Page 14 of 23
PE25.5 | Foreign Body Aspiration — SDL Guide (Part 2)
Management: First Aid and Definitive Treatment
The management of foreign body aspiration has two distinct phases: immediate first aid at the scene to relieve acute obstruction, and definitive hospital-based treatment to retrieve the foreign body and address complications. The single most important principle in immediate management is that the technique you use must be matched to the child's age, because an intervention appropriate for a school-age child can cause serious internal injury if applied to an infant. This age-specificity is not merely a theoretical point — it is the basis of resuscitation guidelines and a high-yield examination topic. Understanding why each technique works, and which anatomical constraint makes a technique dangerous in younger age groups, is what allows you to recall and apply the correct manoeuvre under pressure in a real emergency.
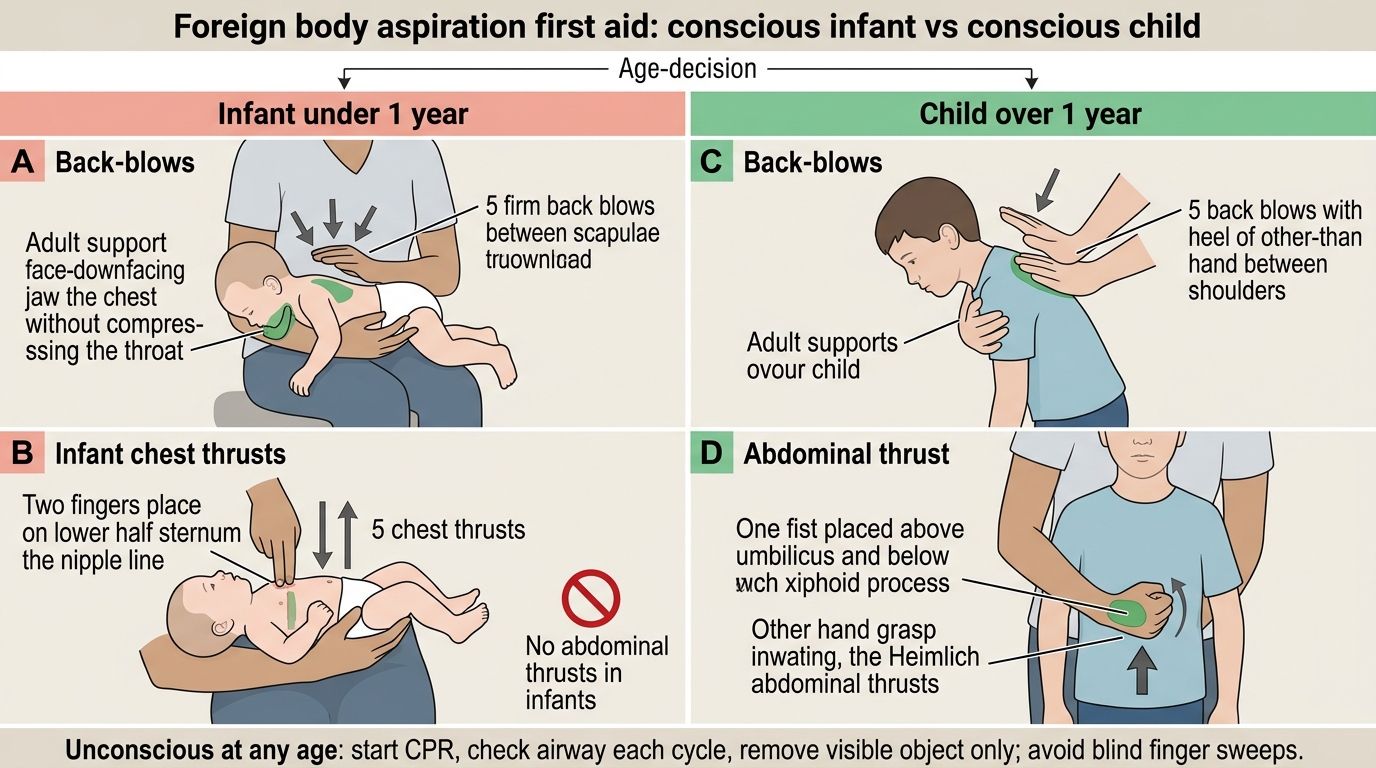
IMMEDIATE FIRST AID — age-appropriate technique is critical:
For an infant under 1 year of age, the correct BLS sequence is:
1. Support the infant face-down along the forearm (head lower than chest)
2. Deliver 5 firm back-blows between the shoulder blades using the heel of the hand
3. Turn the infant supine, support the head
4. Deliver 5 chest thrusts using two fingers on the lower sternum (as for CPR compressions but sharper and more deliberate)
5. Check the mouth between cycles and remove any visible object
6. Repeat the cycle if obstruction persists
Abdominal thrusts (Heimlich manoeuvre) must NOT be used in infants under 1 year because the liver is relatively large and unprotected and abdominal thrusts risk hepatic laceration and visceral injury.
For a conscious child over 1 year of age, the correct BLS sequence is:
1. Deliver 5 back-blows with the heel of the hand between the shoulder blades
2. If unsuccessful, deliver 5 abdominal thrusts (Heimlich manoeuvre): stand behind the child, make a fist with one hand, position it just above the navel and below the xiphisternum, grasp with the other hand, and thrust sharply inward and upward
3. Alternate 5 back-blows and 5 abdominal thrusts until the object is expelled
4. If the child becomes unconscious, begin CPR — each time the airway is opened for rescue breaths, check for the foreign body and remove if visible
For a complete obstruction with unconscious child of any age, commence CPR and summon emergency services immediately.
DEFINITIVE HOSPITAL TREATMENT:
Once the child reaches hospital, the priority is to confirm the diagnosis and arrange rigid bronchoscopy under general anaesthesia in an operating theatre equipped for paediatric airway management. This should not be delayed, particularly for organic FBs where the inflammatory reaction worsens with time. The anaesthetist maintains spontaneous ventilation where possible to avoid pushing the FB distally.
Post-procedure, the child is monitored for residual complications: post-obstructive pneumonia, laryngeal oedema, pneumothorax from procedural trauma, and hypoxaemia. Chest physiotherapy helps clear secretions. If pneumonia is established, appropriate antibiotic therapy is initiated. Complications of delayed diagnosis — such as bronchiectasis, chronic atelectasis, or lung abscess — may require surgical management (segmentectomy or lobectomy) in rare cases.
Prevention is the most effective strategy: parents should be counselled to keep small objects away from children under 3 years, to avoid round firm foods (whole grapes, peanuts, hard candy) for this age group, and to supervise mealtimes.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Foreign Body Aspiration First Aid: Infant and Child Techniques
| Age Group | Technique | Method | What to Avoid |
|---|---|---|---|
| Infant <1 year | 5 back-blows + 5 chest thrusts | Face-down on forearm; two-finger chest compressions | NO abdominal thrusts — risk of hepatic injury |
| Child >1 year (conscious) | 5 back-blows + 5 abdominal thrusts | Heel of hand between shoulder blades; Heimlich above navel | Avoid blind finger sweeps in mouth |
| Any age (unconscious) | CPR + check airway each cycle | Begin chest compressions; remove visible object only | Do not delay CPR to search for FB |
SELF-CHECK
A 10-month-old infant is brought to the emergency room with suspected foreign body aspiration. She is conscious and distressed but still breathing. Which of the following is the correct immediate first-aid sequence?
A. 5 abdominal thrusts followed by 5 back-blows, repeated until FB expelled
B. 5 back-blows followed by 5 chest thrusts, repeated until FB expelled
C. Immediate rigid bronchoscopy without first aid
D. 5 back-blows alone — chest thrusts are only for adults
Reveal Answer
Answer: B. 5 back-blows followed by 5 chest thrusts, repeated until FB expelled
For an infant under 1 year of age, the correct sequence is 5 back-blows (face-down, head lower than body) followed by 5 chest thrusts (two fingers on lower sternum, not the upper abdomen). Abdominal thrusts are CONTRAINDICATED in infants because the proportionally large liver is at risk of laceration. This is a PE known-trap and a frequently examined point. Immediate bronchoscopy without attempting first aid would be inappropriate for a stable, breathing infant. Back-blows alone without the chest-thrust component are insufficient.
Self-Assessment
Use these structured questions to consolidate your understanding of the key concepts in this module before moving to the assessments. Self-directed review is most effective when you attempt to answer each question from memory first, then cross-check against the module content. Pay particular attention to the age-based first-aid distinction (the most commonly examined trap), the radiological logic behind requesting an expiratory or lateral decubitus film, and the significance of the asymptomatic interval in the history. If you can explain the ball-valve mechanism in plain language and derive the management algorithm from anatomical and physiological principles rather than rote memorisation, you have achieved the depth of understanding this module requires. Attempt the questions below before reviewing the answers.
Anatomy & Pathophysiology:
• Why is the right main bronchus the more common site of FB lodgement compared to the left?
• Describe the ball-valve mechanism and explain which radiological finding it produces.
• Why do organic foreign bodies (e.g. peanuts) produce a more severe and rapid inflammatory reaction than inorganic ones?
Clinical recognition:
• A child presents with a 3-day history of right-sided wheeze and fever. The mother recalls a choking episode on seeds 3 weeks earlier, attributed to 'going down the wrong way.' What diagnosis must you consider? What late complication has likely developed?
• What single feature in a history should keep foreign body aspiration on your differential even in the delayed phase?
Management:
• Contrast the first-aid management for a 9-month-old infant versus a 2-year-old child with acute choking.
• When is rigid bronchoscopy indicated, and why is it preferred over flexible bronchoscopy for initial FB removal?
• What post-procedure complications should you watch for after rigid bronchoscopy for FB removal?