Page 32 of 42
PE23.16 | Portal Hypertension — SDL Guide
Learning Objectives
- Define portal hypertension and state its haemodynamic threshold
- Classify portal hypertension as pre-hepatic, intrahepatic, or post-hepatic and enumerate the causes in each category relevant to Indian children
- Explain the pathophysiology of variceal formation and the consequences of elevated portal pressure
- Distinguish EHPVO from cirrhotic portal hypertension on clinical and investigation grounds
- Describe the emergency management of acute variceal haemorrhage
- Describe secondary prophylaxis and chronic management of portal hypertension including the Rex shunt
INSTRUCTIONS
Portal hypertension is one of the most dramatic presentations in paediatric gastroenterology — a child who vomits blood from oesophageal varices needs immediate, organised emergency care. Extrahepatic portal vein obstruction (EHPVO) — not cirrhosis — is the commonest cause of portal hypertension in Indian children, a fact that distinguishes our population from Western series and has important management implications: these children have normal liver function and can survive into adulthood with appropriate variceal surveillance and management. This module covers both the emergency management of acute variceal bleeding and the chronic management strategy, integrating the pathophysiology you need to understand why each intervention works.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 18 — Portal Hypertension (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 384 — Portal Hypertension and Varices (textbook)
- NASPGHAN guidelines on portal hypertension in children (2012) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 7-year-old boy from a rural village is brought to the emergency department with sudden onset of vomiting large amounts of bright red blood. His parents say he has had a 'big spleen' for 2 years, noticed incidentally on examination. He has no history of jaundice, no family history of liver disease, and his general health has been normal otherwise. On examination: he is pale, tachycardic, BP 86/50 mmHg, massive splenomegaly, no jaundice, no ascites. His LFTs are completely normal. What is happening, and what are your next steps?
WHY THIS MATTERS
Portal hypertension in children is important for three reasons. First, it is common — in India, EHPVO alone accounts for a substantial proportion of paediatric upper GI bleeding, and most of these children are in good general health with normal livers, making early recognition and management highly effective. Second, variceal haemorrhage is life-threatening — a child can lose more than a third of circulating blood volume in minutes from a ruptured oesophageal varix, and the correct emergency response (resuscitation + pharmacological portal pressure reduction + emergency endoscopy) is time-critical. Third, long-term management of EHPVO has evolved — the meso-Rex bypass (Rex shunt) can restore physiological portal flow in selected children, offering a superior alternative to repeated endoscopic treatment.
RECALL
Before proceeding, activate your prior knowledge:
- Portal venous anatomy (from AN): the portal vein is formed by the union of the superior mesenteric vein and splenic vein at the porta hepatis; it drains the entire gut, spleen, and pancreas into the hepatic sinusoids; there is no valve in the portal system.
- Portosystemic anastomoses (from AN): sites where portal and systemic venous systems communicate — oesophagogastric junction (varices here → haematemesis), paraumbilical veins (caput medusae), anorectal junction (haemorrhoids), retroperitoneal veins. These are normally collapsed but enlarge when portal pressure rises.
- Splenomegaly and hypersplenism (from PY): the spleen sequesters blood cells when enlarged → anaemia + thrombocytopenia + leucopenia = hypersplenism.
- CLD causes of intrahepatic PHT (from previous SDL pe16-chronic-liver-disease): cirrhosis from biliary atresia, Wilson, AIH, chronic HBV — these are the intrahepatic causes.
Clinical Presentation of Portal Hypertension
Portal hypertension (PHT) presents through the consequences of elevated pressure in the portal venous system — the two principal effects being (1) the development of portosystemic collateral vessels (varices) that carry portal blood directly into the systemic circulation, bypassing the liver, and (2) splenomegaly from splenic venous engorgement with resultant splenic sequestration of blood cells (hypersplenism). The clinical presentation varies depending on whether the aetiology is pre-hepatic (such as EHPVO, where liver function is preserved) or intrahepatic (cirrhotic PHT, where signs of CLD coexist with PHT). This distinction is clinically critical because it shapes the entire investigation and management plan — a child with EHPVO has a near-normal life expectancy with appropriate variceal management, while a child with cirrhotic PHT needs management of both the PHT and the underlying progressive liver disease.
Cardinal features of portal hypertension:
• Splenomegaly — the most consistent finding; the spleen can be massively enlarged (reaching the right iliac fossa in severe cases), firm, smooth, and non-tender. The enlarged spleen causes hypersplenism: thrombocytopenia (platelet sequestration → bleeding risk), anaemia, and leucopenia.
• Variceal haemorrhage — haematemesis (bright red blood or coffee-ground material) and/or malaena (black tarry stools) from ruptured oesophageal or gastric varices. This is often the presenting event in EHPVO — the child may be entirely well before the first bleed.
• Ascites — peritoneal fluid accumulation; more prominent in cirrhotic PHT (combined effect of low oncotic pressure from hypoalbuminaemia + portal hypertension + sodium retention) than in EHPVO (where the liver makes normal albumin)
• Caput medusae — dilated periumbilical superficial veins (recanalized paraumbilical veins draining portal blood into epigastric systemic veins)
• Haemorrhoids — anorectal variceal engorgement; less common in children than adults
• Splenorenal shunts — spontaneous portosystemic collaterals may develop
Distinguishing EHPVO from cirrhotic PHT (key clinical clue):
| Feature | EHPVO | Cirrhotic PHT |
|---|---|---|
| Liver function | Normal | Abnormal (elevated bilirubin, low albumin, coagulopathy) |
| Jaundice | Absent | Present |
| Spider angiomata / palmar erythema | Absent | Present |
| Ascites | Mild or absent | Prominent |
| Liver size | Normal or small | Enlarged (early) then shrunken (late), firm/nodular |
| Growth | Normal | Impaired |
| History | Prior neonatal umbilical catheterisation / omphalitis | History of CLD cause |
In India, a child with massive splenomegaly, variceal bleeding, and normal LFTs almost certainly has EHPVO until proven otherwise.
Classification and Aetiology
The classification of portal hypertension by anatomical site of obstruction is clinically important because it predicts both the clinical features (whether liver function is affected) and the management options available. The three-level classification — pre-hepatic, intrahepatic, and post-hepatic — is the standard framework, and within each category the causes differ markedly between children and adults. In children presenting to Indian hospitals, pre-hepatic obstruction (EHPVO) far outnumbers intrahepatic cirrhotic causes as the most frequent aetiology, reversing the adult pattern. Recognising the site of obstruction from the clinical picture directs the most appropriate investigations (Doppler USG to assess portal vein patency vs liver biopsy for cirrhosis vs hepatic vein imaging for Budd-Chiari) and determines whether the liver itself is at risk, which fundamentally changes the prognostic outlook and urgency of liver-directed therapy.
Pre-hepatic portal hypertension (obstruction before the liver sinusoids):
• EHPVO (Extrahepatic Portal Vein Obstruction) — the portal vein is occluded, most commonly by thrombosis in the neonatal period (neonatal omphalitis, umbilical vein catheterisation, dehydration, septicaemia, hypercoagulable states). The occluded portal vein is replaced over months to years by a sponge-like network of collateral vessels = cavernous transformation of the portal vein (visible on Doppler USG). This is the COMMONEST cause of portal hypertension in Indian children. Liver function is entirely normal because hepatic sinusoidal pressure is not elevated — the block is proximal. Prognosis is generally good with variceal management.
• Splenic vein thrombosis — isolated splenomegaly + gastric varices (left-sided/sinistral PHT) without hepatic involvement; can follow pancreatitis.
Intrahepatic portal hypertension (obstruction within the liver):
• Cirrhotic (sinusoidal): Any cause of CLD causing cirrhosis — biliary atresia, Wilson disease, autoimmune hepatitis, chronic HBV/HCV, NAFLD. The fibrotic architecture compresses sinusoids and hepatic veins, raising intrahepatic resistance. LFTs are deranged.
• Pre-sinusoidal (non-cirrhotic): Congenital hepatic fibrosis (ductal plate malformation; associated with polycystic kidney disease — portal tracts are fibrotic but hepatocytes and LFTs are largely normal until late); schistosomiasis (periportal fibrosis — rare in India but important globally).
Post-hepatic portal hypertension (obstruction at or beyond hepatic veins):
• Budd-Chiari syndrome — obstruction of the hepatic veins or inferior vena cava (IVC); causes: hypercoagulable states (Factor V Leiden, PNH, myeloproliferative disorders), membranous IVC obstruction. Presents with painful hepatomegaly, ascites, and liver failure — USG shows absent hepatic vein flow and dilated, tortuous hepatic veins with caval obstruction.
• Right heart failure / constrictive pericarditis — elevated right atrial pressure transmitted to hepatic veins → congestion.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
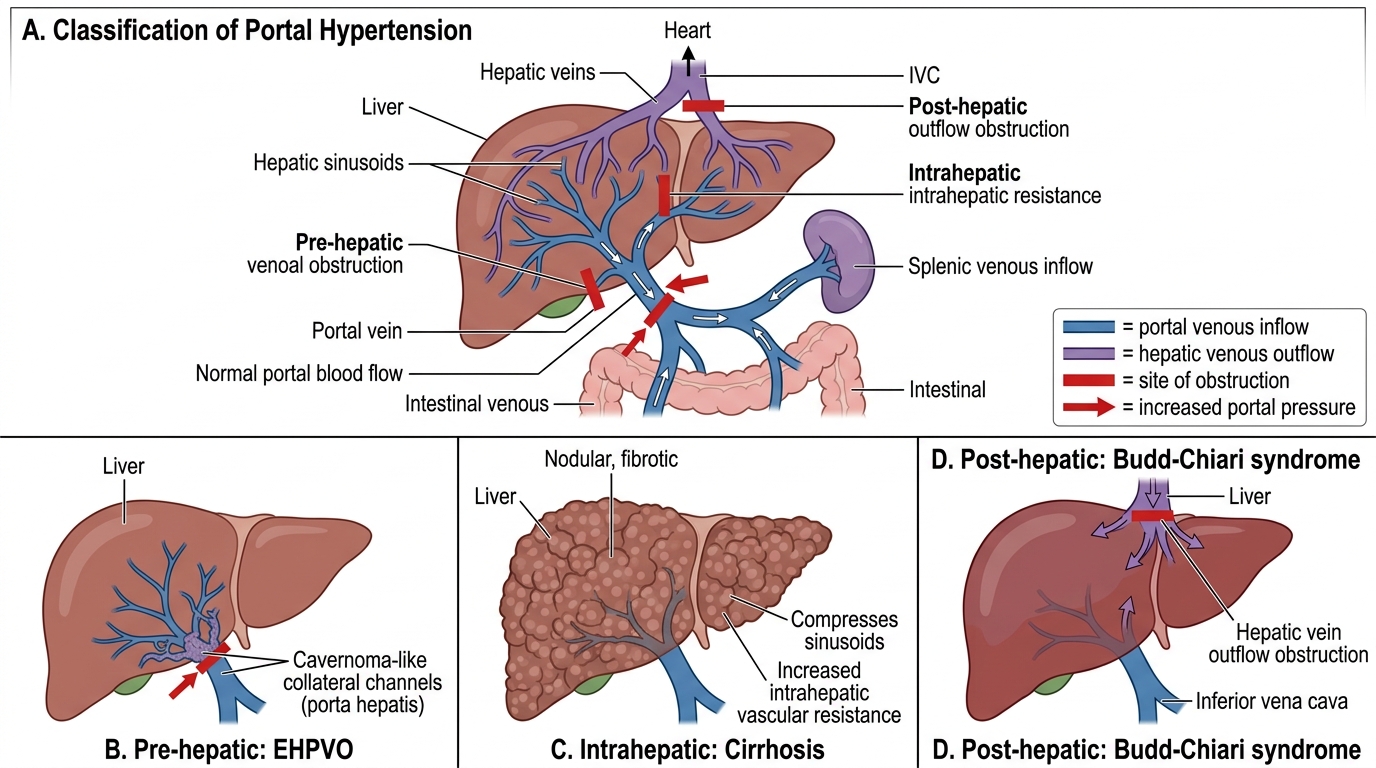
Classification of Portal Hypertension in Children
Pathophysiology of Portal Hypertension and Variceal Formation
The pathophysiology of portal hypertension is driven by two haemodynamic factors that reinforce each other: increased resistance to portal blood flow (the primary event, whether from portal vein thrombosis in EHPVO or sinusoidal fibrosis in cirrhosis) and a compensatory increase in portal blood flow mediated by splanchnic vasodilatation (secondary, driven by nitric oxide and other vasodilators released by the portal hypertensive gut). Together they sustain and progressively amplify the elevated portal pressure, explaining why portal hypertension tends to worsen over time even without new hepatic injury. This dual mechanism is also therapeutically exploitable: drugs like propranolol reduce both cardiac output (reducing portal blood flow) and cause splanchnic vasoconstriction, attacking both components simultaneously. The normal portal venous pressure is 5–10 mmHg; values above 10 mmHg define PHT, and values above 12 mmHg (as measured by hepatic venous pressure gradient, HVPG) are associated with clinically significant complications including variceal haemorrhage and ascites formation.
The variceal formation cascade:
1. Elevated portal pressure → blood seeks alternative routes from the high-pressure portal system to the low-pressure systemic venous system through pre-existing embryonic anastomotic channels
2. Portosystemic collaterals open and dilate at four anatomical sites: oesophagogastric junction (oesophageal/gastric varices), paraumbilical veins (caput medusae), retroperitoneal veins (splenorenal), anorectal veins (haemorrhoids)
3. Oesophageal varices enlarge with increasing portal pressure — their walls are thin (sub-epithelial, covered only by oesophageal squamous mucosa) and they are subject to the transmural pressure of intraluminal contents and wall tension → rupture when the variceal wall tension exceeds its tensile strength
4. Variceal bleeding is often precipitated by sudden rises in portal pressure (e.g. Valsalva manoeuvre, straining at stool, vomiting, exercise) or by erosion of the variceal wall by acidic gastric contents if gastro-oesophageal reflux is present
Splenic consequences:
• Splenic venous engorgement → congestive splenomegaly → increased splenic volume → sequestration of red cells, platelets, and white cells → hypersplenism (pancytopenia despite normal marrow)
Ascites formation in cirrhotic PHT (not in EHPVO):
• Sinusoidal hypertension → transudation of protein-poor fluid into the peritoneum; hypoalbuminaemia reduces oncotic pressure; renal sodium retention (RAAS activation) → sodium and water accumulation in the peritoneal cavity
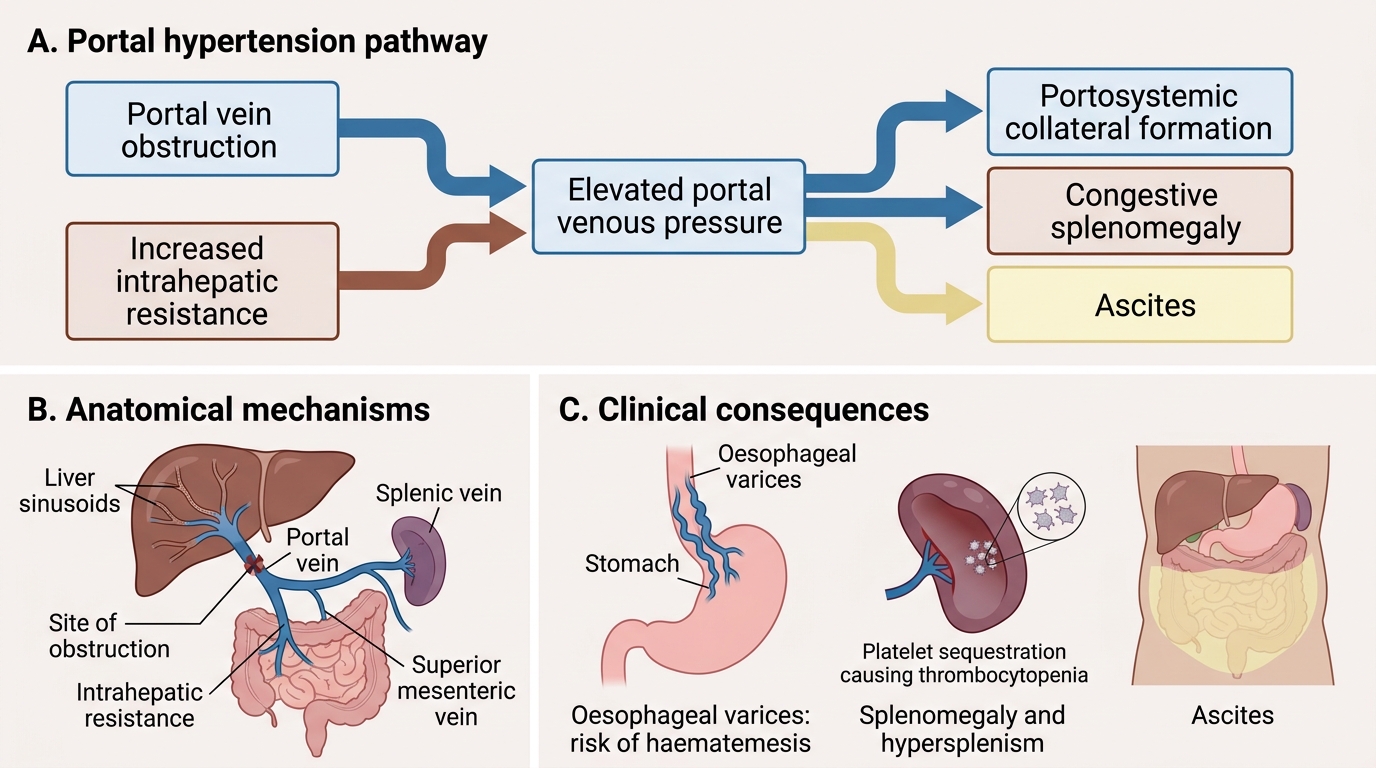
Pathophysiology of Portal Hypertension
SELF-CHECK
A 5-year-old with EHPVO has massive splenomegaly and haematemesis. His platelet count is 62,000/µL. Which mechanism is responsible for his thrombocytopenia?
A. Bone marrow suppression from chronic liver disease
B. Splenic sequestration of platelets due to congestive splenomegaly (hypersplenism)
C. Disseminated intravascular coagulation from the acute bleed
D. Impaired thrombopoietin production by the damaged liver
Reveal Answer
Answer: B. Splenic sequestration of platelets due to congestive splenomegaly (hypersplenism)
In EHPVO, the liver is normal and liver function (including thrombopoietin production) is preserved. The thrombocytopenia is from hypersplenism — the enlarged, congested spleen sequesters and destroys platelets. This is 'destructive' thrombocytopenia with a normal marrow, not marrow suppression or DIC. In EHPVO (unlike cirrhotic PHT), there is no impaired thrombopoietin synthesis since hepatocytes are intact. The clinical distinction matters: EHPVO thrombocytopenia is managed by variceal control and possibly splenectomy/Rex shunt, not by treating the liver.