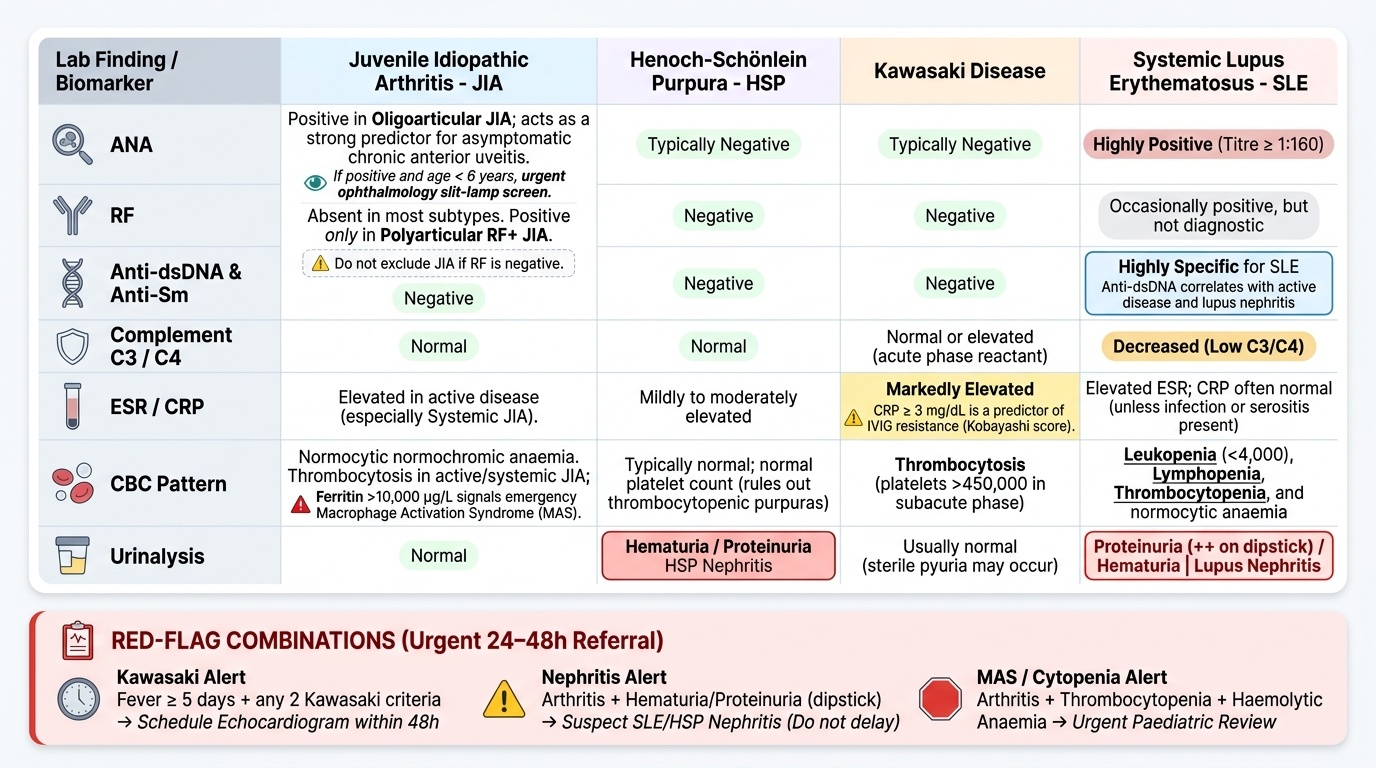
Provided image
ANA (antinuclear antibody): A positive titre ≥1:160 is clinically significant. ANA positivity in a child with arthritis is the most important predictor of asymptomatic chronic anterior uveitis (particularly in oligoarticular JIA) — these children MUST be referred for slit-lamp examination by an ophthalmologist, initially every 3 months (high-risk ANA+ < 6 years at onset), regardless of whether the eye looks normal externally.
Anti-dsDNA and complement C3/C4: Anti-dsDNA antibodies are highly specific for SLE (but low sensitivity); low C3/C4 indicates active complement consumption and correlates with lupus nephritis activity. Anti-Sm is also specific for SLE. In a child with suspected SLE, always order: ANA, anti-dsDNA, anti-Sm, complement C3/C4, urinalysis (proteinuria/haematuria), and CBC with differential.
RF (rheumatoid factor): RF positivity in JIA designates polyarticular RF+ subtype — the closest JIA subtype to adult RA. RF is absent in most JIA subtypes. Do not exclude JIA because RF is negative.
ESR/CRP: Both elevated in active inflammation; CRP returns to normal faster after treatment. In Kawasaki, CRP >3 mg/dL is one Kobayashi score predictor of IVIG resistance.
CBC pattern: Normocytic normochromic anaemia of chronic disease in JIA/SLE; leukopenia (<4,000) and lymphopenia in SLE (SLICC criterion); thrombocytopenia in SLE; thrombocytosis (platelets often >450,000) in Kawasaki and sJIA; elevated ferritin (>10,000 µg/L) in sJIA-associated macrophage activation syndrome (MAS) — a haematological emergency.
Red-flag features requiring urgent referral (same day to within 48 hours):
• Fever ≥5 days + any 2 of the 5 Kawasaki criteria → echocardiogram within 48 hours
• Arthritis + haematuria/proteinuria (++protein on dipstick) → SLE or HSP nephritis, do not delay
• Arthritis + thrombocytopenia + haemolytic anaemia → possible MAS or SLE — urgent paediatric review
• ANA+ arthritis + child <6 years → ophthalmology referral within 1 month
• Back pain + sacroiliitis features in a boy >10 years → paediatric rheumatology within 1 month
• Proximal muscle weakness + heliotrope rash → juvenile dermatomyositis, cannot wait months
CLINICAL PEARL
The most dangerous miss in paediatric rheumatology is asymptomatic uveitis in ANA-positive oligoarticular JIA. The eye looks completely normal to the child, the parents, and the clinician using a torch — yet the anterior chamber is inflamed and synechiae are forming. The rule is simple: every child with JIA who is ANA-positive, female, and younger than 6 years at disease onset requires slit-lamp screening every 3 months for the first 4 years, then every 6 months thereafter. Do not wait for a red eye, photophobia, or visual complaint. By then, band keratopathy and cataract may already be irreversible.
Referral Pathways and Criteria for Paediatric Rheumatology
The decision to refer and the timing of referral are the primary clinical skills this module develops. In India, paediatric rheumatology is a subspeciality available at tertiary and medical college hospitals; most primary-care and secondary-care paediatricians see children with rheumatic diseases first and must initiate assessment and urgent management before the subspecialty encounter. Knowing when to refer, what urgency to apply, and what to do in the interim is therefore a core competency for every paediatrician, not just for rheumatologists. A delayed referral in JIA risks blindness (uveitis), joint destruction, and growth failure; a delayed referral in Kawasaki disease risks coronary artery aneurysm; a delayed referral in lupus nephritis risks renal failure. The following criteria and pathways are based on IAP and international ACR/EULAR paediatric rheumatology guidance adapted to the Indian context.
Criteria for referral to paediatric rheumatology (when any one criterion is met):
1. Arthritis persisting for >6 weeks with no identifiable infectious cause → formal evaluation for JIA
2. ANA or anti-dsDNA positivity in any child with systemic symptoms (rash, fever, renal) → SLE evaluation
3. Suspected Kawasaki disease → rheumatology + cardiology same visit
4. Arthritis + any organ involvement (renal, cardiac, CNS, haematological) → same-day or next-day referral
5. Suspected juvenile dermatomyositis (proximal weakness + skin) → within 1 week (risk of aspiration pneumonia from pharyngeal involvement)
6. Chronic musculoskeletal pain lasting >3 months with normal investigations AND significant functional impairment → paediatric pain/rheumatology for fibromyalgia/chronic pain evaluation
What to do while awaiting referral:
• Start NSAIDs (naproxen 10–15 mg/kg/day in 2 divided doses, or ibuprofen 30–40 mg/kg/day in 3 doses) for symptomatic relief while investigating
• Do NOT start corticosteroids empirically without a diagnosis — steroids can mask the diagnostic pattern of systemic JIA and MAS, and suppress the fever of Kawasaki disease making it harder to diagnose
• If Kawasaki disease is strongly suspected and referral will be delayed >24 h: aspirin 30–50 mg/kg/day in 4 doses (anti-inflammatory dose) can be started, but IVIG must not be delayed beyond 10 days from fever onset
• Document the joint map (which joints, degree of swelling, ROM) to provide the specialist with a baseline
• Ensure ophthalmology referral is initiated concurrently for ANA+ JIA — do not wait for the rheumatologist to order this
Referral letter must include: duration of symptoms, joint map, systemic features, investigations done + results, medications started, vaccination status (JIA patients will require modified vaccination schedules once on immunosuppression), and family contact information for follow-up tracking.
In resource-limited settings where paediatric rheumatology is not immediately accessible, telemedicine consultation with a rheumatologist at a tertiary centre is increasingly available and is appropriate for non-emergency stable cases while arranging in-person referral.
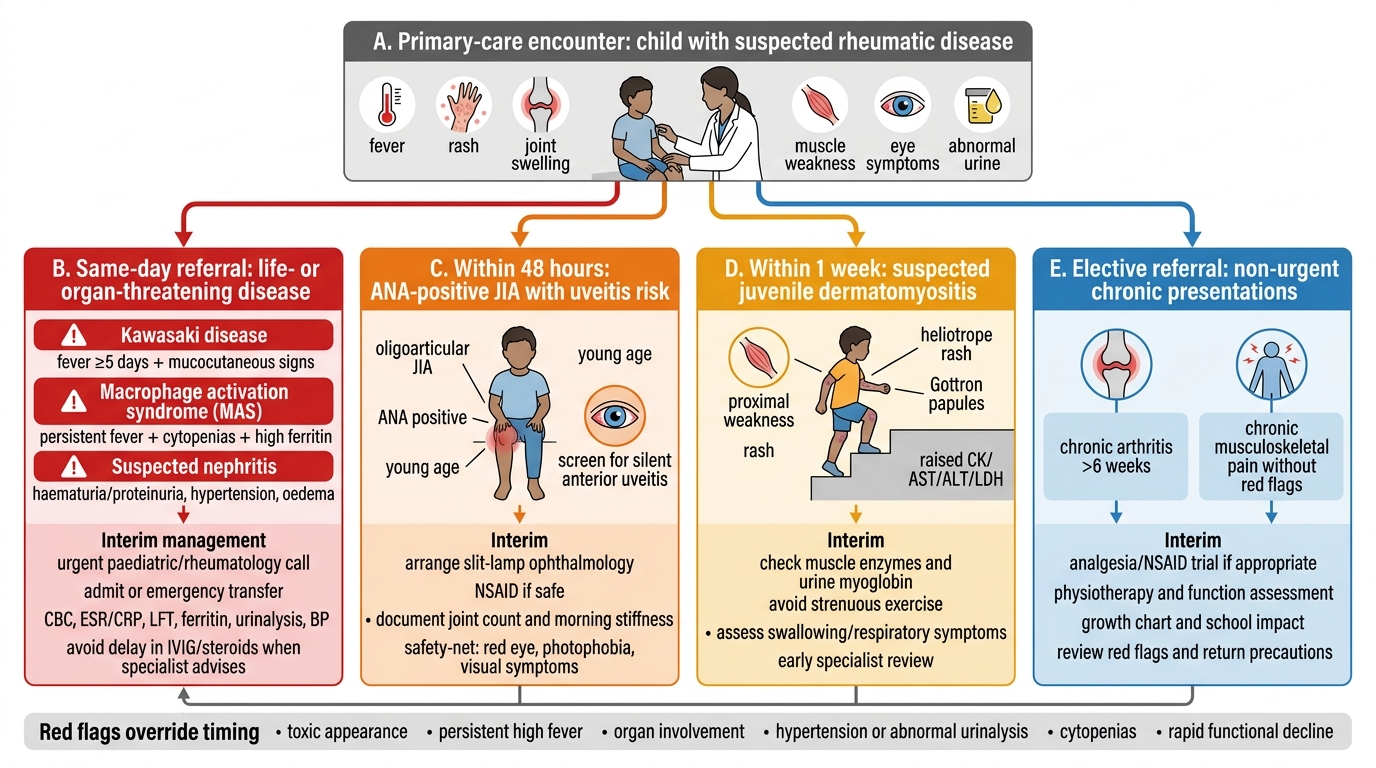
Paediatric Rheumatic Disease Referral Pathway
SELF-CHECK
A 7-year-old girl has had swelling of the right knee for 9 weeks. She has no fever, rash, or systemic symptoms. ESR is 42 mm/hr, ANA is positive at 1:320, and her eyes look completely normal. What is the most appropriate next single action?
A. Reassure parents that the eye is normal and follow up in 6 months
B. Start prednisolone 1 mg/kg/day to suppress inflammation
C. Refer urgently for slit-lamp ophthalmological examination
D. Obtain X-ray of the knee and wait for the result before referring
Reveal Answer
Answer: C. Refer urgently for slit-lamp ophthalmological examination
This child has features of oligoarticular JIA (arthritis <4 joints, >6 weeks, ANA positive, young girl). The most dangerous complication is asymptomatic chronic anterior uveitis, which causes blindness and is externally invisible — the torch examination gives false reassurance. ANA positivity in a young child with JIA mandates urgent slit-lamp ophthalmological examination within 1 month (or sooner at high-risk centres). Steroids should not be started without diagnosis, and the eye referral must not be deferred.
Self-Assessment
Test your understanding of the clinical approach to paediatric rheumatological referral with these scenario-based questions.
Case 1: An 8-year-old girl presents with morning stiffness and swollen knee and ankle (3 joints) for 8 weeks. ANA is positive at 1:320. Hb 10.8 g/dL, ESR 55 mm/hr. Urinalysis normal. Both eyes externally normal. What is the likely JIA subtype? What is the single most important referral you must initiate and why?
Expected answer: Oligoarticular JIA (≤4 joints, >6 weeks, child <16, ANA+). Most important referral = ophthalmology slit-lamp (not rheumatology first) because ANA-positive oligoarticular JIA in a girl <6 years at onset carries highest uveitis risk — though at 8 years risk is lower, ANA positivity still mandates screening. Rheumatology referral also required for disease-modifying therapy.
Case 2: A 3-year-old boy has had fever for 6 days, bilateral conjunctival injection, strawberry tongue, erythema and oedema of hands, and a maculopapular rash on the trunk. Platelet count is 520 × 10³/µL. What is the diagnosis, what investigation is most urgent, and what is the timing constraint for treatment?
Expected answer: Kawasaki disease (fever ≥5 days + 4/5 criteria: conjunctivitis, mucositis/strawberry tongue, extremity changes, rash). Most urgent investigation = echocardiogram. Treatment with IVIG 2 g/kg single infusion + aspirin must be given within 10 days of fever onset to prevent coronary artery aneurysm.
Case 3: A 12-year-old girl presents with fatigue, a butterfly-shaped facial rash, joint pain (both wrists, fingers), and 2+ protein on urine dipstick. CBC shows Hb 9.2 g/dL, WBC 3,200/µL, platelets 140 × 10³/µL. What diagnosis must be excluded, what investigations should you order, and what is the urgency of referral?
Expected answer: SLE must be excluded (butterfly rash, polyarthritis, leukopenia, anaemia, proteinuria — multiple SLICC criteria). Order: ANA, anti-dsDNA, anti-Sm, complement C3/C4, 24-hour urine protein or protein:creatinine ratio, serum creatinine. Urgency = same-day referral to paediatric nephrology + rheumatology because proteinuria in SLE indicates lupus nephritis which can progress to renal failure rapidly without treatment.
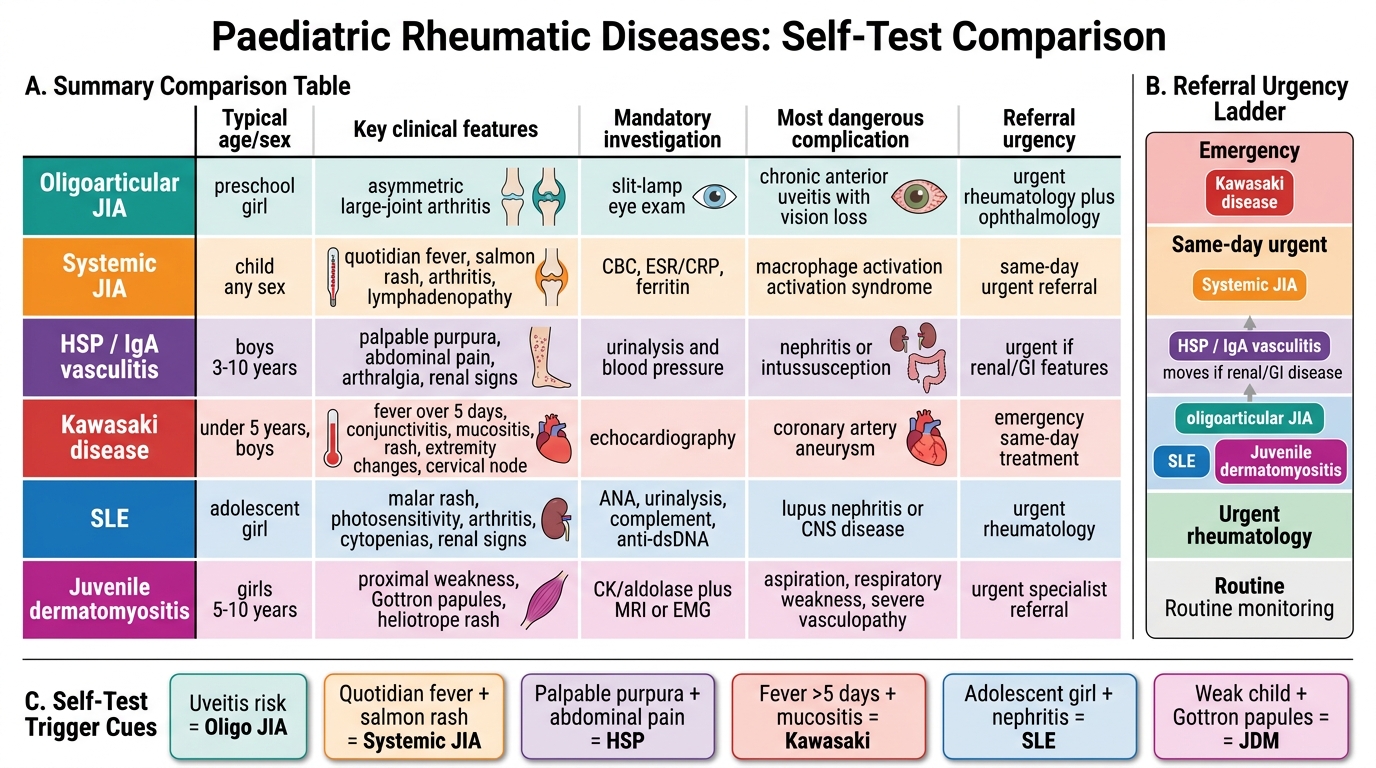
Paediatric Rheumatic Diseases: Self-Test Comparison