Page 13 of 23
PE25.5 | Foreign Body Aspiration — SDL Guide
Learning Objectives
- Describe the types of foreign bodies commonly aspirated by infants and children and the age groups most at risk
- Explain the three clinical phases of foreign body aspiration and recognise each at the bedside
- Justify why the right main bronchus is the most common site of lodgement
- Apply age-appropriate basic life support first-aid manoeuvres for a choking child
- Select appropriate investigations including chest radiography and bronchoscopy for diagnosis
- Describe rigid bronchoscopy as the gold-standard intervention and outline post-procedure care
INSTRUCTIONS
Foreign body aspiration (FBA) is a leading cause of accidental death in children under three years. The silent asymptomatic interval that follows the initial choking episode is a diagnostic trap that leads to dangerous delays. This module equips you to recognise every phase of FBA, perform the correct age-appropriate first-aid manoeuvre, and understand why and when urgent rigid bronchoscopy is life-saving.
References
- Ghai Essential Pediatrics, 9th ed., Ch. 16 — Respiratory Disorders (textbook)
- Nelson Textbook of Pediatrics, 21st ed., Ch. 418 — Foreign Bodies in the Airway (textbook)
- IAP Guidelines on Pediatric Airway Emergencies (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 14-month-old boy is brought to casualty by his mother after she found him playing with roasted peanuts on the kitchen floor. She reports he suddenly turned blue, coughed violently for about a minute, and then — strangely — seemed to settle down and appears almost normal now. Physical examination shows mildly decreased breath sounds on the right side. A chest X-ray taken in full inspiration looks nearly normal. The casualty medical officer reassures the family that the child is fine and proposes discharge. Is this child safe to go home?
WHY THIS MATTERS
Foreign body aspiration is one of the commonest preventable causes of death in toddlers worldwide and a significant public-health concern in India, where children have easy access to small food items such as peanuts, seeds, coins, and hard candies. The deceptive asymptomatic phase that often follows the initial choking episode is the key reason children arrive late or are sent home inappropriately, only to return with life-threatening obstructive pneumonitis or lobar collapse days later. As a clinician, your ability to maintain diagnostic suspicion even when the child appears well, to perform age-correct first-aid manoeuvres, and to arrange timely bronchoscopy is directly life-saving.
RECALL
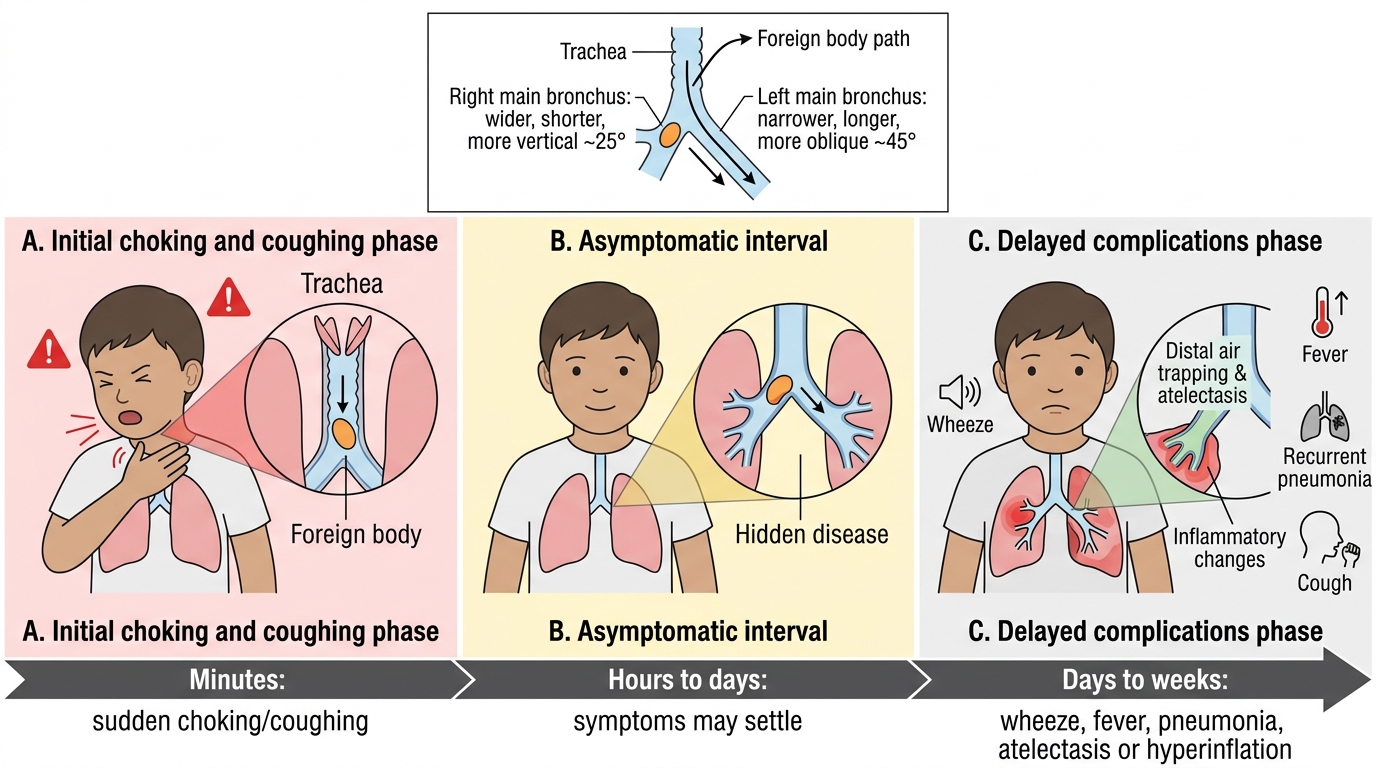
Bring to mind the anatomy of the tracheobronchial tree from your Anatomy studies: the trachea bifurcates at the carina (T4–T5) into the right and left main bronchi. The right main bronchus is shorter, wider, and takes off at a smaller angle from the trachea (approximately 25°) compared to the left (approximately 45°), making it a straighter continuation of the tracheal axis. Recall also from your Physiology studies that infants and toddlers have a relatively small airway cross-section; any reduction in calibre disproportionately increases resistance (Poiseuille's law: resistance is inversely proportional to the fourth power of radius). These anatomical and physiological facts underpin almost everything you will learn in this module.
Clinical Presentation of Foreign Body Aspiration
Foreign body aspiration classically progresses through three sequential phases, and recognising which phase a child is in determines the urgency and direction of management. The initial choking phase occurs at the moment of aspiration and is characterised by sudden violent coughing, choking, gagging, stridor, or cyanosis. The child may turn blue and appear terrified. This phase is often witnessed by a caregiver and provides the most critical diagnostic clue in the history. However, because the cough reflex is so forceful and the foreign body may shift to a stable position in a bronchus, this phase typically resolves within seconds to minutes — which leads directly into the dangerous second phase.
The asymptomatic interval that follows is perhaps the most important clinical concept in FBA. The child appears remarkably well, breathes relatively comfortably, and the family — and sometimes the clinician — is falsely reassured. This interval can last from hours to days, and it is the period during which most diagnostic errors and dangerous discharges occur. Even during this phase, careful auscultation may reveal subtle unilateral decreased breath sounds or a faint wheeze on the affected side.
The delayed or complication phase develops when the foreign body — particularly organic material such as peanuts or seeds — causes progressive mucosal inflammation, oedema, and obstruction. Complications include obstructive emphysema (air-trapping distal to the FB), atelectasis, recurrent pneumonia, lung abscess, and bronchiectasis. Children in this phase often present with fever, productive cough, and respiratory distress that is mistakenly attributed to a lower respiratory infection. A history of a witnessed choking episode weeks earlier is the key to unmasking the true aetiology.
The peak age for FBA is 6 months to 3 years. At this developmental stage, children are highly orally exploratory (putting everything in the mouth), their molars are not yet fully erupted making chewing of hard foods inefficient, and their laryngeal protective reflexes are still maturing. Common foreign bodies include food items (peanuts, groundnuts, seeds, hard candies, grapes, hot-dog pieces) and non-food items (coins, small toy parts, button batteries, safety pins).
IMPORTANT NOTE: Button battery aspiration and impaction is a separate emergency requiring even faster intervention because the electrical current causes liquefactive necrosis within 2 hours.
Clinical Phases of Foreign Body Aspiration
Pathophysiology and Anatomical Basis
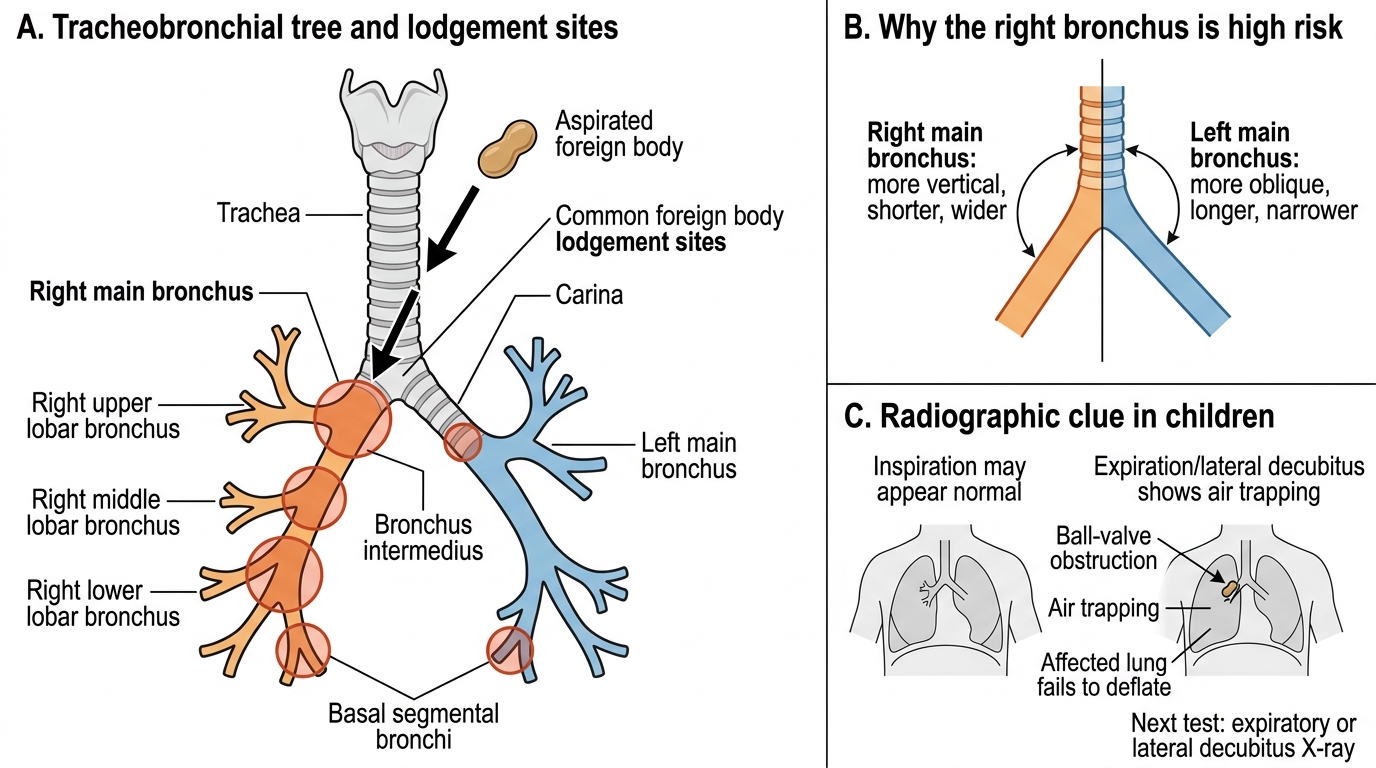
The anatomical predisposition of the right main bronchus to receive aspirated foreign bodies is explained by two structural differences from the left. First, the right main bronchus departs from the trachea at a smaller angle (approximately 25° from the vertical axis) compared to the left (approximately 45°), making it essentially a straight continuation of the trachea. Second, the right main bronchus is wider in calibre and shorter in length. Together, these features mean that when a foreign body descends beyond the cords — propelled by the flow of inspired air — it is carried preferentially into the right bronchus by both gravity and airflow momentum. This rule is most pronounced in older children who are upright; in infants lying supine, the distribution may be more equal.
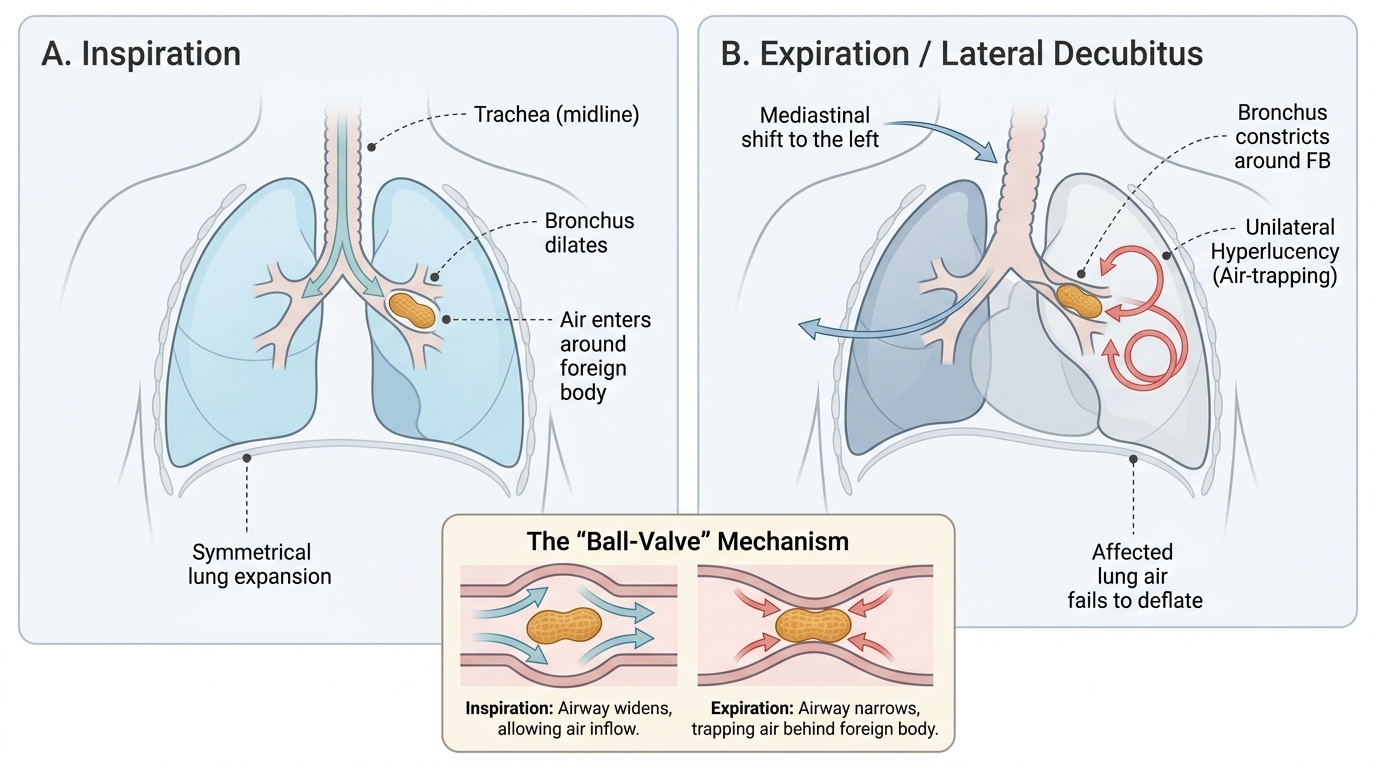
Once lodged in a bronchus, the foreign body produces one of three obstructive patterns depending on the degree of luminal narrowing. A bypass lesion (partial obstruction) allows airflow in both directions and may produce wheeze but little radiological change. A ball-valve or check-valve lesion (the most radiologically detectable pattern) allows air to enter on inspiration — when the bronchus dilates — but not to exit on expiration — when the bronchus constricts around the FB. The result is progressive air-trapping and unilateral hyperinflation (obstructive emphysema) of the affected lobe or lung. A stop-valve lesion (complete obstruction) prevents airflow in either direction and leads rapidly to atelectasis or lobar collapse as trapped air is absorbed.
The nature of the foreign body itself profoundly influences the tempo of the reaction. Inorganic foreign bodies (coins, plastic) cause primarily mechanical obstruction and may remain in place for weeks with relatively mild mucosal reaction. Organic foreign bodies — especially nuts and seeds — release fatty acids that trigger an intense inflammatory mucosal reaction called vegetable bronchitis or lipoid pneumonia, with rapid development of oedema, granulation tissue, and secondary infection. This inflammatory reaction narrows the airway further, making bronchoscopic removal more technically challenging if delayed beyond 24–48 hours.
Foreign Body Aspiration in the Tracheobronchial Tree
SELF-CHECK
A 2-year-old child aspirates a peanut. Three hours later, a chest X-ray taken in full inspiration appears normal. What should be the next diagnostic step?
A. Reassure and discharge — normal X-ray excludes significant aspiration
B. Obtain an expiratory or lateral decubitus chest X-ray to look for air-trapping
C. Arrange CT chest immediately as the gold standard
D. Start antibiotics empirically for pneumonia and observe
Reveal Answer
Answer: B. Obtain an expiratory or lateral decubitus chest X-ray to look for air-trapping
An inspiratory X-ray may appear normal in up to 30% of bronchial foreign bodies because the ball-valve effect is most apparent when the child is exhaling. An expiratory film (or lateral decubitus with the suspected side down, which produces a similar effect by gravity) will demonstrate unilateral hyperinflation or failure of the affected lung to deflate — the cardinal radiological sign of a bronchial foreign body. CT is not needed before bronchoscopy and adds radiation. Empirical antibiotics miss the diagnosis. Discharge with a normal X-ray when the history is suspicious is the single most dangerous error in FBA.
Diagnosis and Investigations
The diagnosis of foreign body aspiration rests primarily on a detailed, targeted history — specifically, whether a witnessed choking episode occurred, the nature of any foreign body the child may have had access to, and the timeline from the episode to presentation. A high index of suspicion must be maintained even when the child appears well in the asymptomatic phase. Physical examination may reveal unilateral decreased breath sounds, a localised wheeze, or reduced chest expansion on the affected side, but may also be entirely normal in the early asymptomatic interval.
Provided image
Plain chest radiography is the first investigation of choice. However, most foreign bodies aspirated by children are radiolucent (peanuts, seeds, soft plastic), so they will not be directly visible. The indirect radiological signs of FBA are therefore critical to recognise:
• Inspiratory film: may appear normal, or may show mediastinal shift away from an over-inflated hemithorax (ball-valve effect), or lobar collapse (complete obstruction).
• Expiratory film or lateral decubitus film (affected side down): the affected lung fails to deflate and appears hyperinflated relative to the normal side — the most reliable plain radiological sign of a bronchial FB. In a cooperative child, both inspiratory and expiratory films should be obtained. In a non-cooperative toddler, bilateral lateral decubitus films (each side in turn) are the practical alternative.
• Radiopaque FBs (coins, batteries, metal) are directly visible. A coin in the trachea lies in the coronal plane (seen as a disc on AP view), while a coin in the oesophagus lies in the sagittal plane (seen edge-on on AP view).
Fluoroscopy allows real-time observation of respiratory-phase mediastinal shift and diaphragmatic movement asymmetry, which is particularly useful for demonstrating ball-valve physiology without the need for expiratory-phase cooperation.
Rigid bronchoscopy is both the definitive diagnostic and therapeutic procedure and is performed under general anaesthesia in the operating theatre. It provides superior optics, a larger working channel than flexible bronchoscopy, the ability to ventilate the patient during the procedure, and a range of rigid forceps for grasping different FB shapes. Flexible bronchoscopy has a role in diagnosis and in selected cases of distal or peripheral FBs where the rigid scope cannot reach, but it is NOT the primary instrument for initial FB removal in most paediatric centres. CT chest is reserved for complex delayed presentations or to delineate complications such as abscess.
CLINICAL PEARL
The most dangerous moment in managing a child with suspected foreign body aspiration is when the X-ray looks normal and the child appears well — this is the asymptomatic interval. Never discharge a child with a convincing choking history on the basis of a normal inspiratory chest X-ray alone. Obtain an expiratory or lateral decubitus film. If the history is strongly suggestive and both films are inconclusive, proceed to rigid bronchoscopy: a negative scope is far safer than a missed foreign body left to cause obstructive pneumonitis or complete airway occlusion.