Page 4 of 31
PE22.2 | Cyanotic Heart Disease — SDL Guide
Learning Objectives
- Describe the haemodynamic changes that produce central cyanosis in congenital heart disease
- Identify and differentiate the five major cyanotic lesions (5 Ts) by anatomy, physiology, and clinical features
- Interpret chest X-ray and ECG findings characteristic of each cyanotic lesion
- Outline immediate management including PGE1 for duct-dependent lesions and tet-spell management
- Describe surgical palliation and definitive repair options for cyanotic CHD
INSTRUCTIONS
Cyanotic congenital heart disease is a paediatric emergency — a newborn in your neonatal unit, blue and tachypnoeic despite oxygen, may die within hours without recognition and prostaglandin E1. In India, CHD accounts for nearly half of all congenital anomalies and cyanotic lesions represent the most life-threatening subset. Mastering the '5 Ts', understanding duct-dependency, and knowing how to manage a tet-spell will directly save lives in your internship and postgraduate practice.
References
- Ghai Essential Pediatrics, 9th edition, Ch 14 — Diseases of Cardiovascular System (textbook)
- Nelson Textbook of Pediatrics, 21st edition, Ch 457–463 — Cyanotic Congenital Heart Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are on call in the NICU. A term newborn delivered 6 hours ago is noted to have persistent bluish discolouration of the lips and tongue despite being placed on free-flow oxygen. The saturation probe reads 72% on oxygen. Auscultation reveals a harsh systolic murmur along the left sternal border. The chest X-ray shows a boot-shaped cardiac silhouette with oligaemic lung fields. The cardiologist on call says 'start PGE1 now and call the cardiac surgery team.' What is the diagnosis? What is the risk if PGE1 is delayed? What will PGE1 do for this baby — and at what dose?
WHY THIS MATTERS
Cyanotic congenital heart disease (CCHD) represents a group of structural cardiac defects in which deoxygenated blood bypasses the lungs and enters the systemic circulation, causing persistent central cyanosis from birth or early infancy. In India, CHD has a birth prevalence of approximately 8–10 per 1,000 live births, and cyanotic lesions account for roughly 25–30% of all CHD cases. Without timely diagnosis and intervention, duct-dependent cyanotic lesions carry a mortality of over 50% in the neonatal period. As a final-year student and future intern, you will be the first to evaluate a cyanotic newborn — your ability to recognise the clinical pattern, perform the hyperoxia test, interpret the chest X-ray, and initiate PGE1 while arranging transfer may be the difference between survival and death.
RECALL
Before proceeding, recall these foundational concepts from your earlier studies:
- Fetal circulation (PY): in utero, oxygenated blood from the placenta enters via the umbilical vein → ductus venosus → IVC → right heart → foramen ovale (to left heart) and ductus arteriosus (bypassing lungs). At birth, the ductus arteriosus closes over 24–48 hours under the influence of oxygen and prostaglandin withdrawal.
- Cardiac embryology (AN): the conotruncal septum divides the primitive truncus into aorta and pulmonary artery; failure produces truncus arteriosus or TGA. The interatrial septum (foramen ovale) and interventricular septum close during gestation; defects produce ASD and VSD.
- Acyanotic CHD (from PE16 — Cardiovascular System basics): ASD, VSD, and PDA cause left-to-right shunts, producing pulmonary plethora but NOT early cyanosis; cyanotic CHD involves right-to-left shunts, producing systemic hypoxaemia.
- Oxygen haemoglobin dissociation curve: clinically apparent cyanosis requires reduced haemoglobin ≥3–5 g/dL in capillaries — more difficult to detect in anaemic children.
Clinical Presentation of Cyanotic Heart Disease
The cardinal symptom of cyanotic heart disease is central cyanosis — blue discolouration of the lips, tongue, mucous membranes, and nail beds reflecting reduced haemoglobin ≥3–5 g/dL in the capillaries. Unlike peripheral cyanosis (acrocyanosis seen transiently in cold exposure or in the first hours of life), central cyanosis persists in a warm environment and does not improve significantly with supplemental oxygen alone — this fundamental difference is the basis of the hyperoxia test that you will use to discriminate cardiac from respiratory causes. Cyanosis is typically present from birth in severe lesions such as TGA, critical TOF, and obstructed TAPVC, but may develop gradually over weeks to months in milder or non-obstructed forms. The timing, severity, and associated features together allow the experienced clinician to narrow the likely lesion before echocardiography confirms the anatomy. Recognition of the presenting pattern — and the appropriate first response — is the most immediate clinical skill this module develops.
The clinical features vary by lesion severity and the child's age:
- Neonatal presentation (duct-dependent lesions): profound cyanosis at or within hours of birth; tachypnoea without significant recession; no response to oxygen; duct-dependent mixing is the only source of pulmonary or systemic flow.
- Infancy presentation: central cyanosis, failure to thrive (increased metabolic demand, poor feeding, decreased caloric intake), tachypnoea on exertion or feeding, and recurrent respiratory infections from increased pulmonary blood flow in some lesions (TAPVC).
- Childhood presentation (TOF): digital clubbing (after 6 months of persistent hypoxaemia — proliferating connective tissue under nail folds due to circulating megakaryocytes and PDGF), squatting posture (increases systemic vascular resistance, reduces right-to-left shunt acutely, improves saturation), and hypercyanotic (tet) spells.
Tet-spell / hypercyanotic spell is an acute, life-threatening episode seen in TOF where sudden fall in systemic vascular resistance or increase in RVOTO triggers a catastrophic increase in right-to-left shunt. The child becomes deeply cyanotic, agitated, hyperventilating, and may lose consciousness or convulse. These typically occur in the morning after waking, during crying, feeding, or defecation. Squatting is the child's own compensatory mechanism. Age of onset of tet-spells is a key indicator for surgical timing.
- Murmur: lesion-specific (see investigations); notably, the murmur in TOF is from RVOTO (not from the VSD itself), and in TGA there may be no murmur if no associated VSD exists.
On examination: central cyanosis, clubbing in older infants, parasternal heave (RV hypertrophy), variable murmur, hepatomegaly (in right heart failure as seen in TAPVC).
Right-to-Left Shunt Pathophysiology
Haemodynamic Changes and Pathophysiology
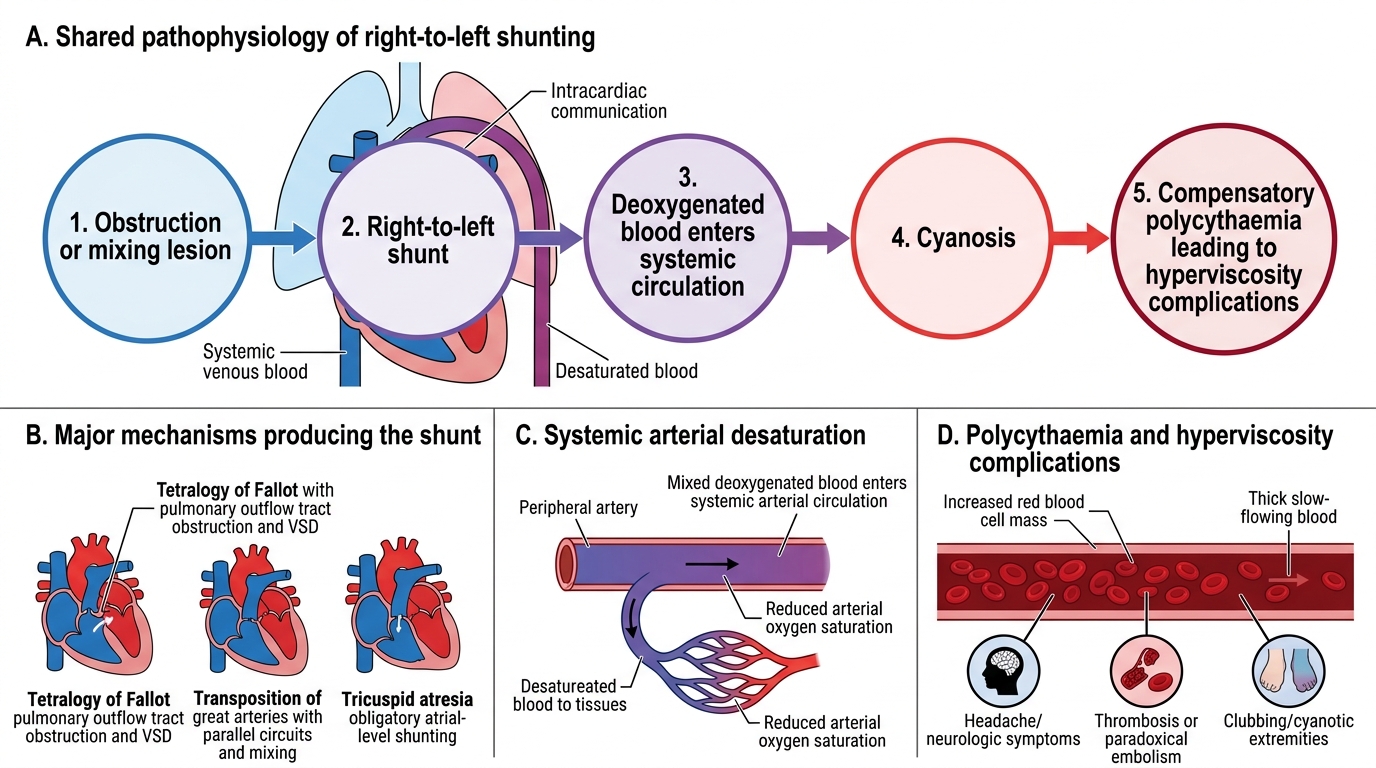
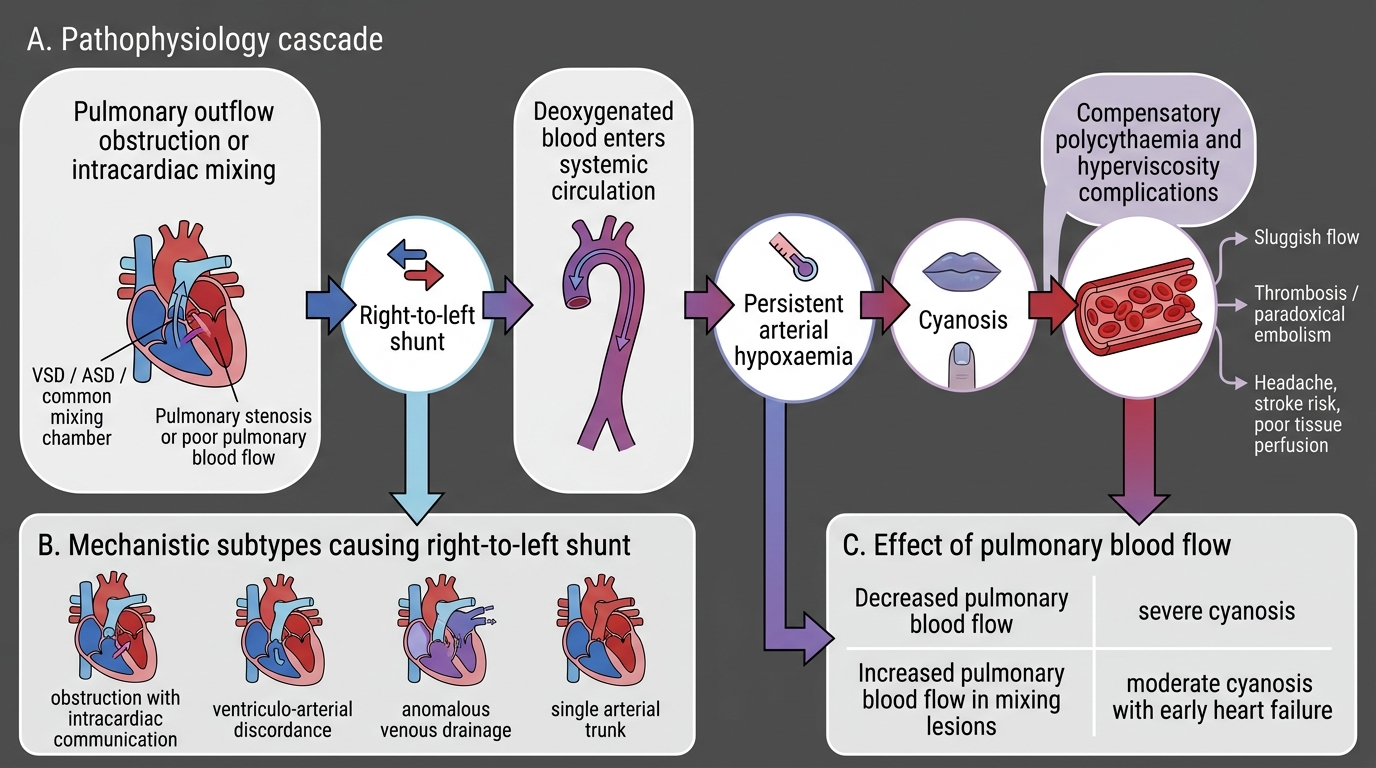
The common haemodynamic thread in all cyanotic CHD is right-to-left shunting — deoxygenated systemic venous blood bypasses the pulmonary circulation and enters the systemic arterial circulation, producing persistent arterial desaturation. Understanding this physiology at a mechanistic level is essential because the treatment strategy — whether PGE1, balloon septostomy, or a palliative shunt — is chosen directly from the haemodynamic subtype. The mechanism of shunting differs between the four main lesion groups (obstruction with intracardiac communication; ventriculo-arterial discordance; anomalous venous drainage; single arterial trunk), but once right-to-left shunting is established the downstream systemic consequences — arterial hypoxaemia, compensatory polycythaemia, hyperviscosity, and the risk of paradoxical embolism — are shared across the group. The relationship between pulmonary blood flow and clinical severity is equally important: decreased pulmonary flow causes profound cyanosis, while some mixing lesions with increased pulmonary flow paradoxically produce only moderate cyanosis but early heart failure.
Mechanisms of right-to-left shunting:
- Obstruction + intracardiac communication (TOF, tricuspid atresia): obstruction to pulmonary flow (infundibular stenosis in TOF; absent tricuspid valve in tricuspid atresia) raises right-sided pressures; blood preferentially crosses a septal defect (VSD in TOF; obligate ASD in tricuspid atresia) into the left heart or aorta without being oxygenated.
- Ventriculo-arterial discordance (TGA): the aorta arises from the RV and the pulmonary artery from the LV, creating two parallel circuits — deoxygenated blood recirculates through the body while oxygenated blood recirculates through the lungs. Survival requires obligate mixing via ASD, VSD, or PDA.
- Anomalous venous drainage (TAPVC): all four pulmonary veins drain into the right heart or systemic veins instead of the left atrium; oxygenated pulmonary venous blood mixes with systemic venous return and enters the right side → obligate right-to-left shunt at atrial level via ASD to maintain any systemic output.
- Single arterial trunk (Truncus arteriosus): a single great vessel overrides the VSD, receiving output from both ventricles; mixing at the level of the truncus is obligatory.
Downstream haemodynamic consequences:
- Arterial hypoxaemia → stimulates erythropoietin release → compensatory polycythaemia (haematocrit may exceed 65–70%) → hyperviscosity → sludging in small vessels → cerebrovascular events (paradoxical embolism from right-to-left shunt) and brain abscess (paradoxical septic emboli — venous micro-emboli bypass pulmonary clearance and lodge in the brain; most common in children >2 years with TOF).
- Pulmonary blood flow effects: decreased (TOF, tricuspid atresia → oligaemic lung fields on CXR) or increased (TAPVC, TGA with VSD → plethoric fields) depending on the lesion.
- Duct-dependency: in severe lesions (critical pulmonary stenosis, TAPVC with obstruction, TGA without ASD), the patent ductus arteriosus may be the sole source of pulmonary or systemic blood flow. As the ductus closes after birth, the neonate deteriorates catastrophically. PGE1 (alprostadil) keeps the ductus open at 0.05–0.1 mcg/kg/min IV, buying time until surgery.
Pathophysiology of Right-to-Left Shunting
The Five Major Cyanotic Lesions (5 Ts)
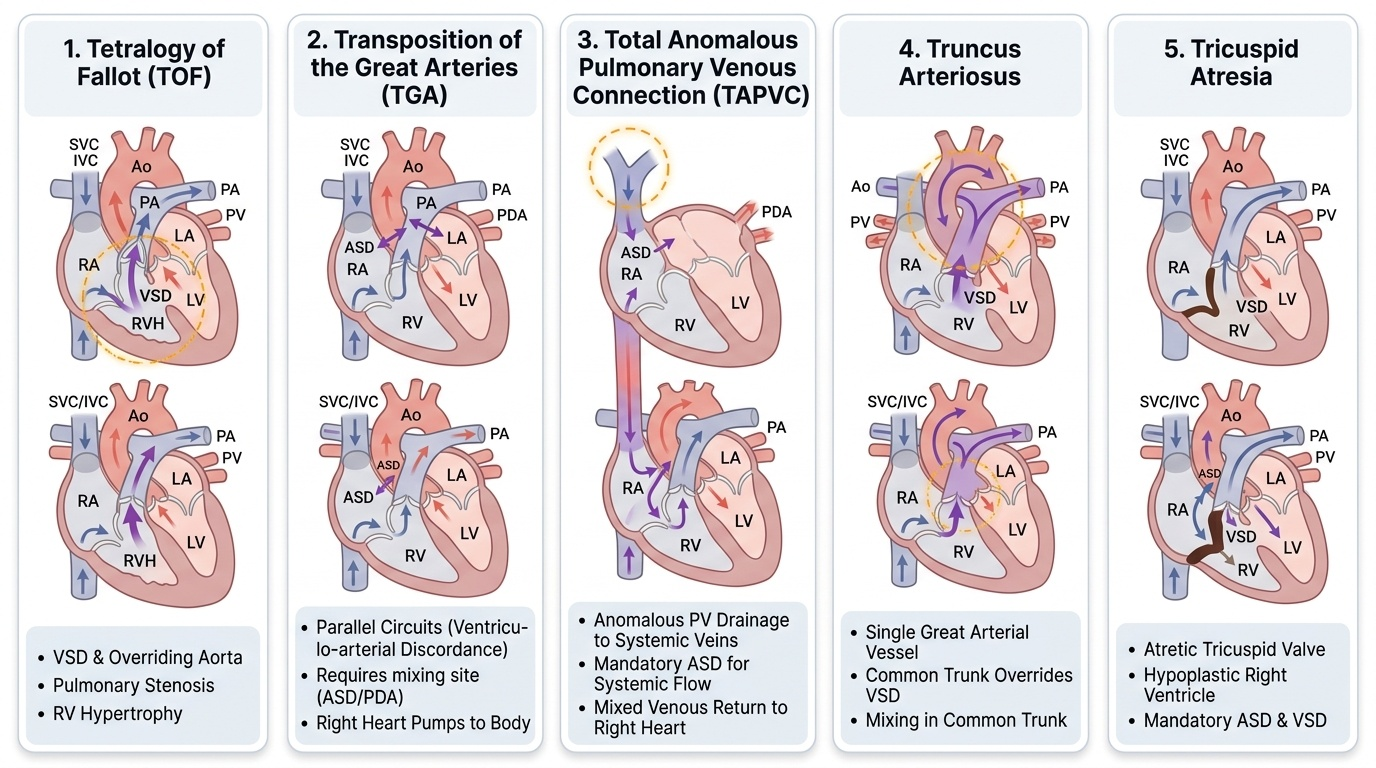
The mnemonic '5 Ts' covers the five most clinically important cyanotic congenital heart lesions. Each has a distinct anatomy, haemodynamic fingerprint, and X-ray appearance that the examiner expects you to know.
Provided image
1. Tetralogy of Fallot (TOF) — the most common cyanotic CHD (5–10% of all CHD). The four anatomical components are: (a) large VSD (malalignment type); (b) right ventricular outflow tract obstruction (RVOTO) — predominantly infundibular (subpulmonic), with or without valvular pulmonary stenosis; (c) overriding aorta (aortic root sits astride the VSD, receiving blood from both ventricles); (d) right ventricular hypertrophy (consequence of pressure overload from RVOTO). The degree of RVOTO determines clinical severity — severe obstruction causes profound cyanosis; mild obstruction produces a 'pink TOF'. CXR: boot-shaped heart (coeur en sabot) with upturned apex (RVH) and oligaemic lung fields. ECG: right axis deviation (RAD), RVH. Tet-spells (hypercyanotic episodes) are managed with knee-chest position → morphine 0.1 mg/kg IV/SC → IV fluid bolus → IV propranolol 0.1 mg/kg → phenylephrine if refractory.
2. Transposition of the Great Arteries (TGA) — aorta arises from the morphological RV; pulmonary artery from morphological LV (ventriculo-arterial discordance with concordant atrio-ventricular connections in D-TGA). The two circuits run in parallel. Survival requires mixing — via ASD, VSD, or PDA. Present in neonates with severe cyanosis unresponsive to oxygen. CXR: egg-on-side (egg-on-a-string) appearance — narrow mediastinum because the great vessels are parallel (not crossing) + cardiomegaly + pulmonary plethora. ECG: RAD, RVH. Emergency: Rashkind balloon atrial septostomy (enlarges interatrial communication). Definitive repair: arterial switch operation (Jatene procedure) in the first 2 weeks of life.
3. Total Anomalous Pulmonary Venous Connection (TAPVC) — all four pulmonary veins drain anomalously to the right heart or systemic venous system instead of the left atrium. Classified by drainage site: supracardiac (into SVC or innominate vein), cardiac (into coronary sinus or RA), infracardiac (into portal/hepatic veins — most severe, obstructed), mixed. Infracardiac TAPVC is associated with pulmonary venous obstruction → presents with cyanosis + pulmonary oedema in the first days of life. An obligate ASD provides the only systemic output. CXR: supracardiac TAPVC shows figure-of-8 (snowman sign) — dilated vertical vein + SVC form the upper bulge, enlarged right heart forms the lower bulge. Infracardiac: diffuse pulmonary oedema. Surgical repair is urgent/emergency in obstructed TAPVC.
4. Truncus Arteriosus — a single arterial trunk (truncus) overrides a large VSD and gives rise to aorta, pulmonary arteries, and coronary arteries. Obligatory complete mixing at truncal level → moderate cyanosis. CXR: cardiomegaly, plethoric lung fields, right-sided aortic arch in 30–35%. ECG: biventricular hypertrophy. Associated with DiGeorge syndrome (22q11 deletion — hypocalcaemia, T-cell immunodeficiency, conotruncal anomaly: test calcium in any neonate with truncus). Surgical repair: unifocalisation and truncal valve repair in neonatal period.
5. Tricuspid Atresia — complete absence of the tricuspid valve; the right atrium cannot empty directly into the RV. Obligate right-to-left shunt at atrial level via ASD (or patent foramen ovale). Hypoplastic RV. Pulmonary blood flow depends on associated VSD and pulmonary stenosis — variable cyanosis. CXR: cardiomegaly, left-sided cardiac apex (left ventricular dominance), oligaemic or normal lung fields. ECG: left axis deviation (LAD) — hallmark in a cyanotic child (contrast with TOF which has RAD); left ventricular hypertrophy. Management: palliative shunts (BT shunt, Glenn, Fontan procedure) — staged single-ventricle palliation.
Summary comparison:
| Lesion | Key defect | CXR | ECG | Definitive repair |
|---|---|---|---|---|
| TOF | VSD + RVOTO + overriding Ao + RVH | Boot-shaped, oligaemic | RAD, RVH | Total correction ~6 mo |
| TGA | Ventriculo-arterial discordance | Egg-on-side, plethoric | RAD, RVH | Arterial switch <2 wk |
| TAPVC | PV → right heart | Figure-of-8 or oedema | RVH | Urgent repair |
| Truncus | Single trunk + VSD | Plethoric, RA arch | BVH | Neonatal repair |
| Tricuspid atresia | No tricuspid valve | LAX apex, variable | LAD, LVH | Staged Fontan |
SELF-CHECK
A 6-hour-old neonate is deeply cyanosed. CXR shows a narrow superior mediastinum and increased pulmonary vascular markings with an 'egg-on-side' cardiac silhouette. The SpO2 is 55% on 100% oxygen. What is the most likely diagnosis?
A. Tetralogy of Fallot
B. Transposition of the Great Arteries
C. Total Anomalous Pulmonary Venous Connection
D. Tricuspid Atresia
Reveal Answer
Answer: B. Transposition of the Great Arteries
The 'egg-on-side' CXR appearance (narrow mediastinum due to parallel great vessels + cardiomegaly + pulmonary plethora) combined with profound cyanosis unresponsive to oxygen in a neonate is the classic presentation of D-TGA. TOF shows a boot-shaped heart with oligaemia. TAPVC shows a figure-of-8 (supracardiac) or pulmonary oedema pattern. Tricuspid atresia shows left axis deviation on ECG and a left-sided cardiac apex on CXR.