Page 2 of 31
PE22.1 | Acyanotic Heart Disease — SDL Guide (Part 2)
Diagnosis and Investigation of Acyanotic CHD
Investigation of acyanotic CHD follows a structured progression from clinical examination to non-invasive imaging, with invasive cardiac catheterisation reserved for specific indications. The three cornerstones are the electrocardiogram (ECG), chest X-ray (CXR), and 2D echocardiography with Doppler — the last of which has largely supplanted cardiac catheterisation as the gold standard for anatomical and haemodynamic diagnosis in the paediatric population.
Provided image
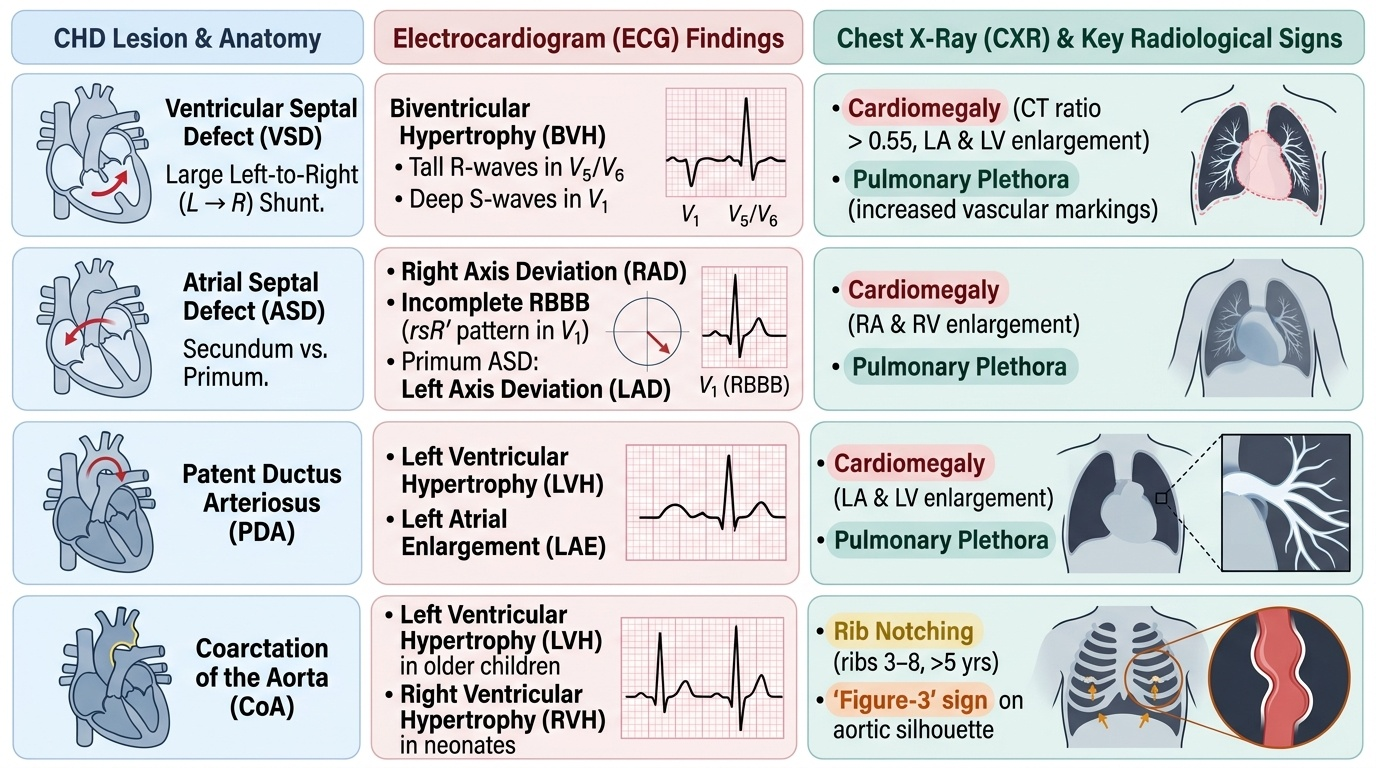
Electrocardiogram (ECG): The ECG reflects the haemodynamic stress on individual cardiac chambers. In VSD with a large L→R shunt, there is biventricular hypertrophy (tall R in V5/V6, deep S in V1 — left ventricular volume overload plus right ventricular pressure overload). A large ASD typically shows right axis deviation (RAD) and right bundle branch block (RBBB) pattern — specifically incomplete RBBB with rsR′ in V1 (a right ventricular conduction delay pattern); secundum ASD may also show RAD while primum ASD (AVSD) characteristically shows left axis deviation (LAD). In PDA, the ECG shows left ventricular hypertrophy and left atrial enlargement. Coarctation of the Aorta in older children shows left ventricular hypertrophy; in neonates, right ventricular hypertrophy may predominate.
Chest X-Ray (CXR): The CXR in L→R shunt lesions shows cardiomegaly (cardiothoracic ratio >0.55 in infants) and pulmonary plethora — increased and prominent vascular markings extending to the periphery of the lung fields. In large VSD and PDA, left atrial and left ventricular enlargement contribute to the cardiomegaly. ASD shows right ventricular and right atrial enlargement. The classic radiological sign of Coarctation of the Aorta is rib notching — erosion of the undersurface of the ribs by dilated intercostal collateral arteries (usually ribs 3–8, visible after age 5 years) — and the 'figure-3' sign or 'reverse-3' (E-sign) on barium swallow, reflecting the indentation of the aorta at the coarctation site with pre- and post-stenotic dilatation.
Echocardiography: The definitive investigation. 2D echo with colour Doppler directly visualises the defect, its location, size, and the direction and velocity of the shunt. M-mode echo measures chamber dimensions. Qp:Qs can be calculated non-invasively from Doppler measurements of pulmonary and aortic outflow velocities and areas. Echo also estimates right ventricular and pulmonary artery systolic pressure via the tricuspid regurgitation jet velocity (modified Bernoulli equation), enabling assessment of PAH severity.
Cardiac Catheterisation: Indicated primarily when non-invasive data are inadequate, when interventional closure is planned (e.g. device closure of ASD or PDA), or when precise PVR measurement is needed to assess operability (particularly to determine if Eisenmenger has supervened). Catheterisation measures oxygen saturation at each cardiac chamber level (an oxygen step-up at ventricular level confirms VSD; step-up at atrial level confirms ASD; step-up at pulmonary artery level confirms PDA) and calculates Qp:Qs via the Fick principle.
Management of Acyanotic CHD
Management of acyanotic congenital heart disease integrates three parallel goals: medical stabilisation of haemodynamic compromise in the symptomatic infant, timely referral for definitive interventional or surgical correction, and long-term follow-up to prevent the catastrophic complication of irreversible pulmonary arterial hypertension. The paediatric clinician encountering a child with acyanotic CHD carries the primary responsibility not only for initiating anti-failure therapy and preventing infective endocarditis, but for ensuring the child reaches the cardiologist and cardiac surgeon at the optimal therapeutic window — a window that opens in infancy and closes, irreversibly, once Eisenmenger physiology is established. This dual mandate — manage now, refer before it is too late — defines the clinical approach to every child with a haemodynamically significant defect.
Provided image
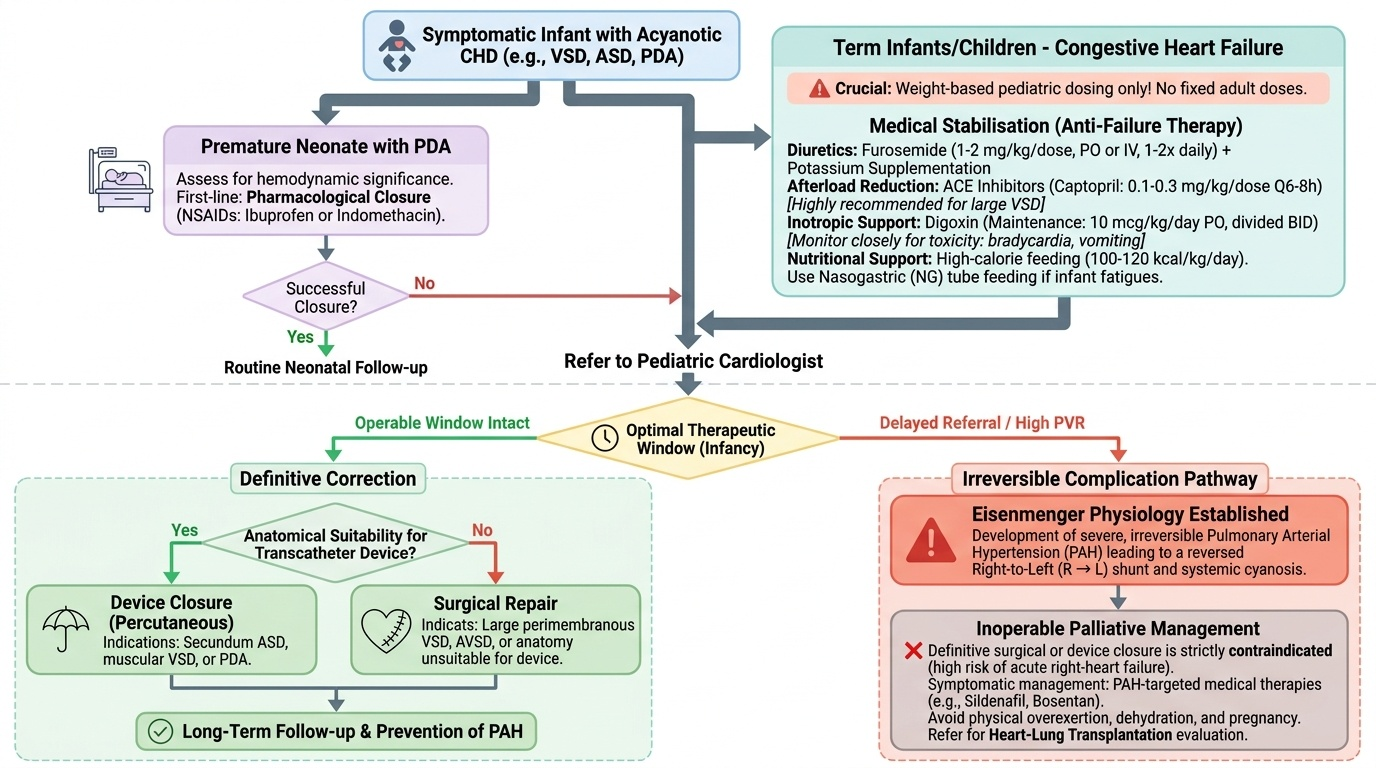
Medical Management — Anti-failure Therapy: In infants with large L→R shunts presenting with congestive cardiac failure, the immediate priority is reducing the haemodynamic burden while the child is prepared for definitive repair. Weight-based paediatric dosing is non-negotiable; adult fixed doses are dangerous and must never be used in children.
- Diuretics: Furosemide (1–2 mg/kg/dose orally or IV, 1–2 times daily) is the first-line diuretic to reduce pulmonary oedema and systemic venous congestion. Potassium supplementation is co-prescribed to prevent hypokalaemia.
- Digoxin: Used to improve myocardial contractility and as a mild diuretic adjunct. Maintenance dose: 10 mcg/kg/day orally in two divided doses in infants; dose is weight-band specific and must be verified against Ghai/Nelson tables. Narrow therapeutic index — toxicity (bradycardia, arrhythmias, vomiting) must be monitored.
- ACE inhibitors (Captopril): Reduce afterload by lowering systemic vascular resistance, thereby reducing the degree of L→R shunting. Captopril dose: 0.1–0.3 mg/kg/dose every 6–8 hours. Particularly useful in infants with large VSD.
- Caloric supplementation: High-calorie feeds (100–120 kcal/kg/day) address failure to thrive; nasogastric tube feeding may be required if the infant fatigues on oral feeding.
Medical Closure of PDA — Premature Neonates: In premature neonates with haemodynamically significant PDA (where the ductus remains open due to immaturity), pharmacological closure is first-line:
• Indomethacin: 0.1–0.2 mg/kg IV over 20–30 minutes every 12–24 hours (dose and interval vary with postnatal age and gestational age per Nelson protocol). Mechanism: COX inhibitor → reduces prostaglandin E2 → promotes ductal smooth muscle contraction. Contraindicated in renal failure, coagulopathy, necrotising enterocolitis.
• Ibuprofen: 10 mg/kg IV loading then 5 mg/kg at 24 h and 48 h — similar efficacy to indomethacin with fewer adverse renal effects; increasingly preferred.
Prostaglandin E1 (PGE1) — Duct-Dependent Lesions: In critical CoA presenting as a neonate with cardiovascular collapse as the ductus closes, PGE1 (alprostadil) 0.05–0.1 mcg/kg/min IV infusion is lifesaving — it keeps the ductus open until surgical repair. Apnoea is a dose-dependent side effect requiring monitoring.
Interventional and Surgical Management: Definitive treatment is catheter-based device closure or open cardiac surgery, guided by defect anatomy and haemodynamic significance.
- VSD: Small VSDs (Qp:Qs <1.5) with no symptoms may be observed — up to 30–40% of muscular VSDs close spontaneously by age 2 years. Large VSDs with Qp:Qs >2:1, failure to thrive, or cardiac failure require surgical closure (patch repair) ideally at 3–6 months of age. Catheter-based device closure is suitable for select muscular and perimembranous VSDs.
- ASD: Ostium secundum ASDs with haemodynamically significant shunting are closed percutaneously with the Amplatzer septal occluder (device closure, preferred if anatomy suitable) or surgically. Ideal timing is 3–5 years of age. Ostium primum (AVSD) requires surgical repair.
- PDA: In term infants and older children, surgical ligation (thoracoscopic or open) or transcatheter coil/device occlusion (Amplatzer duct occluder). In premature neonates — indomethacin/ibuprofen first; surgical ligation if pharmacological closure fails.
- Coarctation of the Aorta: Balloon dilation with or without stenting (for native CoA in older children or re-coarctation) or surgical resection with end-to-end anastomosis in neonates and infants.
Subacute Bacterial Endocarditis (SBE) Prophylaxis: Per IAP/AHA guidelines, SBE prophylaxis (amoxicillin 50 mg/kg orally, max 2 g, 30–60 min before procedure) is recommended for children with unrepaired cyanotic CHD, prosthetic valves, or previous endocarditis undergoing dental or invasive respiratory procedures. It is NOT routinely recommended for all CHD.
When NOT to Operate — Eisenmenger Syndrome: Once PVR index is irreversibly elevated (>8–10 Wood units/m²), surgical closure is contraindicated. Management includes pulmonary vasodilators (bosentan 2 mg/kg twice daily, sildenafil 0.25–1 mg/kg every 6–8 hours — weight-based), phlebotomy for symptomatic polycythaemia, avoidance of dehydration and high altitude, and eventually listing for combined heart-lung transplantation.
SELF-CHECK
A 3-month-old infant with a large VSD has been started on anti-failure treatment awaiting surgery. Which of the following treatment strategies is CORRECT?
A. Digoxin 0.5 mg daily (adult dose) + furosemide 40 mg daily
B. Furosemide 1–2 mg/kg/dose + captopril 0.1–0.3 mg/kg/dose + high-calorie feeds at 100–120 kcal/kg/day
C. Indomethacin 0.2 mg/kg IV — to close the VSD pharmacologically
D. Observation only — all VSDs close spontaneously within 3 months
Reveal Answer
Answer: B. Furosemide 1–2 mg/kg/dose + captopril 0.1–0.3 mg/kg/dose + high-calorie feeds at 100–120 kcal/kg/day
The correct approach uses weight-based paediatric dosing: furosemide for pulmonary oedema, captopril (an ACE inhibitor) to reduce systemic afterload and thereby reduce L→R shunting, and high-calorie feeds to address failure to thrive. Adult fixed doses are dangerous in infants. Indomethacin closes the ductus arteriosus (PDA) — NOT a VSD. Not all VSDs close spontaneously; large (Qp:Qs >2:1), symptomatic VSDs require surgical repair — only small muscular VSDs have a significant spontaneous closure rate.
Self-Assessment — Acyanotic Heart Disease
Use this section to consolidate your understanding of acyanotic CHD through an integrated case scenario. Review each question critically against the haemodynamic principles and clinical patterns covered in this module. If you find yourself uncertain about any answer, return to the relevant section and re-read the haemodynamic mechanism before proceeding.
Integrated Case for Self-Review: A 9-month-old boy presents with recurrent chest infections, failure to thrive (current weight 6.1 kg), and mild breathlessness. Examination reveals: pulse 130/min and bounding in character with wide pulse pressure (systolic 95, diastolic 40 mmHg); a continuous murmur heard loudest at the upper left sternal border; and a hyperactive precordium. CXR shows cardiomegaly with pulmonary plethora. ECG shows left ventricular hypertrophy and left atrial enlargement.
Key questions to consider:
1. What is the most likely diagnosis and why does this infant have wide pulse pressure and bounding pulses?
2. What haemodynamic ratio would you calculate on echocardiography or catheterisation to quantify the shunt magnitude?
3. If this child is now 8 years old and returns with central cyanosis, clubbing, and a diminished murmur, what has happened and why is he now inoperable?
4. What weight-based drug would you use if this were a premature neonate, and at what dose?
Answers (review after self-attempt):
1. The continuous machinery murmur + bounding pulses + wide pulse pressure = PDA. The diastolic run-off through the ductus into the pulmonary artery lowers the diastolic BP, widening pulse pressure. The left ventricle compensates with a hyperdynamic stroke — hence bounding pulses.
2. Qp:Qs ratio — calculated via Fick principle at catheterisation or estimated by Doppler echo. A Qp:Qs >2:1 is haemodynamically significant.
3. Eisenmenger syndrome secondary to PDA reversal — chronic high-pressure, high-flow pulmonary overcirculation has caused irreversible pulmonary arterial hypertension (PVR ≥ SVR), reversing the shunt to R→L. The murmur disappears because the turbulence of L→R flow is gone. He is inoperable because closing the ductus would eliminate the only outlet for the right ventricle against irreversibly elevated PVR.
4. Indomethacin 0.1–0.2 mg/kg IV (or ibuprofen 10 mg/kg loading then 5 mg/kg at 24 h and 48 h) — COX inhibitor to reduce PGE2 and promote ductal closure in premature neonates.