Page 33 of 42
PE23.16 | Portal Hypertension — SDL Guide (Part 2)
Diagnosis and Investigation
The diagnostic approach to portal hypertension in children must answer three questions in sequence: (1) Is there portal hypertension? (clinical + USG evidence); (2) What is the site and cause (pre-hepatic/intrahepatic/post-hepatic, EHPVO vs cirrhosis vs Budd-Chiari)?; and (3) What are the complications and their severity (varices on endoscopy, degree of fibrosis, haematological consequences of hypersplenism)? The investigation strategy is guided by the clinical presentation — a child with massive splenomegaly and normal LFTs needs Doppler USG as the first investigation to look for cavernous transformation of the portal vein (EHPVO), while a child with splenomegaly, ascites, and deranged LFTs needs a full CLD workup (as detailed in the previous SDL on chronic liver disease). Endoscopy is essential in any child with confirmed PHT to assess variceal size and risk, even in the asymptomatic state, because the first variceal bleed can be catastrophic.
Key investigations:
- Doppler ultrasonography of the abdomen — the most important non-invasive investigation:
- EHPVO: portal vein not visualised as a single vessel; replaced by a tangle of collaterals at the hepatic hilum = cavernous transformation of portal vein (pathognomonic); hepatic veins and IVC patent; liver parenchyma and echotexture normal
- Cirrhotic PHT: portal vein visible but slow/reversed flow; coarse echotexture; irregular liver surface; ascites
- Budd-Chiari: hepatic veins absent or thrombosed; IVC narrowed or thrombosed; Doppler shows absent or reversed hepatic vein flow
- Upper gastrointestinal endoscopy (OGD) — essential for all patients with confirmed PHT:
- Grades oesophageal varices (Grades I–IV by size and appearance)
- Identifies portal hypertensive gastropathy (PHG — mosaic pattern in stomach mucosa)
- Detects gastric varices (cardia, fundus — higher risk of catastrophic bleed)
- Guides prophylactic or therapeutic band ligation
- Liver function tests (LFTs) — to distinguish EHPVO (normal) from cirrhotic PHT (elevated bilirubin, low albumin, elevated ALT/AST, deranged INR)
- CBC with differential — thrombocytopenia + anaemia ± leucopenia = hypersplenism; degree of thrombocytopenia reflects splenomegaly severity
- Coagulation profile — PT/INR (prolonged in cirrhotic PHT, normal in EHPVO)
- MRI/MRA portal venography — superior to USG for mapping the extent of EHPVO, identifying a patent intrahepatic left portal vein (essential for Rex shunt planning)
- Liver biopsy — if intrahepatic CLD is suspected as the cause of PHT; not needed in EHPVO where liver is normal
CLINICAL PEARL
Cavernous transformation of the portal vein — the ultrasound pathognomonic sign of EHPVO: Instead of a single, clear-walled portal vein at the hepatic hilum, Doppler USG shows a tangle of small tortuous collateral vessels — the 'cavernoma' — with hepatopetal (towards liver) flow. This finding is pathognomonic of EHPVO. The liver parenchyma is normal in echogenicity because the hepatocytes are healthy. Contrast this with cirrhotic PHT where the portal vein is visible but with slow or hepatofugal (away from liver) flow, the liver is coarse and nodular, and ascites is present. Recognising these two patterns on the USG report is a fundamental clinical skill — it immediately changes the management approach.
Management: Acute Variceal Bleed
Acute variceal haemorrhage is a paediatric emergency with mortality of 5–20% per episode if not managed correctly. The management is a structured, simultaneous sequence of resuscitation, pharmacological portal pressure reduction, antibiotic prophylaxis, and definitive endoscopic haemostasis — all running in parallel, not sequentially. Every step must be initiated without delay; waiting for investigations or specialist review before starting resuscitation measurably increases mortality. The key principle is: control the bleeding first (pharmacological + endoscopic), establish the diagnosis confirmatorily at the same endoscopy, and prevent re-bleeding with secondary prophylaxis once the acute episode is controlled. Variceal haemorrhage in EHPVO generally carries a better per-episode prognosis than in cirrhotic PHT, because the liver is entirely normal in EHPVO and there is no concurrent hepatic synthetic failure, spontaneous bacterial peritonitis, or hepatic encephalopathy; nonetheless, the acute bleed itself is equally life-threatening from haemorrhagic shock regardless of the underlying PHT aetiology.
Step 1: Resuscitation
• Establish large-bore IV access (two peripheral lines or intraosseous if necessary)
• Restore circulating volume: Ringer's lactate or 0.9% NaCl 10–20 mL/kg bolus; then packed red blood cells (10 mL/kg) to maintain haemoglobin >7–8 g/dL
• Avoid over-transfusion — excessive transfusion raises portal pressure and can precipitate re-bleeding; target Hb 7–8 g/dL, not normalisation
• Correct coagulopathy if bleeding uncontrolled: FFP 10–15 mL/kg; platelet transfusion if <50,000/µL with active bleeding
• Monitor: urine output (catheterise), heart rate, BP, oxygen saturation
Step 2: Pharmacological vasoconstriction (start immediately, before endoscopy)
• Octreotide — somatostatin analogue that causes splanchnic vasoconstriction, reducing portal pressure; give as IV bolus 1–2 µg/kg (max 50 µg), then continuous infusion 1–2 µg/kg/hour for 3–5 days. FIRST-LINE in children (terlipressin approved in adults; octreotide preferred in children due to safety data)
• Terlipressin (vasopressin analogue) — 0.1 mg/kg IV bolus every 4 h; approved for acute variceal bleed; causes systemic and splanchnic vasoconstriction; adverse effects include hyponatraemia, bradycardia, ischaemia
Step 3: Antibiotic prophylaxis
• Ceftriaxone IV (50 mg/kg/day, max 2 g/day) for 5–7 days — reduces risk of bacterial infection (SBP, bacteraemia) which is a major cause of early re-bleeding and mortality in variceal haemorrhage; recommended for ALL children with variceal bleed, even in EHPVO
Step 4: Endoscopic therapy (within 12–24 hours of stabilisation)
• Endoscopic variceal band ligation (EVL) — the preferred technique; elastic bands are placed at the base of each varix, causing strangulation and obliteration; preferred over injection sclerotherapy in most centres due to lower complication rates
• Endoscopic injection sclerotherapy (EIS) — injection of sclerosant (sodium tetradecyl sulphate, ethanolamine) into or alongside the varix; used when band ligation is technically difficult (young children, small varix)
Step 5: Rescue therapy for uncontrolled bleed
• Sengstaken-Blakemore tube (SBT) — balloon tamponade; oesophageal and gastric balloons are inflated to compress the varices mechanically; used as a BRIDGE to definitive therapy when endoscopic control has failed, not as definitive treatment. Maximum 24 hours. Complications: aspiration, oesophageal rupture.
• TIPS (Transjugular Intrahepatic Portosystemic Shunt) — radiologically placed shunt between portal and hepatic vein within the liver parenchyma; reduces portal pressure dramatically; used in adults as rescue therapy; technically feasible in older children
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
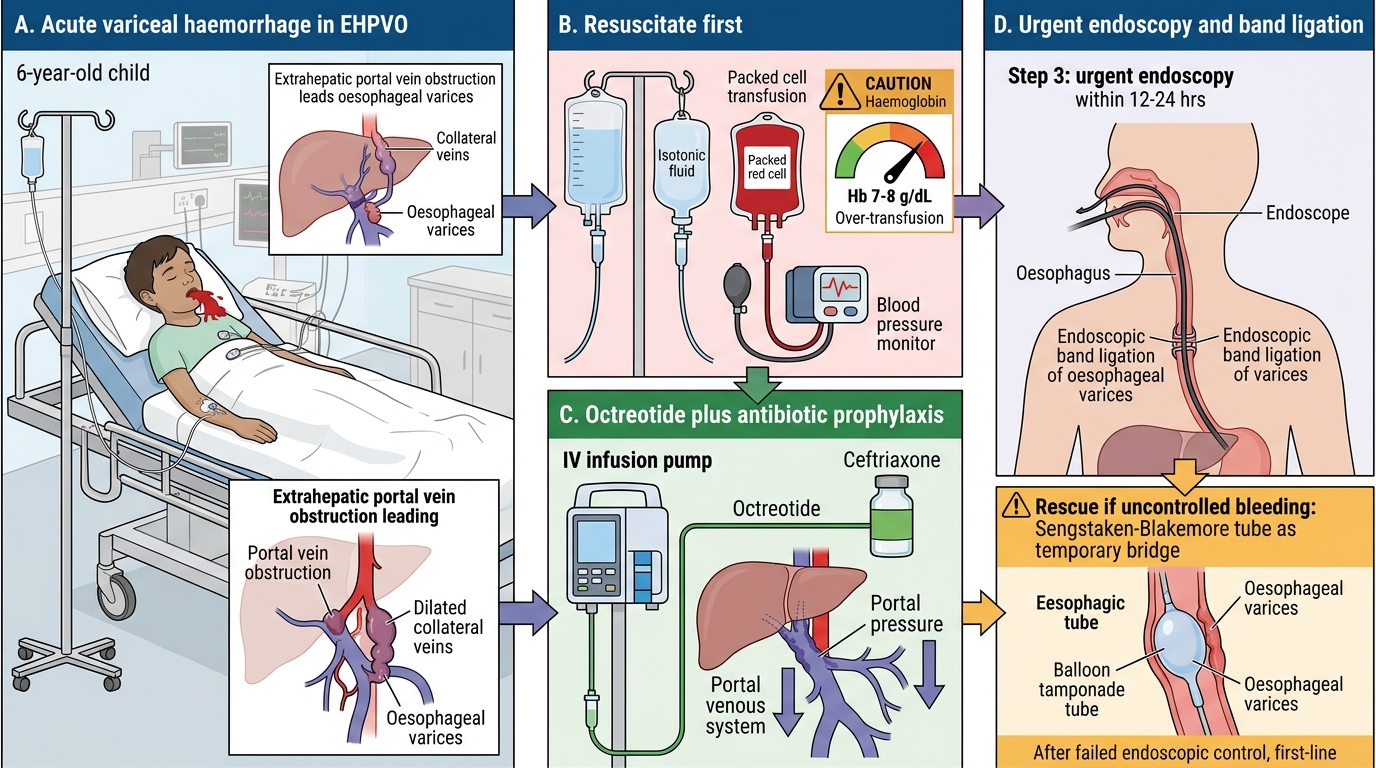
Emergency Management of Acute Variceal Haemorrhage in Children
SELF-CHECK
A 6-year-old with EHPVO is in the emergency department with active haematemesis. IV access has been established. What is the CORRECT order of the next three interventions?
A. Endoscopy → octreotide → blood transfusion
B. Blood transfusion (avoid over-transfusion, target Hb 7-8) → octreotide IV → urgent endoscopy within 12-24h
C. Octreotide → Sengstaken-Blakemore tube → blood transfusion
D. Liver biopsy to confirm EHPVO → endoscopy → blood transfusion
Reveal Answer
Answer: B. Blood transfusion (avoid over-transfusion, target Hb 7-8) → octreotide IV → urgent endoscopy within 12-24h
The correct sequence for acute variceal bleed is: (1) Resuscitate — IV fluids and blood transfusion to haemodynamic stability, but DO NOT over-transfuse (target Hb 7-8, not higher, as over-transfusion raises portal pressure); (2) Start octreotide immediately (pharmacological reduction of portal pressure, given before endoscopy); (3) Urgent endoscopy within 12-24 hours for definitive haemostasis by band ligation. Sengstaken-Blakemore is rescue therapy for uncontrolled bleeding after endoscopy fails, not a first step. Liver biopsy is NOT indicated acutely in EHPVO (liver is normal). Ceftriaxone for antibiotic prophylaxis should also be started at the same time as resuscitation.
Management: Chronic PHT and Prevention
After the acute variceal bleed has been controlled, the focus shifts to two equally important long-term goals: secondary prophylaxis (preventing re-bleeding, which occurs in up to 70% of children without treatment) and management of the chronic complications of portal hypertension including splenomegaly, hypersplenism, and ascites in cirrhotic cases. Re-bleeding after the index variceal haemorrhage is most likely in the first 6 weeks; without any prophylaxis, most children with large varices will rebleed within 1–2 years. The two pillars of secondary prophylaxis are pharmacological reduction of portal pressure (non-selective beta-blockers, specifically propranolol) and endoscopic variceal eradication by a planned, structured programme of band ligation sessions spaced every 2–4 weeks. In EHPVO specifically, the Rex shunt (meso-Rex bypass) represents a landmark surgical advance that transcends both of these measures — it restores physiological portal flow to the liver, permanently eliminating variceal pressure rather than managing its consequences, and does so without requiring a liver transplant or portosystemic shunt that carries encephalopathy risk.
Secondary prophylaxis after variceal bleed:
• Endoscopic variceal band ligation (EVL) programme — repeat sessions every 2–4 weeks until all oesophageal varices are eradicated (typically 3–6 sessions); then surveillance endoscopy every 6–12 months
• Non-selective beta-blockers (propranolol) — reduce cardiac output and cause splanchnic vasoconstriction, lowering portal pressure; dose: 1–3 mg/kg/day in 2 divided doses; titrate to achieve 25% reduction in resting heart rate. Used as adjunct to EVL or where EVL is not available. Not recommended as sole primary prophylaxis in children (NASPGHAN guidelines)
Rex shunt (Meso-Rex bypass) — specific to EHPVO:
• Surgical anastomosis between the left branch of the portal vein (which is patent intrahepatic, even in EHPVO) and the superior mesenteric vein, using an autologous jugular vein graft — bypasses the blocked extrahepatic portal vein and restores normal portal flow to the liver
• Advantages: restores physiological portal flow, reduces portal pressure permanently, resolves splenomegaly and hypersplenism, eliminates variceal re-bleeding risk, and — crucially — allows normal liver growth and function without portosystemic encephalopathy (since blood reaches the liver physiologically)
• Indication: EHPVO with patent intrahepatic left portal vein (confirmed by MRI/MRA); considered the preferred definitive therapy for suitable EHPVO patients in experienced paediatric hepatology centres
• Requires pre-operative MRA portal mapping to confirm left portal vein patency
Conventional portosystemic shunts (for children not suitable for Rex shunt):
• Distal splenorenal shunt (Warren shunt) — decompresses the splenorenal territory selectively while preserving portal hepatic flow partially; reduces encephalopathy risk vs total shunts
• Mesocaval shunt — joins superior mesenteric vein to IVC; used when Rex shunt not feasible
• Portosystemic shunts carry a risk of hepatic encephalopathy (portal blood bypasses the liver entirely) — this risk is much lower in EHPVO (where liver detoxification is normal) than in cirrhotic PHT
Ascites management (cirrhotic PHT):
• Sodium restriction (1–2 mEq/kg/day)
• Spironolactone (3–5 mg/kg/day in divided doses) — aldosterone antagonist, first-line diuretic for ascites
• Furosemide — add if spironolactone alone insufficient (ratio 5:2 spironolactone:furosemide to maintain normokaliaemia)
• Therapeutic paracentesis (with albumin infusion) for tense refractory ascites
• Spontaneous bacterial peritonitis (SBP) — diagnose by ascitic fluid PMN >250 cells/µL; treat with ceftriaxone IV 5–7 days; long-term norfloxacin prophylaxis after first episode
Primary prophylaxis (before first bleed):
• In children with confirmed large varices on surveillance endoscopy, primary prophylaxis with EVL (endoscopic variceal ligation) is recommended — prevents the first bleed in high-risk varices (Grade III–IV)
Self-Assessment: Portal Hypertension
Test your understanding with these clinical scenarios.
Scenario 1: An 8-year-old boy presents with haematemesis. He has massive splenomegaly, completely normal LFTs, and Doppler USG shows absence of the main portal vein replaced by collaterals at the hepatic hilum. What is the diagnosis, and outline your management of the acute bleed?
Key answer points: EHPVO with oesophageal variceal bleed. Management: IV access + resuscitation (RL/NS bolus, PRBC to Hb ≥7 g/dL — avoid over-transfusion), IV octreotide (1–2 µg/kg bolus then infusion), IV ceftriaxone (antibiotic prophylaxis), urgent OGD within 12–24h for band ligation. After stabilisation: plan EVL programme for secondary prophylaxis; refer for Rex shunt assessment (MRI/MRA portal mapping).
Scenario 2: A 13-year-old girl with known biliary atresia (status post-Kasai at 8 weeks) presents with worsening ascites and one episode of haematemesis. LFTs show bilirubin 8 mg/dL, INR 2.1, albumin 2.4 g/dL. What type of PHT does she have, and how does her management differ from EHPVO?
Key answer points: Intrahepatic (cirrhotic) PHT — deranged LFTs, coagulopathy, hypoalbuminaemia, ascites indicate hepatic failure alongside PHT. Management: acute bleed → same resuscitation/octreotide/EVL sequence. But cirrhotic PHT management additionally requires: managing ascites (spironolactone/furosemide), SBP prophylaxis (norfloxacin), managing coagulopathy, and — critically — listing for liver transplant evaluation (PELD score). Rex shunt is NOT suitable for cirrhotic PHT (intrahepatic portal veins are compressed by fibrosis).
Scenario 3: After EVL of oesophageal varices, a 10-year-old with EHPVO is re-evaluated. MRI shows a patent intrahepatic left portal vein. His surgeons propose a Rex shunt. What are the advantages of a Rex shunt over a distal splenorenal shunt for this child?
Key answer points: Rex shunt (meso-Rex bypass) advantages: (1) Restores physiological portal flow to the liver (hepatopetal) → no encephalopathy risk; (2) Allows normal liver growth and function; (3) Resolves splenomegaly and hypersplenism permanently; (4) Eliminates variceal re-bleeding risk definitively. Distal splenorenal shunt (Warren shunt) still diverts some portal blood away from the liver, carries encephalopathy risk, and does not restore physiological flow. Rex shunt is the preferred option when the intrahepatic left portal vein is patent.