Page 1 of 31
PE22.1 | Acyanotic Heart Disease — SDL Guide
Learning Objectives
- Describe the haemodynamic consequences of left-to-right shunt lesions (VSD, ASD, PDA) and obstructive lesions (pulmonary stenosis, aortic stenosis, coarctation of the aorta)
- Identify the clinical presentation and characteristic murmur of each major acyanotic congenital heart defect
- Explain the mechanism and clinical features of Eisenmenger syndrome as a complication of uncorrected L→R shunts
- Select appropriate investigations (ECG, CXR, echocardiography) and interpret their findings in acyanotic CHD
- Outline the medical, interventional, and surgical management of acyanotic CHD using weight-based paediatric dosing
INSTRUCTIONS
Acyanotic congenital heart disease comprises the majority of all congenital cardiac defects and represents one of the most important causes of cardiac failure and recurrent chest infections in infancy. Understanding the haemodynamic basis of each lesion — the direction of the shunt, its magnitude, and its consequences on the pulmonary and systemic circulations — is the conceptual foundation for rational clinical diagnosis and management. This module is directly testable in university examinations and, more importantly, forms the basis for recognising and urgently referring a child whose uncorrected defect is progressing toward the catastrophic and irreversible Eisenmenger syndrome.
References
- Ghai Essential Pediatrics, 9th edition, Ch 14 (Cardiovascular System) (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 457–461 (Congenital Heart Disease) (textbook)
- IAP Guidelines on Congenital Heart Disease and SBE Prophylaxis, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 4-month-old girl is brought to paediatric OPD by her mother, who reports that the baby has not been gaining weight as expected and sweats excessively during feeds. On examination, the child is tachypnoeic with a respiratory rate of 60/min, has a precordial bulge, and a loud pansystolic murmur is heard at the lower left sternal border radiating to the axilla. The liver is palpable 4 cm below the costal margin. Her birth weight was 3.1 kg and she now weighs only 4.0 kg at 4 months — far below the expected 6 kg. What is the most likely diagnosis, and why has this infant developed congestive cardiac failure?
WHY THIS MATTERS
Congenital heart disease (CHD) affects approximately 8–10 per 1000 live births in India, and the majority — nearly 70–80% — are acyanotic defects. Among all paediatric admissions for cardiac causes, acyanotic CHD accounts for a significant proportion of infants presenting with failure to thrive, recurrent lower respiratory tract infections, and congestive cardiac failure in the first year of life. Crucially, many of these lesions are curable with early surgical or catheter-based intervention; however, if undetected and uncorrected, they lead to Eisenmenger syndrome — an irreversible, inoperable complication that converts a curable condition into a fatal one. The NMC competency PE22.1 requires you to describe not just the clinical features but the underlying haemodynamic mechanism — because haemodynamics determines which child needs urgent referral today versus watchful waiting.
RECALL
Before proceeding, recall from your Anatomy and Physiology courses: the fetal circulation has two physiological right-to-left shunts — the foramen ovale (atrial level) and the ductus arteriosus (between the pulmonary artery and aorta). Both normally close after birth as pulmonary vascular resistance drops. The Fick principle states that cardiac output equals oxygen consumption divided by the arterio-venous oxygen difference — a concept used in cardiac catheterisation to measure Qp:Qs (the ratio of pulmonary-to-systemic blood flow). Recall also that the left heart normally operates at a higher pressure than the right, and the systemic vascular resistance greatly exceeds the pulmonary vascular resistance in the postnatal state. This pressure gradient — higher left than right — is what drives a left-to-right shunt.
Clinical Presentation of Acyanotic CHD
The clinical presentation of acyanotic congenital heart disease depends critically on the type of lesion — whether it causes a left-to-right shunt (increasing pulmonary blood flow) or an obstruction (impeding outflow without an initial shunt). This distinction shapes everything from the age of presentation to the character of the murmur and the likelihood of cardiac failure in infancy. A thorough understanding of these patterns allows the clinician to formulate a likely diagnosis at the bedside before any investigation.
Provided image
Left-to-right shunt lesions (VSD, ASD, PDA) share a common symptom cluster: failure to thrive (poor weight gain, inadequate feeding), recurrent lower respiratory tract infections (due to pulmonary oedema and fluid in the lungs making the child susceptible), exertional dyspnoea manifest as feeding fatigue and diaphoresis, and eventually congestive cardiac failure in large undetected defects. Infants with large VSDs or PDAs may present as early as 4–8 weeks of life as pulmonary vascular resistance physiologically drops after birth and the shunt increases.
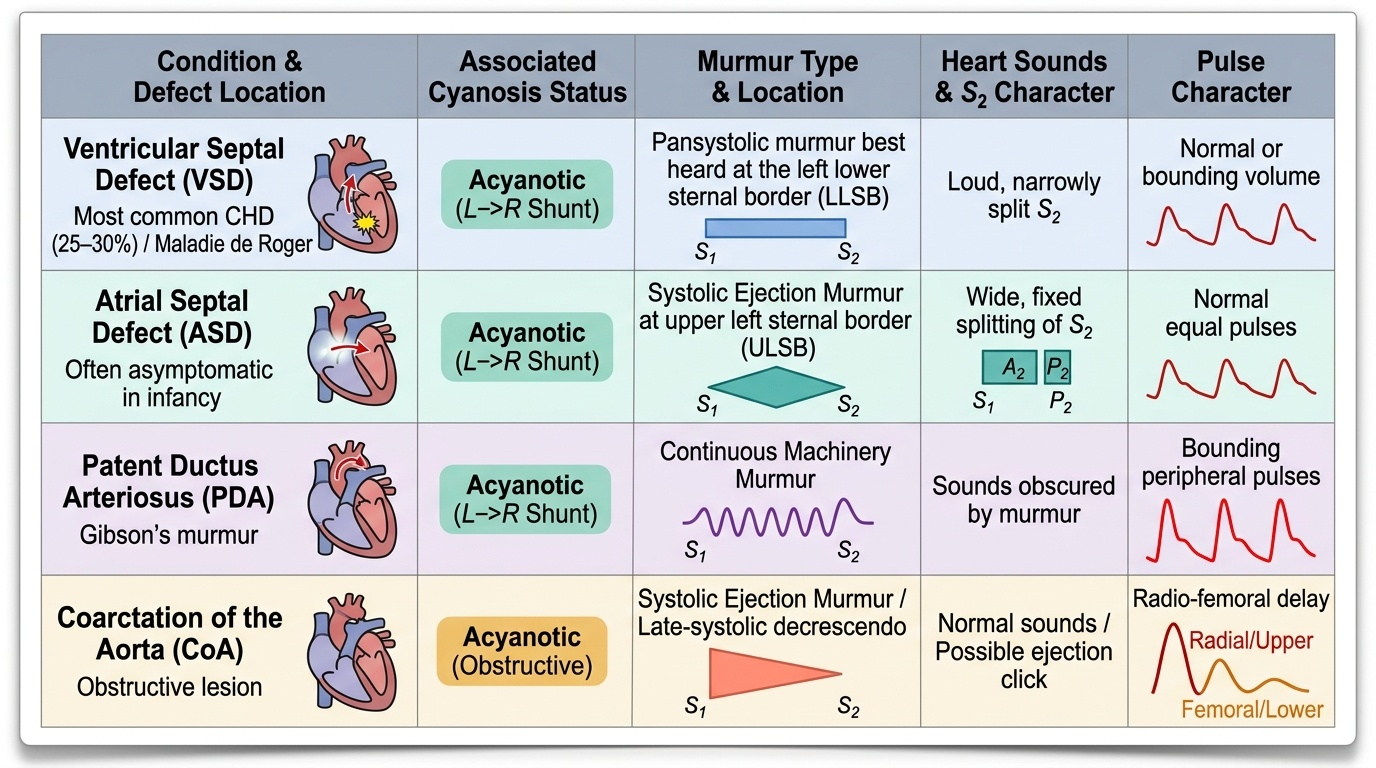
Ventricular Septal Defect (VSD): The most common CHD (25–30% of all CHD). A small VSD presents as an incidental asymptomatic pansystolic murmur at the lower left sternal border (LLSB) radiating to the axilla — the Maladie de Roger. A large VSD produces symptoms of cardiac failure, a thrill at LLSB, and a mid-diastolic rumble at the apex (due to high pulmonary flow across the mitral valve — a functional mitral stenosis). The S2 is loud and may be narrowly split due to pulmonary hypertension.
Atrial Septal Defect (ASD): Usually asymptomatic in infancy; symptomatic presentation is more common after the first decade. The cardinal signs are: wide and fixed splitting of S2 (hallmark, due to delayed right ventricular emptying), a pulmonary ejection systolic murmur at the upper left sternal border (due to increased flow across the pulmonary valve, not the defect itself), and a mid-diastolic tricuspid murmur in large ASDs (increased flow across the tricuspid valve). ASD is often detected incidentally on chest X-ray or examination.
Patent Ductus Arteriosus (PDA): The pathognomonic finding is a continuous machinery murmur heard best at the upper left sternal border/infraclavicular area, peaking at S2, heard throughout systole and diastole (Gibson murmur). Large PDAs produce bounding pulses, a wide pulse pressure, and a hyperactive precordium. Premature neonates are especially at risk because ductal closure is often delayed.
Obstructive lesions (Pulmonary Stenosis, Aortic Stenosis, Coarctation of the Aorta) typically present with a murmur detected incidentally, as they do not cause increased pulmonary flow or early cardiac failure unless severe. PS produces an ejection systolic murmur at the upper left sternal border with a widely split S2 (delayed pulmonary component). Coarctation of the Aorta (CoA) has the distinctive sign of upper limb hypertension with reduced/absent femoral pulses — the femoral-radial pulse delay is pathognomonic. Severe CoA can present as a sick neonate with cardiovascular collapse as the ductus closes.
SELF-CHECK
A 6-week-old infant has a pansystolic murmur at the lower left sternal border with a thrill, failure to thrive, and a mid-diastolic rumble at the apex. The MOST likely diagnosis and the explanation for the mid-diastolic rumble is:
A. ASD — increased flow across the tricuspid valve
B. Large VSD — increased flow across the mitral valve (functional mitral stenosis)
C. PDA — diastolic runoff in the aorta
D. Pulmonary stenosis — turbulence across the pulmonary valve in diastole
Reveal Answer
Answer: B. Large VSD — increased flow across the mitral valve (functional mitral stenosis)
A large VSD produces a pansystolic murmur at LLSB plus a mid-diastolic rumble at the apex. The apex rumble is NOT from the VSD itself but from the large volume of blood recirculating through the pulmonary vasculature and returning to the left atrium, then crossing the mitral valve — the increased flow across a normal mitral valve creates a functional 'mitral stenosis' murmur. This is a classic pointer to a haemodynamically significant L→R shunt.
Haemodynamics: L→R Shunts and Obstructive Lesions
The haemodynamics of acyanotic congenital heart disease determine the nature of cardiac stress, the timing and pattern of symptoms, and ultimately the risk of irreversible pulmonary vascular disease. Two fundamentally different haemodynamic patterns exist: left-to-right shunting (with volume overload of the pulmonary circulation) and obstruction (with pressure overload of the relevant ventricle or great vessel). A clear grasp of these mechanisms explains why management differs so dramatically between lesion types.
Left-to-Right Shunt Haemodynamics: In all three major L→R shunt lesions, oxygenated blood from the higher-pressure left side crosses to the lower-pressure right side, adding extra volume to the pulmonary circulation. The key metric is the Qp:Qs ratio (pulmonary-to-systemic flow ratio, calculated via the Fick principle at cardiac catheterisation or estimated by echocardiography). A Qp:Qs of 1.5–2:1 is a moderate shunt; >2:1 is haemodynamically significant and usually symptomatic.
- VSD haemodynamics: In small VSDs, the high resistance of the defect limits the shunt — Qp:Qs <1.5, and many close spontaneously (especially muscular type). In large non-restrictive VSDs, equalization of ventricular pressures occurs: the right ventricle and pulmonary artery are exposed to systemic (left ventricular) pressure, leading to left heart volume overload, pulmonary oedema, and cardiac failure. The left ventricle is dilated but not hypertrophied initially — it is volume-loaded.
- ASD haemodynamics: The shunt is at atrial level; the pressure difference between atria is small (5–10 mmHg). The right ventricle tolerates the volume load well — ASD rarely causes cardiac failure in infancy. Over decades, however, chronic right ventricular volume overload leads to right ventricular dilatation, arrhythmias (atrial fibrillation), and eventually pulmonary hypertension.
- PDA haemodynamics: Blood flows from the aorta through the ductus into the pulmonary artery during both systole and diastole (because aortic pressure exceeds pulmonary artery pressure throughout the cardiac cycle — hence the continuous murmur). The diastolic run-off into the pulmonary artery produces bounding pulses and wide pulse pressure (elevated systolic, reduced diastolic). Both left atrium and left ventricle dilate due to increased pulmonary venous return.
Obstructive Lesion Haemodynamics: Pulmonary stenosis (PS) produces right ventricular pressure overload with right ventricular hypertrophy; in severe PS, right ventricular pressure may exceed systemic. Aortic stenosis (AS) produces left ventricular pressure overload with concentric left ventricular hypertrophy. Coarctation of the Aorta produces proximal (upper body) hypertension and distal hypoperfusion — the kidneys sense reduced perfusion, activating the renin-angiotensin system and perpetuating hypertension.
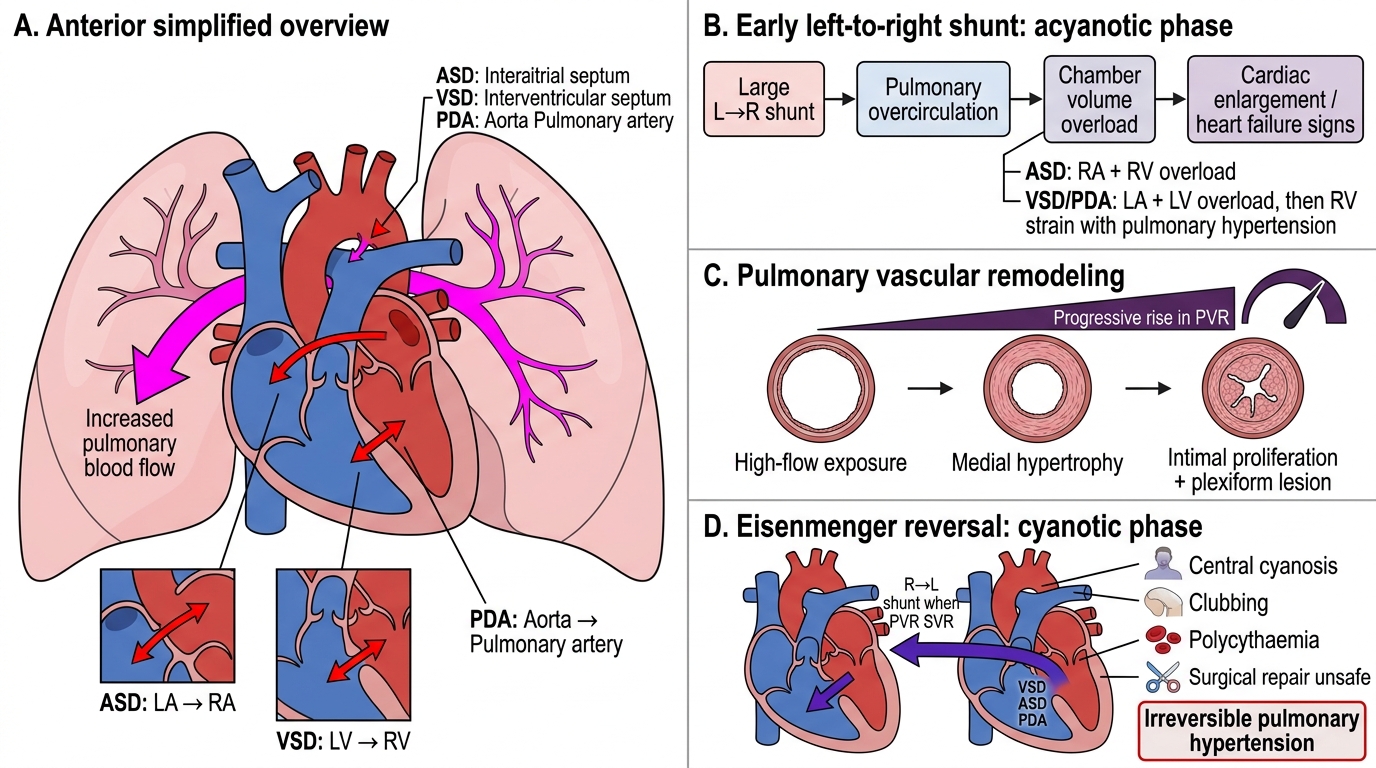
Pulmonary Vascular Resistance and its Central Role: In normal postnatal life, pulmonary vascular resistance (PVR) is low and systemic vascular resistance (SVR) is high — this drives L→R flow in shunt lesions. The magnitude of the shunt depends on the ratio PVR:SVR. As pulmonary arteries are exposed to high-pressure, high-flow blood, they respond with medial hypertrophy, intimal hyperplasia, and eventual fibrosis (Heath–Edwards grades I–VI) — a process of pulmonary arterial hypertension (PAH) that, if irreversible, converts a curable defect into an inoperable one.
Haemodynamics of Left-to-Right Shunts and Eisenmenger Reversal
Eisenmenger Syndrome — The Critical Complication
Eisenmenger syndrome represents the most feared complication of uncorrected large left-to-right shunt lesions and stands as the classic example of a curable disease rendered incurable by delayed diagnosis. Understanding its mechanism is not merely academic — recognising its early features and knowing that it renders surgical repair unsafe is a clinical imperative.
Mechanism of Eisenmenger Syndrome: In a large, uncorrected L→R shunt (most commonly a large VSD, but also large ASD or PDA), the pulmonary vasculature is chronically exposed to high-pressure, high-flow blood. Over months to years, the pulmonary arterioles undergo irreversible structural changes — medial hypertrophy, intimal proliferation, and ultimately obliterative plexiform lesions — causing a progressive rise in pulmonary vascular resistance (PVR). When PVR equals or exceeds systemic vascular resistance (SVR), the shunt first becomes bidirectional, then reverses direction to a right-to-left shunt. The child now becomes cyanotic — having been acyanotic before. This is the defining moment of Eisenmenger syndrome.
Clinical Features: The child with Eisenmenger syndrome presents with central cyanosis (clubbing, polycythaemia, exercise intolerance), haemoptysis (due to in-situ pulmonary arterial thrombosis and rupture of dilated vessels), syncope on exertion, and signs of right heart failure (raised JVP, peripheral oedema, hepatomegaly). The previously loud murmur may actually diminish or disappear as the shunt reverses and becomes less turbulent.
Differential Cyanosis in PDA-Eisenmenger: In PDA with reversed shunt, a distinctive pattern emerges — differential cyanosis: the right-to-left shunt in the PDA delivers desaturated blood into the descending aorta below the ductus. Blood above the ductus (carotid, subclavian, right upper limb) remains oxygenated. Therefore, the lower limbs are cyanosed and clubbed while the upper limbs remain pink — a pathognomonic finding of reversed PDA shunt and a must-know trap in examinations.
Why Eisenmenger is Inoperable: If surgical closure is attempted once PVR is irreversibly elevated (PVR index >8–10 Wood units/m²), the shunt is the ONLY mechanism by which the right ventricle can offload its afterload. Closing it traps the right ventricle against a catastrophically elevated PVR, causing immediate right heart failure and death. Management of established Eisenmenger syndrome is medical (pulmonary vasodilators such as bosentan, sildenafil) and eventually consideration for combined heart-lung transplantation — the condition is not curable at this stage.
The Preventable Window: VSDs presenting with cardiac failure in the first year of life, and large PDAs in neonates/infants, must be corrected before irreversible PAH develops. This is why early recognition — the scenario in our opening hook — determines outcome.
CLINICAL PEARL
Differential cyanosis is pathognomonic of reversed-PDA Eisenmenger syndrome: when you see a child with cyanosis and clubbing confined to the lower limbs (and potentially the left hand if the ductus inserts near the left subclavian) while the right hand and face remain pink, you are looking at a reversed PDA shunt. The desaturated blood from the pulmonary artery enters the descending aorta below the ductus, sparing the vessels that branch from the aortic arch above it. This is distinct from VSD-Eisenmenger where cyanosis is uniform. Recognising this pattern can save a step in diagnosis — it tells you exactly which lesion caused Eisenmenger before echocardiography confirms it. A corollary pearl: in early VSD, the second heart sound (S2) is a reliable guide to pulmonary arterial pressure — a loud, single, narrow-split S2 at the upper left sternal border signals rising PAP and is an early warning of evolving Eisenmenger.
SELF-CHECK
A 12-year-old boy has a history of a heart murmur since infancy that was not treated. He now has cyanosis and clubbing of both feet and the left hand but his right hand and face are pink. He is breathless on exertion and has haemoptysis. What is the most likely diagnosis and the mechanism?
A. Tetralogy of Fallot — right ventricular outflow obstruction
B. Eisenmenger syndrome with reversed PDA — desaturated blood enters the descending aorta below the ductus
C. Large VSD with Eisenmenger — differential cyanosis at ventricular level
D. Pulmonary atresia — no pulmonary blood flow
Reveal Answer
Answer: B. Eisenmenger syndrome with reversed PDA — desaturated blood enters the descending aorta below the ductus
The pattern of lower-limb and left-hand cyanosis with right-hand and face remaining pink is pathognomonic of Eisenmenger syndrome secondary to a reversed PDA. In reversed PDA, desaturated blood from the right ventricle/pulmonary artery flows via the ductus into the descending aorta below the level of the left subclavian artery origin. Blood to the right arm and head (from the brachiocephalic and left carotid artery, which branch above the ductus) is fully saturated. The left hand may be cyanosed if the ductus inserts close to the left subclavian artery origin. VSD-Eisenmenger causes uniform central cyanosis, not differential.